Article Text

Abstract
Objectives In part 1, the objective was to undertake a systematic scoping review of applied sports science and sports medicine in women’s rugby, and in part 2 to develop a consensus statement on future research priorities.
Design In part 1, a systematic search of PubMed (MEDLINE), Scopus and SPORTDiscus (EBSCOhost) was undertaken from the earliest records to January 2021. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020, the PRISMA extension for Scoping Reviews, and the PRISMA extension protocols were followed. In part 2, 31 international experts in women’s rugby (ie, elite players, sports scientists, medical clinicians, sports administrators) participated in a three-round Delphi consensus method. These experts reviewed the findings from part 1 and subsequently provided a list of priority research topics in women’s rugby. Research topics were grouped into expert-based themes and expert-based subthemes via content analysis. Expert-based themes and expert-based subthemes were ranked from very low to very high research priority on a 1–5 Likert scale. Consensus was defined by ≥70% agreement. The median research priority agreement and IQR were calculated for each expert-based theme and subtheme.
Data sources PubMed (MEDLINE), Scopus and SPORTDiscus (EBSCOhost).
Eligibility criteria for selecting studies Studies were eligible for inclusion if they investigated applied sports science or sports medicine in women’s rugby.
Results In part 1, the systematic scoping review identified 123 studies, which were categorised into six sports science and sports medicine evidence-based themes: injury (n=48), physical performance (n=32), match characteristics (n=26), fatigue and recovery (n=6), nutrition (n=6), and psychology (n=5). In part 2, the Delphi method resulted in three expert-based themes achieving consensus on future research priority in women’s rugby: injury (5.0 (1.0)), female health (4.0 (1.0)) and physical performance (4.0 (1.0)).
Summary/Conclusion This two-part systematic scoping review and Delphi consensus is the first study to summarise the applied sports science and sports medicine evidence base in women’s rugby and establish future research priorities. The summary tables from part 1 provide valuable reference information for researchers and practitioners. The three expert-based themes that achieved consensus in part 2 (injury, female health and physical performance) provide clear direction and guidance on future research priorities in women’s rugby. The findings of this two-part study facilitate efficient and coordinated use of scientific resources towards high-priority research themes relevant to a wide range of stakeholders in women’s rugby.
- women
- female
- rugby
- sport
- sports medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Women’s rugby has grown substantially in global popularity and professionalisation. As women’s rugby continues to grow and develop, it is important to systematically identify and map the volume and nature of research on applied sports science and sports medicine to establish the current evidence base in the scientific literature and future research priorities.
What are the new findings
The scoping review part of this study identified 123 studies investigating applied sports science and sports medicine in women’s rugby. Studies were categorised into six evidence-based themes, with the most researched evidence-based themes identified being injury, physical performance and match characteristics. The summary tables of the applied sports science and sports medicine evidence base provide valuable reference information.
Based on the current evidence base, experts established consensus on three expert-based themes for future research priority: injury, female health and physical performance. The findings of this study guide future research priorities in women’s rugby and have relevance to a wide range of stakeholders (eg, practitioners, coaches, players, researchers and governing bodies).
Introduction
Rugby union, rugby league and rugby sevens are all codes of rugby (rugby codes collectively referred to as ‘rugby’ hereafter). Men and women play rugby at junior, senior, amateur and elite levels.1–3 At the elite level, each team in rugby union, rugby league and rugby sevens matches consists of 15, 13 and 7 players, respectively, on the pitch, with 8, 4 and 5 players, respectively, on the bench as interchanges or substitutions. There are rule variations at lower performance levels (eg, in rugby union, the Rugby Football Union (RFU) has stipulated not more than five replacements and substitutions at levels 3 and 4, and not more than three replacements and substitutions at levels 5 and below).4 Players are broadly categorised into the positional playing groups of forwards or backs.1–3 Specialist positions within the broad positional categories exist for each rugby code.2 3 5 Match duration can vary by country. For example, women’s rugby union and rugby league in England are played over two 40 min halves. In the Australian women’s rugby league domestic competition, each half is 30 min in length, less than the Australian women’s rugby union competition and the domestic women’s rugby league competition in England, which is 40 min per half. Although rugby sevens is played under essentially the same rules as rugby union, it is played over 7 min halves. Rugby sevens is typically played in a tournament-style format, with five to six games played over 2–3 days. Another key difference between the rugby codes is that when the ball leaves the field of play, rugby union and rugby sevens restart with a line-out, whereas rugby league restarts with a scrum. Additionally, following a tackle, in rugby union and rugby sevens, players can contest the ball via ruck or maul, whereas rugby league requires a play-the-ball. In rugby union, a ruck involves one or more players from each team, close around the ball, which is on the ground, while a maul consists of a ball carrier and at least one player from each team, bound together and on their feet.6 In rugby league, a play-the-ball is the act of bringing the ball into play after a tackle.7
Women’s rugby has grown substantially in global popularity and professionalisation. In the 2016 Rio Olympics, men’s and women’s rugby sevens were introduced, which helped increase the spotlight on women’s game.8 Internationally, women’s rugby union participation increased by 28% from 2017 to 2019, resulting in 2.7 million registered players.9 Major investment into women’s rugby in England was seen in 2017 with the introduction of top-tier competitions (RFU: Premier 15s; Rugby Football League: Women’s Super League), supporting the growth and profile of women’s rugby. In 2019, the England senior women’s rugby union squad became the world’s first professional women’s rugby union team when the RFU awarded 28 full-time playing contracts ahead of the women’s Six Nations Championship.10 This is in contrast to men’s rugby union, which went professional in 1995.11
Alongside the global growth in women’s rugby, recent systematic reviews of the emerging evidence base in women’s rugby have been provided on injury,12 match demands and physical characteristics13 for specific rugby codes. These reviews are limited to a single rugby code or research theme. Similarities exist between rugby codes (ie, physiologically demanding intermittent contact sports that involve high-intensity actions (eg, tackling, sprinting) interspersed with low-intensity actions (eg, walking))2 14 15 in comparison with non-contact sports. Therefore, it is important to collate the evidence base within women’s rugby to facilitate cross-code knowledge transfer and collaboration. Identifying and mapping the current research literature within women’s rugby and then highlighting evidence gaps are important to ensure the current evidence base is applied in policy and practice, and the evidence base continues to evolve systematically in areas where limited research exists. A systematic scoping review, by definition, is well suited to achieving these objectives.16 Systematic scoping reviews aim to examine the extent, range and nature of the evidence, summarise findings from a body of knowledge, and identify gaps in the literature to aid planning of future research.16
Once the evidence base is known, it is important to establish research priorities. Developing research priorities facilitates efficient and coordinated use of scientific resources towards meaningful topics and outcomes. Research priorities should be co-constructed by various stakeholders (including the athlete) in women’s rugby to ensure the research has translational impact and benefit.17–22 Previous literature has not included the athlete in the construction of collaborative sports science research.19 Inclusion of the athletes’ views in developing research priorities advances not only previous work19 22 but also ensures relevant player-focused research questions, development of player-friendly information and the translational impact of the research.20 The Delphi technique is well suited to achieving these outcomes as it is a method used to achieve consensus or determine priorities.23 The technique is highly structured and generally uses a panel to rate a series of statements on a defined Likert scale.23 A key strength of this method is that it allows balanced stakeholder participation, which minimises the risk of bias, thus enhancing scientific rigour.23 Therefore, the aims of this study were as follows: in part 1, to undertake a systematic scoping review of applied sports science and sports medicine in women’s rugby; and in part 2, to develop a consensus statement on future research priorities.
