Article Text

Abstract
Background Lifeguards may face many life-threatening situations during their careers and may be at increased risk of post-traumatic stress disorder (PTSD). Minimal evidence concerning critical incident management systems in lifeguard organisations exists.
Objectives To develop, implement and evaluate an operational system for critical incident management in lifeguard organisations.
Methods This retrospective study included data on occupational injury reports from 2013 to 2022 in TrygFonden Surf Lifesaving Denmark. All active lifeguards were invited to evaluate the system and the individual steps using an online questionnaire with three questions rated on a 5-point Likert scale. Primary outcome was a change in the frequency of psychological injury reports after system implementation in 2020. The secondary outcome was the lifeguards’ satisfaction with the system.
Results After implementation, the average annual number of psychological injury reports increased 6.5-fold from 2 (2013–2019) to 13 (2020–2022), without changes to the number of critical incidents attended by the lifeguards. Sixty-six (33.8%) active lifeguards answered the questionnaire and agreed that follow-up after critical incidents was very important (mean score 4.7/5). Satisfaction with steps 1–2 and 3 of critical incident management among involved lifeguards was high (mean score 4.4/5 and 4.6/5, respectively). The system included an operational workflow diagram and incident report template presented in this study.
Conclusions The operational system for critical incident management may improve early recognition of symptoms for the prevention of PTSD. It may be used as a screening and decision tool for referral to a mental health professional.
- psychology
- retrospective
- performance
- sports medicine
- water sports
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lifeguards may be at increased risk of post-traumatic stress disorder (PTSD). Still, most lifeguard organisations and training programmes pay minimal attention to PTSD.
WHAT THIS STUDY ADDS
This study provides a baseline for change. It presents a system that can be implemented worldwide with little adaptations, with the benefit of improving the lifeguards and their organisation’s awareness and adherence to monitoring their psychological health.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study may improve early recognition of symptoms for the prevention of PTSD, which may be the first step in future research.
Introduction
Lifeguards may face many psychologically distressing, life-threatening situations outside the range of usual human experiences during their careers and may be at increased risk of post-traumatic stress disorder (PTSD).1 2 The syndrome results from an experience of intense fear or horror after being exposed to a traumatic (especially life-threatening) event.3 4 The symptoms of PTSD occur after the traumatic event and include recurrent, distressing memories, dreams or flashbacks of the traumatic event, persistent avoidance behaviour, adverse changes in cognitions and mood, and changes in arousal and reactivity in terms of irritable behaviour, hypervigilance or sleep disturbance. Symptoms last more than 1 month and cause significant impairment in critical areas of functioning.5 High-risk situations encountered by the lifeguard vary from fatal and non-fatal drowning accidents to non-water-related life-threatening incidents involving heart attack, severe trauma and multicasualty incidents.6 7 The psychological stress in these situations may be exaggerated due to the emotional reactions from other bystanders and relatives or because of the experienced danger to the lifeguard during a rescue (eg, high surf or being pulled under by the victim).8 Normal lifeguard behaviour also contributes to stress build-up, as lifeguards repeatedly scan the same area with hundreds or thousands of people for long periods while remaining highly alert and making split-second decisions.1
PTSD is triggered by an incident and has an apparent onset. The onset of symptoms typically occurs after a latency period ranging from a few weeks to months,9 but early symptoms may develop within days after the incident.10 Even though PTSD is not inevitable and post-traumatic growth may occur, the apparent onset and early symptoms provide opportunities for early recognition and prevention. If the lifeguard organisation does not have an operational system for critical incident management, recognition of PTSD may be delayed. Although only a minority of rescue workers will develop PTSD or major depression in the years following a critical incident,11 delayed treatment may result in lifelong psychological consequences for those in need, increased alcohol and drug use, and affected job performance in the future.1 12 Anxiety and depression are commonly associated with PTSD signs and symptoms, and suicidal ideation is known to occur.13 Evidence of PTSD among lifeguards is minimal,1 and extrapolation from other categories of rescue workers (eg, police officers, ambulance officers and firefighters) is necessary. Extrapolation needs to be cautious as most rescue workers are older and have more hours of training compared with the average lifeguard.1 In Denmark, pool lifeguards may be employed at age 16,14 similar to the UK and New Zealand. The minimum age requirement in Germany and Brazil is 15 years and that in Australia is 17 years.1 In Denmark, the pool lifeguard course takes less than 10 hours of training. Most lifeguards work seasonally, and most lifeguard training programmes pay minimal to no attention to PTSD.1
This study aimed to develop, implement and evaluate an operational system for critical incident management in TrygFonden Surf Lifesaving Denmark.