Methods
Design
This research follows a two-part study design. Although this study was not registered, the protocol has been previously published.24
Part 1: systematic scoping review of women’s rugby
A systematic scoping review of applied sports science and sports medicine in women’s rugby was performed in line with the updated guideline for reporting systematic reviews (Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020),25 the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews,16 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension.26
Part 2: consensus on future research priorities in women’s rugby
A three-round Delphi consensus method was performed to identify future research priorities.23 27 28 The CREDES (Conducting and Reporting Delphi Studies) guidance was followed.29 This process involved expert stakeholders reviewing findings from part 1 and subsequently providing a list of priority research topics in women’s rugby. Research topics were grouped into expert-based themes and expert-based subthemes via content analysis.30 31 Expert-based themes and subthemes were ranked from very low to very high research priority on a 1–5 Likert scale. Consensus was defined as achieving ≥70% agreement.28 32–34
All participants provided informed consent.
Part 1: systematic scoping review of women’s rugby
Search strategy
To carry out this review, a systematic search of electronic databases (PubMed (MEDLINE), Scopus, SPORTDiscus (EBSCOhost)) was performed from the earliest records to 20 January 2021. Search terms were constructed using previously published sports science and sports medicine reviews as a guide.5 12 35 36 All study designs were included. The search strategy combined women (“female”, “women*”) AND rugby (“rugby”, “rugby league”, “rugby union”, “rugby sevens”), with terms covering topics related to the applied sports science and sports medicine in women’s rugby: “performance” OR “match*” OR “characteristics” OR “peak” OR “game” OR “competition” OR “skill” OR “technical” OR “anthropometric” OR “composition” OR “physical” OR “strength” OR “power” OR “jump” OR “speed” OR “fitness” OR “aerobic” OR “training” OR “qualities” OR “neuro*” OR “muscle damage” OR “fatigue” OR “recovery” OR “nutrition” OR “iron” OR “injury” OR “incidence” OR “psychology” OR “menstrual” OR “period” OR “menses”. Searches were performed in the title and abstract fields. Searches were limited to the English language. The reference lists of selected studies were manually searched for additional eligible papers.
Study selection
After removing duplicates, search results were independently screened by two researchers (OH, SS) against the eligibility criteria. Disagreements were resolved through discussion or via a third researcher (BJ) if required. The title and authors were not masked to the reviewers. Studies were eligible for inclusion if they investigated applied sports science or sports medicine in women’s rugby. Only peer-reviewed original research studies in the English language were included. Studies including both women’s and men’s rugby players were included if data were reported separately for men and women. Studies were excluded in cases where they did not investigate rugby, or they used rugby players as participants but did not investigate applied sports science and/or sports medicine in rugby players. For example, one study37 used women’s university rugby players as participants but the purpose of the investigation was to examine the relationship between the composite Functional Movement Screen and the modified Star Excursion Balance Test scores on agility performance and was therefore excluded. Such studies using women’s rugby players to examine broader concepts have minimal direct application to women’s rugby. Review articles, conference proceedings, editorials, case studies, letters to editors and theses were excluded.
Data charting
The categorisation of studies into evidence-based sports science and sports medicine themes was determined by each study’s primary aims and outcome measures. Similar methods have been used in a recent scoping review.38 When studies investigated multiple themes, they were categorised by the primary theme. Primary themes were determined by the main study aim, as stated in the study and/or by the theme of the journal where the paper was published. Evidence-based theme subcategories were identified where appropriate. Data charting was conducted by one researcher (OH) and confirmed by a second (SS) using a predeveloped charting form,39 which included the general study characteristics (ie, year of publication, geographical location, cohort (rugby code, playing level), sample size) of each study, data relating to participants’ characteristics (eg, age, height, body mass), the aim, outcome measures and key findings.
Data analysis
As the purpose of a scoping review is to map the extent, range and nature of literature and summarise heterogeneous findings, data analysis was not conducted.16 All data are presented as mean±SD unless otherwise stated.
Part 2: consensus on future research priorities in women’s rugby
Delphi technique
Expert panel
A group of 52 international experts on sports science and/or sports medicine in women’s rugby were invited to participate. The invited experts included 27 women and 25 men across (n=6 elite players, n=19 sport scientists, n=17 medical clinicians, n=10 sports administrators). A minimum of 10 experts were required for reliable results.40 41 Including a greater number of experts increases the reliability.40 41 Eligibility criteria were defined as a researcher, professional or elite player with experience and/or affiliation with women’s rugby at the national level or above. Furthermore, for players to be included in the expert panel, they must have met the following criteria: (1) currently play internationally and (2) actively involved in sports science or medicine (eg, PhD (candidate), lecturer, medical doctor). Although the criteria for players may limit the number of included participants, as per sampling guidelines, it enhances the possibility of players drawing clear interpretations from published research studies.42 All participants were recruited via a purposeful sampling technique, which involved selecting knowledgeable individuals with specific experience in women’s rugby.43 Consideration was given to having multiple national governing bodies represented across rugby codes, as well as representation by elite players and practitioners in sports science (eg, researcher, strength and conditioning coach), medicine (eg, chief medical officer, team doctor) or sports administrators (eg, director of women’s rugby, programme manager). This wide array of international experts was included to ensure multiple participant views would be captured, thus enhancing the translational impact and benefit of the research.17 18 21 22
Round 1
In the first round of questioning, the expert panel were asked to read the results from part 1 (online supplemental tables 1–7) to inform them about the current research in women’s rugby. Via the Qualtrics online software (Qualtrics, Provo, USA), experts were then asked to provide a list of priority research topics. Research topics from the first round were grouped, by inductive content analysis,30 31 into expert-based themes and expert-based subthemes. This process has recently been used in both netball36 and women’s football (soccer)38 reviews. It involves an abstraction process whereby expert-based subthemes were given categories to develop expert-based themes.30 31 When the final list of expert-based themes and expert-based subthemes was identified, the list was refined to enhance clarity and remove duplicates and typographical errors. In each round, participants were given 1 week to respond to the questionnaire, with reminder emails sent out to non-responders 2–3 days before the deadline.
Supplemental material
Round 2
As per the inductive content analysis process,30 31 the expert panel received the refined list of expert-based themes and subthemes developed in round 1. The expert panel were then required to (1) rate the research priority of each of the applied sports science and sports medicine expert-based themes and expert-based subthemes from low to high on a 5-point agreement Likert scale (1: very low priority; 2: low priority; 3: medium priority; 4: high priority; 5: very high priority). The expert panel were again provided with an opportunity to include any additional sports science and sports medicine expert-based themes or expert-based subthemes. Experts were given 1 week to respond to the questionnaire. When assessing consensus, Likert scale ratings were combined (ie, low: 1 and 2; medium:3; high: 4 and 5).44 As per previous literature,32–34 consensus was defined as achieving ≥70% agreement.
Round 3
The expert panel was asked to rerate (using the same 5-point Likert scale) the criteria from round 2 that did not reach consensus, including any new themes or subthemes that panel members included in round 2. The expert panel received feedback on round 2 in descriptive statistics (ie, mean priority rating of expert-based themes and expert-based subthemes), which enabled reflection before expressing their final opinion. Experts were given 1 week to provide their final responses to the questionnaire. As the aim of the Delphi consensus method was to ascertain the research priority of all expert-based applied sports science and sports medicine themes and subthemes, no expert-based themes or subthemes were removed on the grounds of low priority. Expert-based themes or subthemes that did not reach consensus after round 3 were not removed as they may be important to some but not all stakeholders. To manage confidentiality and experts discussing their responses during the Delphi process, the names of experts were not disclosed or shared publicly.23
Research priority agreement ratings were obtained separately for each expert-based theme and expert-based subtheme. The median research priority agreement and IQR were calculated for each expert-based theme and subtheme.
Results
Part 1: systematic scoping review of women’s rugby
Search and selection of studies
The database search identified 2417 articles. After removing duplicates (using Mendeley Desktop V.1.19.8) and applying the eligibility criteria, 123 studies remained for inclusion in the scoping review. The flow of articles from identification to inclusion is shown in figure 1.

Flow of articles from identification to inclusion.
General characteristics of the studies
Expert-based sports science and sports medicine themes
The 123 articles included in this systematic scoping review were categorised into six evidence-based sports science and sports medicine themes: injury (n=48, 39%), physical performance (n=32, 26%), match characteristics (n=26, 21%), fatigue and recovery (n=6, 5%), nutrition (n=6, 5%), and psychology (n=5, 4%) (figure 2).

Number of studies per sports science and sports medicine theme.
Rugby codes
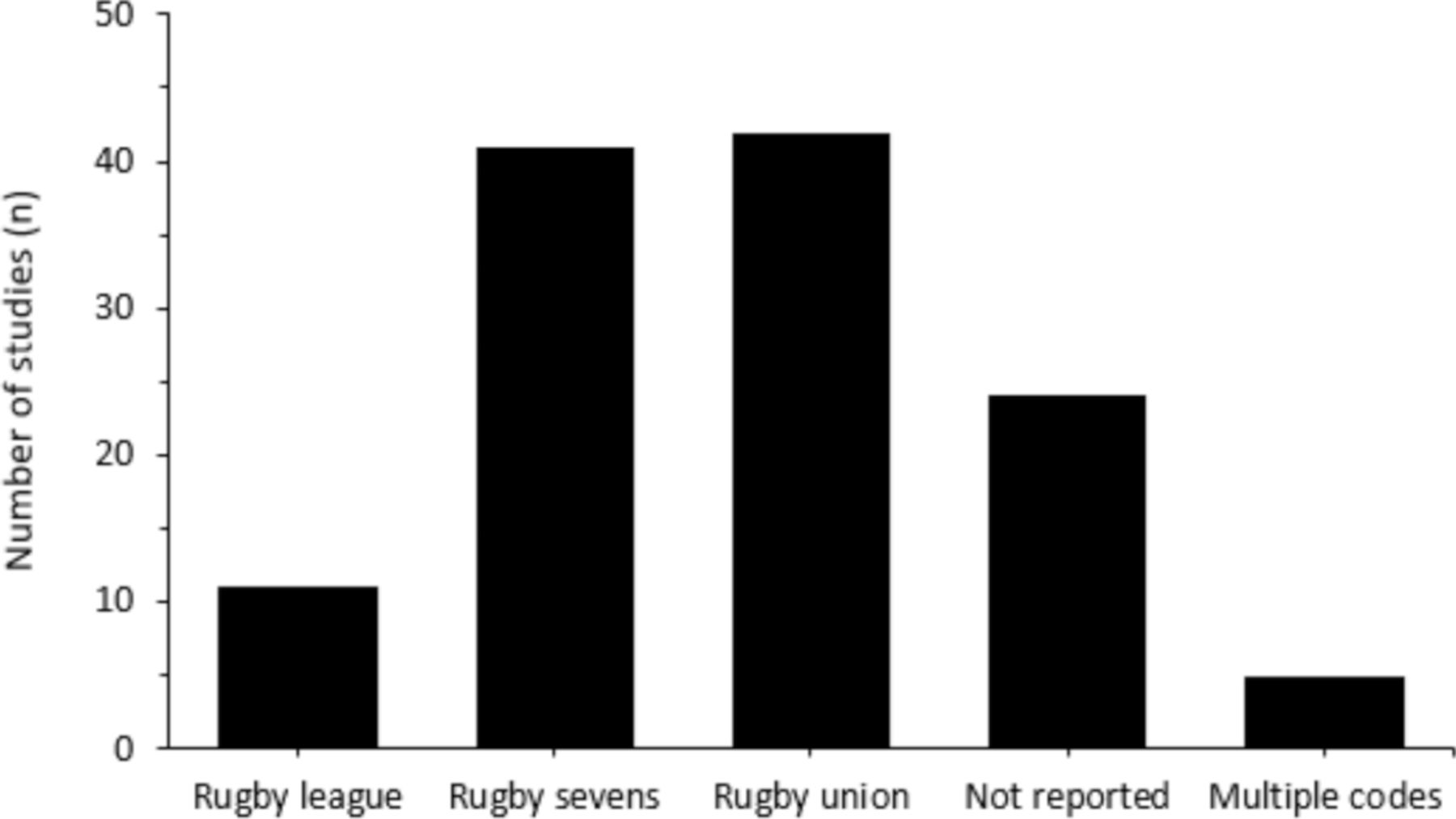
Figure 3 shows the overview of rugby codes that were included in this review: rugby union (n=42, 34%), rugby sevens (n=41, 33%), code not reported (n=24, 20%), rugby league (n=11, 9%) and multiple codes included (n=5, 4%).

{kind=link}
{kind=link}
{kind=link}
Number of studies per rugby code.
Publication year
Table 1 shows the recent rapid growth in published research, with 80% of studies published between 2011 and 2021. Only evidence-based themes of injury and physical performance include studies across all-year group classifications. All studies categorised in fatigue and recovery, match characteristics, nutrition, and psychology evidence-based themes were published between 2011 and 2021.
Period of publication of studies included in the systematic scoping review
Geographical location of the studies
Studies were published in 16 different countries: Australia, Brazil, Canada, France, Hong Kong, Ireland, New Zealand, Norway, Romania, South Africa, Spain, Switzerland, Thailand, The Netherlands, the UK and the USA. The greatest number of studies was from the USA (n=23, 19%), followed by New Zealand (n=18, 15%), Australia (n=17, 14%), Canada (n=17, 14%) and the UK (n=17, 14%). Within the injury evidence-based theme, the greatest number of studies was from the USA (n=13, 27% of 48 studies) and then New Zealand (n=11, 23% of 48 studies). For the physical performance evidence-based theme, the greatest number of studies was from the USA (n=7, 22% of 32 studies) and then the UK (n=6, 19% of 32 studies). Most studies on match characteristics were from Australia (n=8, 31% of 26 studies), Spain and the UK (n=5, 19% of 26 studies for both countries).