Methods
Study design
We conducted a national retrospective observational study describing the development, implementation and evaluation of a three-step system for critical incident management in TrygFonden Surf Lifesaving Denmark.
Outcomes
The primary outcome was a change in the frequency of psychological injury reports following system implementation and activation in season 2020. Secondary outcomes were satisfaction with the system and the individual steps.
Setting
The position of a professional lifeguard in TrygFonden Surf Lifesaving Denmark is to maintain supervision and safety of the beach, provide advice on safety to visitors and perform rescues, first aid and resuscitation as required—alone if necessary.15
Every lifeguard station is manned between 10:00 and 18:00 7 days a week by two lifeguards, and every Monday, the lifeguards move to a different beach with a new colleague. Once every week, the lifeguards are subject to an unannounced in situ simulation-based exercise within working hours and subsequent debriefing by their local supervisors. The purpose of the simulation is to evaluate practical skills, decision making and teamwork and to make the participants reflect on how to improve future performance in real-life situations. This type of in situ training combines skills training and stress exposure, which has been shown to improve the functioning of the lifeguards by reducing stress responses1 2 and optimising real-situation patient care.16 Each of the five regions in Denmark has a supervisory team (consisting of two experienced lifeguards with additional instructor training) responsible for approximately 10 lifeguard stations. Their job is to coordinate lifeguarding shifts, handle the day-to-day function of a lifeguard station and respond to stations following a critical incident.
Participants
The minimum age requirement for Danish surf lifeguards is 18 years.17 The lifeguard training is divided into three levels: open water lifeguard (first year), surf lifeguard (second year) and senior lifeguard (third year), constituting around 50 hours of training per year.15 After completing the training programme each year, the lifeguards are assigned between 3 weeks and 11 weeks of full-time work during the summer holiday.
Three-step system for critical incident management
In 2019, an interdisciplinary working group consisting of a physician, a psychologist, the operations manager, and the education and training manager at TrygFonden Surf Lifesaving Denmark was established. A 2-year plan was made to ensure sufficient implementation and evaluation of the critical incident management system. First year (2019), a three-step system for critical incident management was developed with inspiration from Grosse,8 19 based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,3 and the International Classification of Diseases, 11th Revision,4 criteria for PTSD. Second year (2020), the organisation implemented the three-step system with an extensive focus on critical incidents, debriefing, PTSD potentials and symptomatology in the lifeguard training programmes at all levels. The three-step system included an operational workflow diagram (figure 1), an incident report template (figure 2), and Danish teaching materials targeting lifeguards and supervisors (available from the corresponding author on request).

Workflow diagram showing the three-step system for critical incident management in TrygFonden Surf Lifesaving Denmark consisting of (1) accident reporting within 6 hours after an incident, (2) staff informational debriefing within 24 hours after an incident, (3a) critical incident stress debriefing, and (3b) critical incident medical debriefing. This system was active from 2020.

Incident report template in TrygFonden Surf Lifesaving Denmark. AED, Automated External Defibrillator; CPR, cardiopulmonary resuscitation; EMS, Emergency Medical Service; LG, Lifeguard; ROSC, Return Of Spontaneous Circulation.