Fatigue and recovery
Six studies investigated fatigue and recovery in women’s rugby (online supplemental table 1). All studies were performed in rugby sevens. Two studies (33% of 6 studies)45 46 used both state-level and national-level athletes, while the remaining four studies used either university-level,47 national-level48 or international/elite-level49 50 players. Four studies (66%) investigated the fatigue responses resulting from tournament play.45–47 50 One study49 (16%) quantified core temperature during tournament play and the efficacy of cold water immersion recovery protocols. Another study48 (16%) characterised sleep in team sport athletes.
Studies investigating fatigue responses reported that national-level rugby sevens players displayed smaller performance decrements between tournament days 1 and 2 when compared with state-level players45 and that post-tournament leucocyte count increased similarly (30%–50%) at both playing levels.46 Furthermore, well-being, fatigue, muscle soreness, stress levels, mood and total quality of recovery are impaired after match day 1 and do not return to baseline until 2 days post-tournament.50 Creatine kinase after tournament play has been shown to increase twofold and fourfold in national-level and state-level rugby sevens players, respectively,45 but remain constant in university players.47 Henderson et al49 found that cold water immersion did not entirely remove body heat accumulated during warm-up and match-play in international-level rugby sevens players. Finally, national-level rugby sevens players may suffer poor sleep quality with high levels of associated daytime sleepiness.48
Injury
Epidemiology
Of the 48 studies investigating injury in women’s rugby, 32 (66%) had an injury epidemiology focused theme (online supplemental table 2). These studies included participants from rugby union (n=13, 41% of 32 studies), rugby sevens (n=8, 25%), rugby league (n=3, 9%), a combination of both union and league (n=1, 3%), or the code was not reported (n=7, 22%). The cohorts used in these studies varied widely and included amateur,51–53 high school/junior/U19,54–56 provincial,57 58 collegiate,59 60 collegiate club,61 club,62 Olympic/international/world series63–68 or a combination of levels.69–73 Nine studies (28%) reported injuries to rugby patients/claimants.74–82 The majority of the epidemiological studies (69%) collected data over longer time periods (eg, ≥1 season/year).51–57 59 60 63 68–74 76–82 Some studies collected data during shorter time periods (eg, ≤4 days/tournaments)52 58 64–67 and one study did not report the time course of data collection.62
Multiple approaches to injury definition were taken within the included studies. Many studies (n=17, 53%) used similar definitions to a consensus statement83 on injury definitions in rugby union.51–54 56 57 61 63–67 70–73 84 Ten studies did not report an injury definition.58 62 69 74 75 78–82 Very broad (eg, ‘any physical damage’) or narrow (eg, specific body region) definitions were also used.55 59 60
Studies typically reported injuries per hours of exposure52–57 60 61 63 64 67 68 70 72 or number of players.58 59 69 78 Injury incidence was reported as between 1 and 106 injuries per 1000 exposures.52–57 60 63 64 67 68 71 72 85 The site and/or type of injury were frequently reported. The lower limb53 56 57 60 61 63 64 67 72 77 81 and the head were the most common injury sites in comparison with other injury locations, as identified by the included studies.52 54 57 59 64 72 82 In women’s rugby sevens, lower limb injuries have been reported as the most prevalent injury location, at 63.2% of all injuries at the senior level63 and 38.1% at the U19 level.72 Furthermore, in rugby union, injuries to the knee were the most common, accounting for 40.3% of moderate-to-serious national insurance claims.77 Regarding the knee, in collegiate rugby, ACL injury incidence was reported 5.3 times higher in women compared with men.61 The proportion of head injuries has been reported as 33.3% in amateur rugby sevens,52 23% in rugby-playing patients presenting to emergency departments,82 22.1% in high school rugby union54 and 12.7% in international rugby union.64 Collisions or tackles were typically reported as the cause of injuries.52 54 64 72 74 Tackling has been reported to account for ~74%52 72 and 63.6%64 of injuries in rugby sevens and rugby union, respectively. Injury severity in rugby sevens has been reported as 53.4 days lost in international players68 and 36.7 days lost in regional, collegiate and national players.71 When comparing elite with non-elite rugby sevens players, injury severity has been reported as 74.9 and 41.8 days lost per injury, respectively.72 Injury severity in amateur rugby union has been reported to be as high as 170 days lost per injury for the lower limb.53 Injury severity in international women’s rugby union and junior girls rugby league has been reported as 55 and 13 days lost per injury, respectively.55 67
Risk, management and prediction
Of the 48 studies investigating injury in women’s rugby, 16 (33%) had an injury risk, management and prediction focused theme (online supplemental table 3). These studies included participants from rugby union (n=9, 56% of 16 studies), rugby sevens (n=1, 6%), a combination of union, sevens and league (n=1, 6%), or the code was not reported (n=5, 31%). The cohorts used in these studies varied widely and included amateur/community,86–88 high school,89 rugby schools,90 club,91 university/college,92–95 international,84 or a combination of levels.96–100
Many included studies aimed to determine the relationship between injury and potential risk factors. Some potential risk factors included physical characteristics,86 92 95 concussion history,88 89 wellness,86 demographics,89 foul play100 and Functional Movement Screen scores.93 Concussion was commonly assessed within injury risk, management and prediction studies (44% of 16 studies).84 87–89 91 94 97 These studies provided Sport Concussion Assessment Tool reference values89 and determined whether limits should differ between sexes,84 evaluated standardised assessment and management of concussion,97 investigated the use of the King-Devick Assessment Tool for a sideline concussion assessment,87 investigated the neurological deficits that accompany head impacts,94 explored concussion history on head control,91 and determined the association between concussion and lower limb injury.88
From a concussive symptom standpoint, more symptoms and symptom severity were reported in women’s rugby union players compared with men’s players.84 In high school rugby union, the median symptom severity was also found to be highest in women with concussion history and lowest in men with no concussion history.89 Women have been reported to perform better in orientation, concentration and balance assessments when compared with men.84 Investigations of balance across the duration of a collegiate women’s rugby competitive season have shown reductions in static balance and improvements in dynamic balance at postseason testing.94 Significant associations between concussion and lower extremity musculoskeletal injury have been reported in women’s community rugby union players (OR=2.49).88 Furthermore, women’s senior club-level players with concussion history have been shown to exhibit greater head accelerations and reduced trapezius and splenius capitis electromyography amplitudes.91 When returning to sport after a concussion in rugby, postconcussive syndrome has been shown to last longer in women than men (median number of days: 15 vs 4).97 A delay in women’s return to sport was also found compared with men (30 days vs 21 days; p=0.19).97 For concussion assessment, the King-Devick test has shown good to excellent reliability for baseline (intraclass correlation coefficient (ICC): 0.84–0.89), postinjury (concussion) sideline screening (ICC: 0.82–0.97) and postseason evaluation (ICC: 0.79–0.83).87
Match characteristics
Physical match characteristics
Of the 26 studies investigating match characteristics in women’s rugby, 21 (81%) had a physical demands focused theme (online supplemental table 4). These studies investigated rugby sevens (n=11, 52% of 21 studies), rugby union (n=5, 24%) or rugby league (n=5, 24%). Many of these studies used an international/elite/professional cohort (n=12, 57%).101–112 Other cohorts used included provincial,113 collegiate,114 domestic,115 premier division116 117 or a combination of levels.118–121 Sixteen of the 21 studies (76%) investigating physical characteristics within the match-play theme sampled ≤10 matches (online supplemental table 4).
The mean total distance covered during match-play was typically reported. The mean whole-match total distance covered was reported as 4982–5820 m in rugby union,109 110 113 116 4680–6582 m in rugby league103 121 and ~1416–1642 m in rugby sevens.104–107 112 118–120 Maximum velocity and ‘high-speed’ distance were also typically reported. Peak demands over various epochs (1–10 min) were quantified in two studies.110 121 The average speed demands of international women’s rugby league backs and forwards peaked at 144 m/min over a 1 min epoch.121 In international women’s rugby union, the 1 min average speed demands were 150 m/min for forwards and 157 m/min for backs.110 Comparisons between international and domestic locomotor characteristics during women’s rugby league match-play found that generally the demands were greater for international competition (eg, 241±146 m vs 190±156 m high-speed distance in international and domestic backs, respectively).121 Collisions or impacts were assessed in five studies.101 111 114 115 117 Two studies investigated the ability of Global Positioning Systems to detect collisions compared with video-coded analysis101 111 and found precision to be ~72%–83% in women’s rugby league and that 62% of rugby sevens collisions were incorrectly labelled. Two studies quantified head impacts over one competitive season.114 115 These studies found the mean number of head impacts per player per match to be 0.4–14. In domestic women’s rugby league, the median peak linear acceleration >10 g was reported as 15 g (25th–75th, IQR=12–21).115 One study quantified movement patterns through time-motion analysis and assessed physical demands during premier division rugby union competition and found that backs, when compared with forwards, spent more time sprinting (37±12 min vs 25±16 min) and less time in scrums, rucks, mauls and tackles (25±11 min vs 61±12 min).117
Technical-tactical match characteristics
Of the 26 studies investigating match characteristics in women’s rugby, 5 (22%) had a technical-tactical focused theme (online supplemental table 5). These studies included participants from rugby sevens (n=4, 80% of 5 studies)122–125 and rugby union (20%).126 All these studies were performed in an international cohort.
Studies investigating the technical-tactical characteristics of international women’s rugby sevens match-play found that successful teams gained more possession from handling turnovers, used more quick line-outs, threw more passes, made more ball-jolting tackles124 and had a higher percentage of positive phases122 compared with unsuccessful teams. In international women’s rugby union, winning teams achieved a greater amount of line breaks, higher tackle completion, fewer pick and go’s and fewer rucks in the opposition 22–50 m126 when compared with unsuccessful teams. In rugby sevens ruck situations, when attacking players arrived first, there was a greater chance of maintaining possession.123 Additionally, one study investigated the effects of caffeine on technical performance in international rugby sevens and found no effects on any rugby-specific actions.125
Nutrition
Six studies investigated nutrition in women’s rugby (online supplemental table 7). Three of these studies were performed in rugby sevens (50% of 6 studies),127–129 one in rugby league (17%),130 one in rugby union (17%)131 and one did not report the rugby code (17%).132 Four studies used an elite/international cohort,127–130 one study used university athletes131 and one used both professional and amateur players.132 Two studies investigated player hydration status during training130 131 and match-play,130 three studies investigated haematological (specifically iron and vitamin D) status,127–129 and one study investigated dietary supplementation consumption.132
Investigation of hydration status in international women’s rugby league found that on arrival to training and matches, urine osmolality values were indicative of euhydration.130 The mean body mass reduction in university rugby union did not exceed 2% in training.131 This aligns with the findings of Jones and colleagues,130 who found ~0.5% reduction in body mass during both rugby league training and match-play. In international rugby sevens, investigation of haematological status found that 23% of women’s players were classified as iron-deficient (ferritin <30 µg/L).127 The greatest iron deficiency incidence occurred in mid-season (30% of players), but full recovery was evident by the end season.127 Suboptimal iron stores in elite women’s rugby sevens were mirrored in another study, where 29%–35% of players were identified with ferritin <45 µg/L at some stage in the study.129 Women’s rugby sevens players were found to be vitamin D-sufficient.128 Regarding dietary supplementation in a mixed cohort of professionals and amateurs, 25%–43% of women’s players were identified to consume whey protein, sports drinks, caffeine or sports bars.132
Physical performance
Anthropometrics
Of the 32 studies investigating physical performance in women’s rugby, 7 (22%) had an anthropometrical focused theme (online supplemental table 6). Four of these studies included participants from rugby union (57% of 7 studies).133–136 The remaining three studies did not report the rugby code (43%).137–139 These studies included cohorts from university/college,134 138 139 a combination of club and university,133 semiprofessional,137 or elite levels.135 136
One study investigated positional differences in anthropometric characteristics in elite rugby union women’s players and found the sum of eight skinfold thickness (128.2±36.6 mm and 94.4±29.0 mm) and body fat percentage (26.5%±3.1% and 20.8%±3.0%) were greater in forwards compared with backs, respectively.135 In division 1 collegiate rugby union, forwards displayed greater height (167.7±7.2 cm vs 164.5±5.1 cm), body mass (81.5±15.1 kg vs 64.5±7.7 kg) and body fat percentage (28.2%±6.1% vs 21.9±3.7%) relative to backs.134 Body mass investigations, between playing tiers, in elite women’s rugby union found forwards mass increased by 4.8% from 2010 to 2017 (79 kg to 83 kg) in tier 1 nations, with no changes in either tier 2 nations or backs from either tier.136 Mean Q-angle (21.5°), pelvic width (29 cm) and femur length (41 cm) were described in a university-level cohort.138 Compared with athletes of other (non-contact) sports or controls, semiprofessional women’s rugby players had greater body mass, fat-free mass, fat mass and bone mineral density and increased thickness of abdominal musculature.133 137 139
Biomechanics
Of the 32 studies investigating physical performance in women’s rugby, 3 (9%) had a biomechanical focused theme (online supplemental table 6). One of these studies was performed in rugby sevens with an international cohort (33% of 3 studies).140 In comparison, the other two were performed in rugby union (67%) with amateur141 and combined (club and international)142 cohorts. In amateur women’s rugby union, improvements in 5 m and 20 m sprint performance and mechanical properties related to the horizontal power–force–velocity profile were observed over the course of an 8-week sled training intervention.141 In international women’s rugby sevens, asymmetry of running mechanical variables was investigated, and symmetry angle remained mostly constant across all kinetic, kinematic, spring-mass characteristics and horizontal force production variables.140 Finally, machine scrummaging forces were described in club and international rugby union, and women’s peak compressive force was 8.7 kN.142
Performance
Of the 32 studies investigating physical performance in women’s rugby, 13 (41%) had a performance testing focused theme (online supplemental table 6). Six of these studies included participants from rugby union (46% of 13 studies),1 143–147 three were from rugby sevens (23%),148–150 two from rugby league (15%),151 152 one used both rugby union and sevens (8%),153 and one did not report the code (8%).154 These studies included various cohorts including amateur,151 university/college,144 145 147 154 national,146 international143 148–150 152 or a mixed sample.1 153