Step 1: defusing and incident reporting
The first step was informal defusing, characterised as a reflective discussion around the critical incident between the involved lifeguards, allowing the lifeguards to talk about crisis memories in a safe and supportive environment. The incident report (figure 2) provides a structure for the defusing and should be factual, unemotional, verifiable and specific. The lifeguards should contact their local supervisor within 6 hours after a critical incident. It is advised that defusing and incident reporting be commenced immediately after the critical incident to prevent a series of pathological reactions that may cause PTSD.20 21 Furthermore, writing the incident report is part of the legal process in many aquatic facilities.
Step 2: staff informational debriefing
The second step was a non-judgemental staff informational debriefing with the local supervisor as moderator characterised as an objective, factual reporting, as recommended by the American Red Cross,22 to structure and analyse the sequence of events and prevent similar incidents in the future.23 The debriefing occurred in a secure area away from the lifeguard station, as recommended, within 24 hours after the incident.1 During the staff informational debriefing, the supervisor gathered all information necessary to follow the workflow diagram (figure 1). The primary aim was to detect early symptoms for referral to a mental health professional. The secondary aim was to educate the lifeguards on common PTSD symptoms, as some may not experience symptoms until after a latency period. Initial emotional reactions should not be perceived as signs of mental disease, as they often decrease within days to weeks.24
Step 3: critical incident stress and medical debriefing
The third step was a non-judgemental critical incident debriefing with a health professional. It was divided into two: 3 a) critical incident stress debriefing with a psychologist, and 3b) critical incident medical debriefing with the Chief Medical Officer or other first aid coordinator. If the lifeguards were referred for a critical incident stress debriefing, the mental health professional would contact the lifeguards to arrange a group meeting for a professional debriefing, usually within a 72 hours after the critical incident. The stress management debriefing aimed to precipitate the healing process,25 minimise emotional impact,26 and prevent long-term damage, which is beyond this paper’s scope. The debriefing initially included all the lifeguards involved, followed by more group or individual meetings as appropriate. Inviting the lifeguards for a follow-up debriefing several weeks after the incident was recommended.25
The critical incident medical debriefing should be scheduled after the stress debriefing. The primary aim was to provide answers to medical questions and create a better understanding of the incident and its outcomes. The secondary aim was to collect input from the lifeguards on how to improve lifeguard training in the future.
Data collection
TrygFonden Surf Life Saving Denmark agreed to share anonymised data on Danish lifeguards and their occupational injury reports from 2013 to 2022. One month after the 2020 season (year of implementation), TrygFonden Surf Lifesaving Denmark requested all employed lifeguards, regardless of their involvement in critical incidents, to evaluate the critical incident management system. The lifeguards received an initial email invitation and reminder mail 2 weeks later. Participation was voluntary and unpaid, and data were anonymised prior to analyses. The questionnaire contained three questions that were rated on a 5-point Likert scale:
‘How important is the follow-up after critical incidents?’
‘How satisfied are you with the defusing and the staff informational debriefing following critical incidents (if you experienced any)?’
‘How satisfied are you with the critical incident stress and medical debriefing following critical incidents (if you experienced any)?’
Participants could also comment on the three-step system for critical incident management.
Statistical analysis
The statistical analysis is consistent with the CHecklist for statistical Assessment of Medical Papers (CHAMP) statement.27 Categorical variables are presented as frequencies (counts and percentages). Occupational and psychological injury reports are presented as medians with IQRs. P values were calculated using Kruskal-Wallis test. P values of <0.05 were considered statistically significant. Statistical analyses were performed using RStudio V.1.2.5001.28 Comments in the free text were analysed qualitatively and included as quotes were appropriate.
Equity, diversity and inclusion statement
The study population included all active lifeguards in TrygFonden Surf Lifesaving Denmark. The author team was multidisciplinary and multigender and included junior researchers. Data collection and analysis were made on pre-existing data.
Patient and public involvement
Given the study’s retrospective nature, participants or the public were not involved in the design.