In women’s rugby union, studies investigating performance testing between positions found that backs were significantly quicker than forwards over 5, 10, 20, 30 and 40 m and in the 505 agility test and also demonstrated greater vertical jump height (44±5 cm vs 38±5 cm) compared with forwards.1 143 146 In both rugby union and rugby sevens,1 148 forwards were found to demonstrate greater initial sprint momentum (eg, 367±20 kg/m/s vs 399±22 kg/m/s)148 compared with backs. In university women’s players, anaerobic power was found to be greater in forwards than backs.154 In rugby union National All-Star Championship players, backs performed better on all running tests (ie, 40-yard speed, 100 m and 300 m speed, bleep test) than forwards.146 Similar findings were reported in senior and schoolgirl rugby union, where backs outperformed forwards on the aerobic shuttle test.1 Significant correlations were observed between total body fat and all fitness variables in international rugby league.152 When sex comparisons were made between female and male youth rugby league players, respectively, one repetition max squat (115±41 kg vs 104±31 kg) and bench press (46±17 kg vs 47±14 kg) were not different.151 In international rugby sevens, women demonstrated lower performances than men in all speed-power assessments and change of direction tasks (effect size=0.61–2.09), except for the zigzag drill, where no significant differences were identified between men and women.149 Additionally, women displayed a lower change of direction deficits in all tests and lower sprint momentum.149 Sprint times with different ball-carrying techniques were assessed in university-level rugby union and 10 m sprint speed was slower for women beginners who were carrying the ball versus not carrying the ball.147 This study did not find a difference in sprint speed for experienced women or men carrying or not carrying the ball.147 Multidirectional ability was specifically examined in two collegiate rugby union studies,144 145 which found vertical jump height correlated with 20 m speed, standing long jump distance correlated with 5 m and 10 m speed and the left-leg 505 performance (r=−0.71 to −0.88) and predicted 0–5 m and left-leg 505 time.144 No correlation was found between the change of direction deficit and sprint times.145 International rugby sevens players with high playing minutes (≥70 min) were older (24±3 years vs 21±4 years), had greater experience in a national training centre (2.4±0.8 years vs 1.7±0.9 years), had faster 1600 m time (375±20 s vs 394±30 s) and greater one repetition max strength (bench press: 68±6 kg vs 62±8 kg; pull-up: 84±8 kg vs 79±5 kg) than athletes who played fewer minutes.150
Physiology
Of the 32 studies investigating physical performance in women’s rugby, 7 (22%) had a physiology focused theme (online supplemental table 6). Three of these studies (43% of 7 studies) were performed in rugby sevens with an international/Olympic cohort.155–157 Of the remaining four studies, the rugby code was not reported, and the cohort was either varsity (14%),158 subelite and elite (14%),159 international (14%)160 or not reported (14%).161
Studies investigated a range of physiological-themed topics. One study investigated the relationships between blood rheology and body composition and found red blood cell aggregability negatively correlated with isometric handgrip and adductor strength (r=−0.58 to −0.50).161 From a women’s health perspective, 93% of international-level athletes reported menstrual cycle-related symptoms. Furthermore, perceived heavy menstrual bleeding was reported by 33% of players, and 67% considered symptoms to impair physical performance.160 Urinary incontinence prevalence has been reported by 54% of varsity players, and as many as 90% of affected players leaked urine during match-play.158 When investigating resting metabolic rate in subelite and elite women’s players, indirect calorimetry-derived measurements have been reported at 1651±167 kcal/day.159 When comparing resting metabolic rate prediction equations with indirect calorimetry, the Cunningham, Ten Haaf and Watson (body mass) values did not differ from measured metabolic rate (p>0.05).159 Two studies investigated physiological and physical variables in rugby sevens155 156 and found that the critical velocity test was correlated with the Yo-Yo Intermittent Recovery Test Level 1 test (r=0.86).155 Furthermore, compared with the mean speed at the second ventilatory threshold (3.5 m/s), the industry-used threshold of 5 m/s underestimated the absolute amount of high-intensity running completed by individual players by up to 30%.156 One final study investigated the relationship between skeletal muscle properties and peak power production capacity in Olympic rugby sevens and found a strong relationship (r=−0.75, 90% CI −0.90 to −0.44) between vastus lateralis contractile properties and power output.157
Training
Of the 32 studies investigating physical performance in women’s rugby, 2 (6%) had a training focused theme (online supplemental table 6). One of these studies used an elite cohort of sevens players (50%),162 while the other used women’s rugby sevens, league and union strength and conditioning coaches (50%).163 One study evaluated countermovement jump performance over 6 weeks of progressively increasing training load and found training load to increase from week 2 to week 6. Analysis of countermovement jump variables indicated diminished neuromuscular function in elite rugby sevens players throughout the training intervention.162 When exploring current physical preparation practices across all rugby codes,163 it was found that physical testing was more commonly performed during preseason (97% of participants) and inseason (86%) phases when compared with off-season (23%). Resistance, cardiovascular, sprint and plyometric training, and recovery sessions were all believed to be important to enhancing performance and were implemented by most participants (≥89%). Physical preparation coaches identified the most frequent unique aspects of consideration in women’s rugby as psychosocial, menstrual cycle and physical differences.163
Psychology
Five studies investigated the psychological aspect of women’s rugby (online supplemental table 7). One of these studies was performed using rugby union athletes (20% of 5 studies),164 one used a combination of rugby union and sevens athletes (20%),165 and the remaining three studies did not report the rugby code (60%).166–168 The investigated cohorts included varsity,168 university,166 international,164 167 or a combination of both collegiate and national levels.165
Studies investigated a range of psychologically themed topics. One study investigated early maladaptive schema elements in international players and identified an average of five per player.167 The most frequent were self-sacrifice (83%) and unrealistic standards/hypercriticism (78%).167 When investigating participant motivation in international rugby union, multifaceted motives were discovered. The four major participation motivation themes identified were (1) getting started with rugby, (2) physical aspects, (3) achievement and success, and (4) on-field and off-field player interactions.164 A study on rugby union and rugby sevens athletes investigated the role of mental toughness during injury and found that those who would play through injury reported higher mental toughness than those who would not.165 When examining avoidance behaviours during a head-on collision course, varsity rugby athletes avoided significantly later than non-athletes.168 One study assessed the four-stage sequence of relationships between coaches’ perceived interpersonal coaching styles and university players’ basic psychological needs, self-determined motives and performance.166 It was found that all basic psychological needs were perceived to be highly fulfilled.