Results
TrygFonden Surf Life Saving Denmark counts approximately 205 active lifeguards each year (74% male), 50 (25%) first-year lifeguards, 36 (17%) second-year lifeguards, 94 (46%) senior lifeguards and 25 (12%) instructors/supervisors (see table 1).
Baseline characteristics from TrygFonden Surf Life Saving Denmark
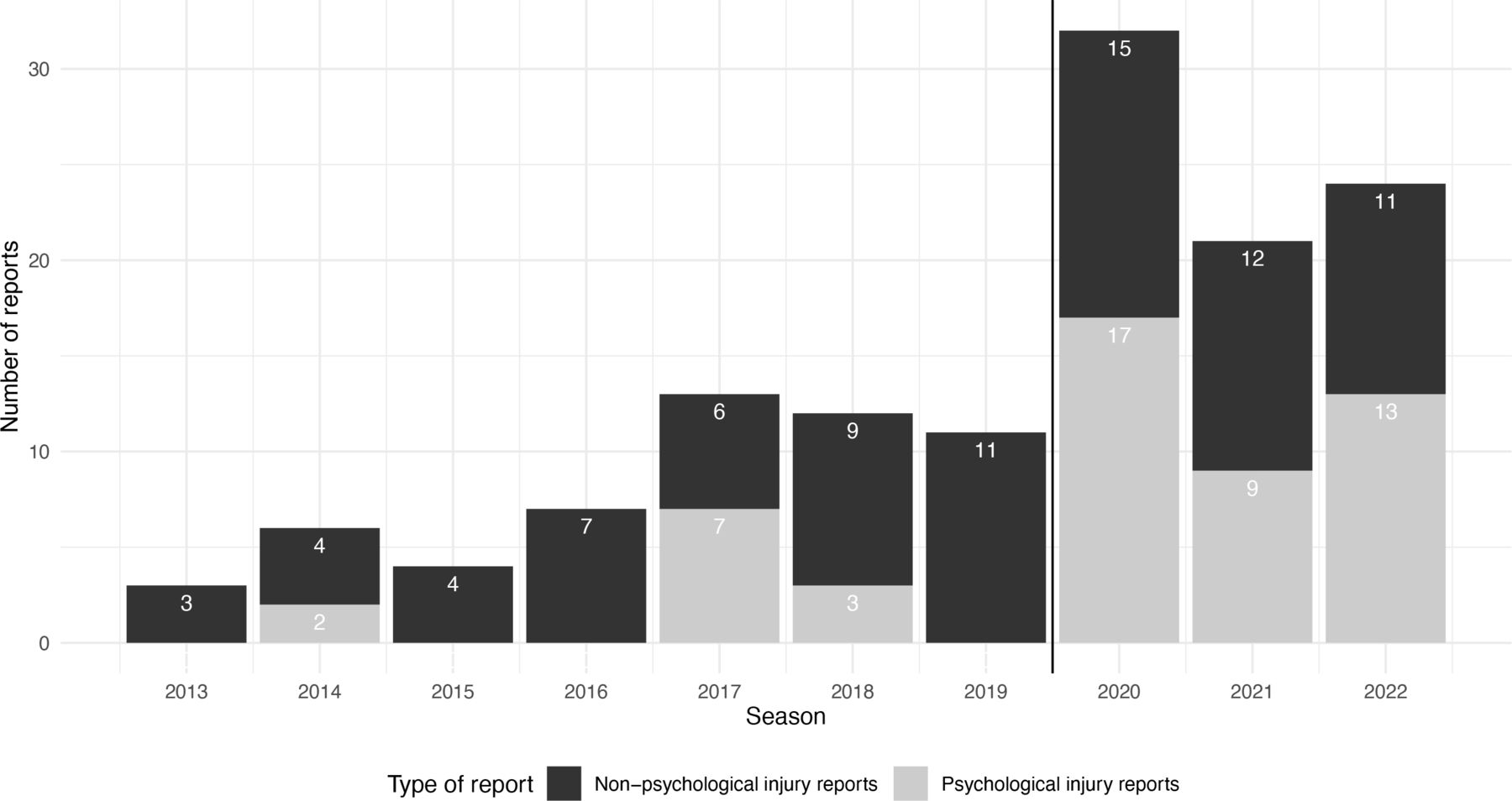
Median (IQR) incidence of all types of occupational injury reports increased from 7,5 12 between 2013 and 2019 (before implementation) to 24,23 29 between 2020 and 2022 (after implementation) (p=0.017). Non-psychological occupational injury reports increased from 64 8 (before implementation) to 1212–14 (after implementation) (p=0.022), and psychological injury reports increased from 0 (0–3) (before implementation) to 1311 15 (after implementation) (p=0.014) (table 2 and figure 3). There was no increase in the number of cases attended by the lifeguards in the period from 2018 to 2021.