Part 2: consensus on future research priorities in women’s rugby
Expert panel
Fifty-two international experts on women’s rugby were invited to participate. Thirty-one invited experts participated in the study, while the remaining experts did not respond to the invitation. The participating experts represented multiple nations (Australia n=4, Canada n=3, England n=10, France n=1, Ireland n=5, Scotland n=5, USA n=1, Wales n=2) across rugby codes (rugby union and/or sevens n=25, rugby league n=6) and governing bodies (experts who consented to public recognition are included in the acknowledgement section). Experts were categorised into elite player (n=4), sports science (n=11), medical clinician (n=9) or sports administrator (n=7) domains. When experts crossed multiple domains, they were classed by their primary domain expertise. The expert group consisted of 12 men and 19 women. The average number of years of experience in participants’ respective domains (ie, player, sports science, medical clinician or sports administrator) were 6.4±4.4 years (range: 2–20 years). The response rates in this Delphi consensus method, from the original 52 international experts, were 60% (n=31; round 1), 56% (n=29; round 2) and 58% (n=30; round 3). Our retention rate was 97%, which is substantially greater than the expected rate of 75%.169
Consensus on future research priorities
During round 1, experts identified 183 individual meaning units. A meaning unit represents an idea, argument/reasoning chain or discussion topic in content analysis.170 171 Twenty-one meaning units were removed as they were irrelevant to applied sports science and sports medicine in women’s rugby (eg, meaning units pertaining to sociology). To form expert-based subthemes, meaning units were streamlined for clarity and concision. The abstraction process revealed 68 expert-based subthemes, which were categorised into 5 expert-based themes (ie, female health, injury, match characteristics, physical performance and psychology). After subtheme duplicates were removed, 41 unique expert-based subthemes emerged. The expert-based themes that reached consensus on future research priority during round 2 included injury (median research priority=5.0 (1.0)), female health (median research priority=4.0 (1.0)) and physical performance (median research priority=4.0 (1.0)). Furthermore, two expert-based injury subthemes and one expert-based physical performance subtheme reached consensus. An additional five expert-based female health subthemes and one expert-based psychology subtheme reached consensus. During round 3, although no expert-based themes reached consensus, subthemes in female health (n=2), injury (n=3) and physical performance (n=1) did. All expert-based themes and subthemes of research priority that reached consensus are listed in table 2. Likert scale ratings were combined (ie, low: 1 and 2; medium: 3; high: 4 and 5).44
Expert-based subthemes that reached consensus, median research priority (IQR) calculated from a 5-point Likert scale and percentage of expert agreement
Expert-based (sub)themes that did not reach consensus
Match characteristics (median research priority=3.0 (1.0)) and psychology (median research priority=4.0 (1.0)) were the two expert-based themes that did not reach consensus. Unique expert-based subthemes that did not reach consensus (n=43) are listed in online supplemental table 8. Although consensus was not reached, these themes and subthemes may be important to some but not all stakeholders in women’s rugby.
Supplemental material
Discussion
This systematic scoping review and Delphi consensus aimed to summarise the current evidence and provide consensus on future research priorities in women’s rugby. Part 1 of this study, the systematic scoping review, identified 123 studies that were categorised within six evidence-based applied sports science and sports medicine themes (ie, fatigue and recovery, injury, match characteristics, nutrition, physical performance, and psychology). Part 2 of this study, the Delphi consensus, included an international group of expert stakeholders in women’s rugby, including elite players, sport scientists, medical clinicians and sports administrators, to determine consensus on future research priorities. Consensus on future research priorities for injury, female health and physical performance expert-based themes was achieved. The findings of this systematic scoping review and Delphi consensus provide clear future research priorities in women’s rugby for several stakeholders, including practitioners, researchers, policy makers and governing bodies.
Experts identified the injury as a very high-priority research theme (median research priority=5.0). Five unique research subthemes were identified within this expert-based theme, with 77%–93% of experts stating these were a high priority. Concussion occurrence, risk factors, mechanisms and return-to-play management (median research priority=5.0, 93% high-priority expert agreement) and women’s response to concussion (median research priority=4.0, 90% high-priority expert agreement) were the two highest priority subthemes. This systematic scoping review supports the notion to investigate concussion further, as women’s rugby injury locations were commonly the head and lower limb, with collisions or tackles frequently reported as the cause (online supplemental table 2). Injury incidence was variable in women’s rugby and reported between injury types at 1–106 injuries per 1000 hours (online supplemental table 2). In professional men’s rugby union, match injury incidence has been reported to be 87 per 1000 hours.172 The large range in injury incidence found in this systematic scoping review may be due to various codes, cohorts, injury definitions and injury surveillance time course (eg, one season, 5 years) between the included studies (online supplemental table 2). Similar to women’s rugby, men’s rugby league173 and union172 found the head/face/neck, knee and lower limb to be frequent injury sites and the tackle as a common injury cause. For example, in professional men’s rugby union, tackle was responsible for 46% of ankle injuries, 45% of knee injuries and 66% of shoulder injuries.172 Furthermore, injury risk reduction strategies (eg, warm-ups, neuromuscular training and tackle technique) (median research priority=5.0, 86% high-priority expert agreement) were deemed a very high priority by experts. When considering the high research priority for injury risk reduction strategies and the tackle being responsible for a high percentage of injuries in women’s rugby (online supplemental table 2), the investigation of tackle technique and injury is justified within women’s rugby research.
Experts identified female health as a high-priority research theme (median research priority=4.0). In this expert-based theme, seven unique subthemes were identified, with 72%–90% of experts stating these were a high priority for research. The menstrual cycle, and its relationship to applied sports science and sports medicine, was found to be a common priority among experts. Menstrual cycle and injury, training load, performance, well-being and symptom management all achieved expert consensus (median research priority=4.0–5.0, 72%–90% high-priority expert agreement). Although in the evidence base there are recent meta-analyses available that investigate menstrual cycle39 and oral contraceptive174 effects on exercise performance in women, this systematic scoping review found that menstrual cycle research in rugby populations is sparse (n=1).160 Similar to the female health research priority that achieved expert consensus (table 2), a recent narrative review of health and performance in women’s football (soccer)175 highlighted menstrual cycle and performance, menstrual cycle and injury, menstrual cycle and responses to training, hormonal contraceptives, and energy availability as important considerations for women’s football. While female health has been highlighted as a high-priority expert-based theme, insufficient studies were identified in this systematic scoping review to warrant female health as an evidence-based theme. This is likely owing to the limited number of published research articles on women’s rugby at present. Despite this, relevant female health studies identified in this systematic scoping review include investigations of menstrual cycle on performance,160 breast injuries,96 urinary incontinence158 and iron deficiency.127 129 It remains clear, based on expert consensus and evidence base gaps, that further female health research is required in rugby to support both player health and performance.
Experts identified physical performance as a high-priority research theme (median research priority=4.0). In accordance with previously published scoping reviews on women’s football (soccer)38 and netball,36 the present systematic scoping review found that physical performance was a highly researched theme (n=32 of 123 studies). The two expert-identified physical performance research subthemes were strength and conditioning practices and efficacy in women’s rugby (median research priority=4.0, 77% high-priority expert agreement) and fatigue and recovery (median research priority=4.0, 76% high-priority expert agreement). This systematic scoping review highlighted that, although physical performance was the second most researched evidence-based theme, a research gap is still evident. Only two studies were identified that investigated strength and conditioning practices,162 163 and all the identified fatigue and recovery studies45–50 were performed in rugby sevens. In contrast, the fatigue and recovery research in men’s rugby, for example, comprises enough studies to compile reviews on male age-grade rugby union35 and senior men’s rugby league and union.176 Given both expert consensus and the current evidence base limitations, future physical performance research could aim to improve understanding of (responses to) strength and conditioning training, and fatigue and recovery responses to various physical stimuli women’s rugby players are exposed to (eg, collisions, high-speed running).
Although the expert-based theme of psychology did not reach consensus (ie, <70% expert agreement), its subtheme of mental health (eg, stress, body dysmorphic disorders, depression, eating disorders) was deemed a high research priority (median research priority=4.0) by 76% of experts. As per our systematic scoping review findings, the evidence base on psychology in women’s rugby is sparse (n=5). Studies investigating psychological aspects in women’s rugby were varied in their topics and included maladaptive schemas,167 mental toughness,165 avoidance behaviours,168 coach–athlete relationship166 and participant motivation.164 This evidence scarcity is also apparent in psychological research on male rugby in both senior and junior populations.35 177 Furthermore, although not achieving consensus, four expert-based subthemes in psychology attained a high priority from ≥57% of experts (online supplemental table 8) (ie, psychological aspects of dual-career players, psychological demands of rugby, optimising the relationship between (male) coaches and women’s rugby players, psychological barriers to rugby participation). When considering expert consensus and the current lack of psychological evidence on women’s rugby, future research could investigate mental health in women’s rugby.
This systematic scoping review revealed a further two evidence-based themes, nutrition and match characteristics, that subsequently did not achieve expert consensus as research priorities. An absence of literature on nutrition in women’s rugby is apparent (n=6). This finding is comparable with reviews on men’s rugby union,35 178 men’s rugby league,179 women’s football (soccer)38 and netball.36 Three expert-based subthemes on nutrition were identified (nutritional strategies to reduce concussion risk, interventions (training, nutritional) to enhance performance, and nutritional requirements and supplementation), all of which did not achieve consensus (median research priority=3.5, 4.0 and 3.0, respectively; high priority expert agreement=23%, 53% and 27%, respectively). These findings suggest that, overall, nutrition investigations are of moderate to high research priority but may be of high priority to some stakeholders. In the match characteristics evidence-based theme, a relatively high proportion of studies investigated physical match characteristics (n=21) compared with technical-tactical characteristics (n=5). This systematic scoping review found that no technical-tactical characteristics studies were performed below the international standard. Although they did not reach consensus, five expert-based subthemes on match characteristics were identified (online supplemental table 8). The highest priority match characteristics subtheme (relationship between match characteristics and injury) achieved a median priority of 4.0, and 63% of experts agreed it was a high priority. Match characteristics may not be deemed a high research priority by experts as, overall, this theme accounts for a high percentage (21% of 123 included studies) of all studies included in this systematic scoping review.
Overall, this systematic scoping review and Delphi consensus highlights key future research priorities in applied sports science and sports medicine in women’s rugby. Expert-based themes and subthemes that have achieved consensus represent high research priorities that have been agreed upon by a diverse range of international stakeholders (elite players, sports scientists, medical clinicians and sports administrators). Results from part 1 of this study highlight that some themes are under-researched (eg, female health, fatigue and recovery, nutrition, psychology). Due to the broad nature of scoping reviews and the aim of developing a consensus statement on future research priorities in mind, not all research gaps have been highlighted in this study. Additionally, combining rugby codes (ie, rugby sevens, rugby union and rugby league) may have impacted consensus as some expert-based themes (and subthemes) may be relevant to some but not all rugby codes. Furthermore, some expert-based themes (and subthemes) may be important to only specific expert groups (eg, players), which may explain why consensus was not reached (see online supplemental table 8). The (sub)themes that did not reach consensus may provide specific stakeholders with valuable information for further investigation. Finally, this systematic scoping review and Delphi consensus employed robust methodology by sampling several experts from various domains. Typically, athletes have not been included in the co-construction of sports science research.19 22 Including elite players in our expert panel not only develops upon previous research19 22 but also ensures findings are relevant to women’s rugby players.20 A wide range of international experts were included to ensure several opinions would be captured, thus enhancing the translational impact and benefit of the research.17 18 21 Although there was a wide array of international experts included, recruitment of experts may have been limited by selection bias. Due to the limited time allotment (ie, 1 week) for experts to review the findings of part 1 (online supplemental tables 1–7) to inform expert-based research priorities, some expert-based research subthemes may be already appropriately covered by existing literature. Future research on applied sports science in women’s rugby can use the data presented in this study to prioritise research topics and streamline projects to ensure the best use of scientific resources.
Conclusions
This systematic scoping review and Delphi consensus summarises the applied sports science and sports medicine in women’s rugby evidence base and provides consensus on future research priorities. Part 1 of this study, the systematic scoping review, identified 123 studies investigating applied sports science and sports medicine in women’s rugby (ie, rugby union, rugby sevens, rugby league). Most of the included studies (83%) were published in the last decade (table 1). Studies with rugby union or rugby sevens cohorts were the most common (n=83, 67%). Studies were categorised into six sports science and sports medicine evidence-based themes, namely injury, physical performance, match characteristics, fatigue and recovery, nutrition, and psychology. Summary tables of the systematic scoping review (online supplemental tables 1–7) provide valuable reference information for researchers and practitioners. In part 2 of this study, the Delphi consensus on future research priorities in women’s rugby, international experts (elite players n=4, sport scientists n=11, medical clinicians n=9, sports administrators n=7) identified and achieved consensus on three expert-based themes, namely injury, female health and physical performance. The findings of this two-part study facilitate efficient and coordinated use of scientific resources towards high-priority themes. The findings of this systematic scoping review and Delphi consensus can be used to further develop the applied sports science and sports medicine support provided to women’s rugby players. The results of this study have relevance to a wide range of stakeholders in women’s rugby, including practitioners, players, researchers and governing bodies.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Leeds Beckett University Research Ethics Committee (#80327). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to extend their gratitude to all members of the expert panel for their contributions. The expert panel members included the following: Allan Macdonald (Scottish Rugby), Andy Boyd (Scottish Rugby), Dr Anthea Clarke (La Trobe University), Dr Anthony Couderc (French Rugby Federation), Caoimhe Morris (Rugby Academy Ireland), Professor Carolyn Emery (University of Calgary), Dr Claire McLaughlin (Irish Rugby), Associate Professor Clare Minahan (Griffith University), Dr Éanna Falvey (World Rugby), Dr Izzy Moore (Cardiff Metropolitan University), Dr Gemma Phillips (Rugby Football League), Gemma Fay (Scottish Rugby), Dr Ian Sampson (Rugby Football League), Isla Shill (University of Calgary), Kathryn Dane (Irish Rugby), Dr Katy Hornby (England Rugby), Kris Robertson (Rugby Canada), Lauren Delany (Irish Rugby), Lesley McBride (University of Coventry), Lindsay Starling (University of Bath), Luke Woodhouse (England Rugby), Nicky Ponsford (England Rugby), Orlaith Curran (Irish Rugby), Rachel Faull-Brown (England Rugby), Dr Rachel Malcolm (Scottish Rugby), Robert Cain (USA Rugby), Dr Sharron Flahive (Australian Rugby), Stuart Barrow (Rugby Football League), Thomas Brindle (Rugby Football League) and Dr Thomas Longworth (Australian Rugby League Commission).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Omar_Heyward, @S_Emmonds, @GregoryRoe, @SeanScants, @drkeithstokes, @23benjones
Contributors OH, KS and BJ conceptualised the manuscript. OH, SE, GR and BJ identified the method and framework for the manuscript. OH and SS proposed the search strategy and screened the studies. OH prepared the manuscript. All authors contributed to subsequent drafts and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.