Change in injury reports from before and after implementation of a critical incident management system in TrygFonden Surf Life Saving Denmark

{kind=link}
{kind=link}
{kind=link}
Frequencies (counts and percentages) of occupational and psychological injury reports from 2013 to 2022. Following system implementation and activation in 2020, the annual incidence of occupational injury reports increased from 8 (2013–2019) to 26 (2020–2022). Simultaneously, the annual incidence of psychological injury reports increased from 2 (2013–2019) to 13 (2020–2022).
One month after the 2020 season, all 195 active lifeguards received the questionnaire, and 66 answered the questionnaire (response rate 33.8%). There were no missing data from the questionnaires. Reasons for non-participation were not routinely collected. There was a general agreement among lifeguards that follow-up after critical incidents was essential (4.7/5).
Thirty-seven (56.1%) of the participating lifeguards had been involved in a critical incident and participated in defusing and supervisor debriefing. Satisfaction with defusing and supervisor debriefing was high (4.4/5).
It is reassuring to know that there is a follow-up after critical incidents, even if it is not a cardiac arrest. During my employment, this [operational system] is one of the best initiatives in TrygFonden Surf Lifesaving Denmark. (LG1)
The local supervisors should have a template for staff informational debriefing to standardise the structure of the conversation. (LG4)
It was suggested that all lifeguards within the organisation be informed about critical incidents to increase transparency, allow colleagues to applaud the involved lifeguards and as a learning opportunity for others.
Of the 37 participating lifeguards involved in a critical incident, 10 (27.0%) were referred to a professional debriefing. Satisfaction with the professional debriefing was high (4.6/5).
The critical incident mental debriefing is a fantastic offer to those in need. The mental health professionals must know our organisation to be of better assistance. (LG5).
The critical incident medical debriefing is extremely useful. It is good that the debriefing is scheduled some weeks after the incident to allow the lifeguards some time to reflect and recover. (LG6)
It was suggested that the lifeguard station should be closed during step 1: defusing and incident reporting, and step 2: staff informational debriefing. It may be untimely to close the station (eg, on busy days or in dangerous conditions). Under these circumstances, lifeguards from adjacent lifeguard stations may be summoned to assist, or the local supervisor may undertake surveillance to give the lifeguards time off directly after the critical incident. This may prevent pathological reactions and reduce sick leave in the long run.30 It was recommended that bystanders and other healthcare professionals be invited to participate in the staff informational debriefing, if possible.
Discussion
Summary of findings
Following system implementation in 2020, the annual incidence of all occupational injury reports, including psychological and non-psychological reports, increased significantly. Lifeguards considered follow-up after critical incidents highly important. Lifeguards were highly satisfied with the staff informational debriefing moderated by the local supervisor and the critical incident stress and medical debriefing moderated by health professionals. Follow-up after critical incidents is essential, as there are several characteristics related to the work as a lifeguard, the seasonal employment, the administration and the culture within lifeguard organisations that counteract mental health.1
Normal lifeguard behaviour contributes to stress build-up in many ways (eg, repeatedly scanning the same area for long periods while remaining highly alert, making split-second decisions and endangering their own lives when attempting a rescue).1
Seasonal work is characterised by variable hours, and weekly changes in workplace and lifeguard staffing situations make it challenging to gather the seasonal lifeguards for debriefings within working hours. The onset of post-traumatic stress symptoms typically occurs after a latency period ranging from a few weeks to months.9 It may only occur after the season when the lifeguard and the local supervisors are not legally employed. Screening criteria are essential to consider during the lifeguard selection process (eg, age criteria and personality testing), as young individuals1 (<18 years) with high scores on neuroticism31 may be at increased risk of highly perceived stress following a critical incident.
Employers of seasonal staff may not provide the necessary resources to establish a critical incident management system. They may not prioritise education regarding risk factors, symptoms, trajectories and prevention of PTSD for lifeguards and supervisors. However, education is a crucial step towards changing the culture in lifeguard organisations. Here, lifeguards may be expected to handle stress; seeing a mental health professional may be a stigma; and colleagues and supervisors may not identify the critical incident as critical.32
Implementation barriers
In TrygFonden Surf Lifesaving Denmark, only the first step was made mandatory for legal reasons, and subsequent steps were offered to lifeguards. The system received great support from the lifeguards, and we experienced no major challenges to system implementation at lifeguard level. Some of the local supervisors were initially concerned about moderating the staff information debriefing for their colleagues and not having the required skills or professional attitude. However, after sufficient training and implementation of standardised criteria for referral, the supervisors accepted their new responsibilities. In our opinion, using the local supervisor’s knowledge about the lifeguards and the lifeguard organisation in their role as a moderator of the staff informational debriefing improved the quality and minimised the cost at this step. A template for staff informational debriefing may aid the supervisors at the beginning of the implementation phase to standardise the structure of the conversation.
Clinical implications
Every lifeguard organisation has employee mental health risk factors. Therefore, it is fundamental for all lifeguard organisations to implement a system for critical incident management. The findings of this study may be implemented in all lifeguard organisations worldwide. They may also be implemented as part of a citizen first responder system to standardise critical incident management.
Limitations
We could not perform an in-depth analysis as baseline data, incident reports and occupational injury reports were not routinely collected. Furthermore, the questionnaire data were anonymous, and we could not include the lifeguards’ short-term or long-term outcomes following critical incidents.
Future studies should collect these data to evaluate the effect and refine the three-step system for critical incident management. This study introduced non-response bias as only 66 (33.8%) lifeguards participated in the questionnaire, including 10/17 (58.8%) who were referred for professional stress debriefing with a mental health professional. Both positive and negative experiences would be incentives to participate in the evaluation to improve the workflow in the future, and 56.1% of participants had experience with the system.
Conclusion
The operational system for critical incident management may improve early recognition of symptoms for the prevention of PTSD. Other lifeguard organisations worldwide may use this system, workflow diagram and incident report template as a screening and decision tool for referral to a mental health professional.
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants, but according to Danish law, retrospective studies do not need ethical approval and thus exempted this study. Informed consent was waived, given the retrospective nature of the study. Participation in the questionnaire was voluntary and unpaid. This study is reported in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies.29
Acknowledgments
The authors acknowledge the help of the management staff in TrygFonden Surf Lifesaving Denmark for allocating the necessary resources to develop the three-step system for critical incident management, the supervisors for undertaking the responsibility as moderators of the staff informational debriefing, and the lifeguards for their time and honesty in completing the survey questionnaire.
Footnotes
Contributors NB and KFS developed and implemented the flowchart in TrygFonden Surf Life Saving Denmark. NB, KFS, DØ and HCC participated in study conception and design. NB drafted the manuscript. KFS, DØ and HCC revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript and agreed on accountability. NB is responsible for the overall content as guarantor.
Funding This study was supported by the Danish foundation TrygFonden.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.