Article Text

Abstract
Objectives Little is known about the impact of elite sport participation on long-term athlete health. We aimed to: (1) describe musculoskeletal, mental health, reproductive/endocrine and cardiovascular characteristics in retired elite female athletes and compare to the general population and (2) explore athletes’ perceptions of their elite sport participation and its impact on health.
Methods A 136-item online questionnaire was disseminated to Canadian elite female rowing and rugby athletes >18 years old, >2 years retired from elite competition. Matched general population data were obtained from Statistics Canada when available.
Results Seventy-four (24% response rate) athletes (average age 45 (±9) years; retired 15 (±9) years) completed the questionnaire (30 rowing, 44 rugby athletes). During their career, 63 athletes (85%) experienced a hip/groin, knee, foot/ankle injury, or low back pain, with 42 (67%) reporting ongoing symptoms. Athletes 35–54 years reported worse knee symptoms and quality of life compared with the general population (symptom: p=0.197; d=1.15 [0.66, 1.63]; quality of life: p=0.312 d=1.03 [0.54, 1.51]) while other hip, knee and foot/ankle outcome scores were similar. Retired athletes had lower odds of anxiety (OR=0.155 [95% CI0.062 to 0.384]), greater lifetime/ever odds of amenorrhea (OR=6.10 [95%CI 2.67 to 13.96]) and gave birth when older (p<0.05). Fifty-nine (79%) recalled witnessing or experiencing at least one form of harassment/abuse during their career. Sixty athletes (81%) rated their current health as above average or excellent and 61 (82%) would compete at the same level again if given the choice.
Conclusion These novel insights can inform future preventative efforts to promote positive elite sport-related outcomes for current, former and future female athletes.
- female
- athlete
- elite performance
- rowing
- rugby
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Roughly half of retired female football players will develop knee osteoarthritis by age 50. Risk profiles of other female athletes are not known.
Retired male athletes with lower physical activity levels report increased mental health concerns (eg, anger, anxiety, depression). Data on female athletes are unknown.
Female athletes with Relative Energy Deficiency in Sport can suffer disruptions in menstrual function, with unknown impacts on long-term fertility.
Retired male athletes have similar cardiovascular risk profiles as the general population but higher rates of atrial fibrillation. The impact of intense training on the female athlete heart is unknown.
WHAT THIS STUDY ADDS
Most female athletes sustained at least one injury while competing, that affected performance or kept them out of training/competition for ≥1 week. Two thirds reported ongoing symptoms post-retirement. Over half of rugby players were diagnosed with at least one concussion during their career.
Retired female athletes had lower odds of having anxiety or depression than the general population. Half reported a history of either experiencing or witnessing verbal or physical abuse during their career.
Retired female athletes reported healthy cardiovascular risk profiles. Two rowers reported a history of atrial fibrillation.
Retired athletes had greater lifetime/ever odds of amenorrhea and gave birth at an older age when compared with the general population. They also reported lower rates of gestational hypertension, postpartum depression and urinary incontinence, and higher rates of twin pregnancy.
Retired female athletes reported above average to excellent health and if given the choice, would compete again.
The period of transition to retirement may result in poorer self-rated health in female athletes and presents an opportunity for targeted health counselling.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Research to date examining the health of retired female athletes is limited. This study advances knowledge across the domains of musculoskeletal, mental, reproductive and cardiovascular health for female athletes. As sport and exercise medicine researchers and clinicians, we must do better to improve injury prevention research and clinical initiatives for female athletes. Safe sport policy development and implementation are required to create safe sport environments for women’s sport. Screening, counselling and end-of-career health examinations can support female athletes during and after their careers, where the effects of intense training may impact them most.
Introduction
Major strides are being made in injury prevention and health promotion programmes1 for elite athletes to promote longer and safer careers in sport. However, little is known about the long-term health characteristics following retirement from sport—both positive and negative—for female athletes,2 and few supports exist. When data are missing, strategies to prevent injury and to protect the health of current and retired female athletes may fail.
The impact of elite sport participation on post-retirement health was deemed a critical research gap by the International Olympic Committee (IOC) and World Olympians Association.3 Specific knowledge gaps for retired female athletes include musculoskeletal (MSK) health characteristics (particularly post-traumatic osteoarthritis),4 concussion,5 mental health (including impacts of sports-related abuse and harassment),6 long-term sequelae of Relative Energy Deficiency in Sport (RED-S), reproductive health (including fertility/pregnancy)7 and cardiovascular health.4
Addressing these gaps is important for a number of reasons. Half of retired female football players developed knee osteoarthritis by age 50.8 Risk profiles of other female athletes are not known. While retired elite male football players had higher prevalence of mental health disorders, especially anxiety and depression (39%) than current players (26%),9 the prevalence of depression and anxiety in female players is largely unknown.6 Female athletes are more susceptible to concussion and report more concussion symptoms than male athletes.10–12 Female athletes with RED-S can have disrupted menstrual function, with unknown impacts on long-term fertility or pregnancy outcomes.13–15 Retired male athletes have similar cardiovascular risk profiles as the general population but higher rates of atrial fibrillation (AF), arrhythmias and other cardiac findings.16 Knowledge of the retired female athlete heart is scarce. Finally, long-term outcomes of experiences of athletes during their elite career—for example, associations between prior abuse and harassment and current mental health17–19—are unknown.
Therefore, the purpose of this study was to (a) describe the status of MSK, mental, reproductive/endocrine and cardiovascular health of retired elite rowing and rugby (union) athletes and compare these characteristics to the general population and (b) explore athletes’ perceptions of their elite sport participation, and its impact on their long-term health.
Methods
Methodological information is reported in accordance with the Checklist for Reporting Results of Internet E-Surveys20 (see online supplemental appendix A). Utilising a retrospective cross-sectional study design, self-report data were collected through an online questionnaire in English (Qualtrics software). Data were collected between 29 March to 22 June 2021. General population data were obtained from Statistics Canada when identical outcome measures were available, and from women with matched age ranges. When appropriate Statistics Canada surveys could not be identified, general population studies with compatible characteristics were identified through literature review. Ethical approval was obtained from Western University Research Ethics Board (number 118403).
Supplemental material
Study population and recruitment
Participants were retired elite (national team) Canadian female athletes that had participated in at least five international matches/races and/or selected to three international competitions between 1976 (for rowing) or 1981 (for rugby) and 2019. The start dates reflect the first years that Canadian teams participated in their respective international competitions. Respondents had to be at least 18 years old, at least 2 years retired from elite competition, and able to communicate in English. We chose two national sporting organisations with different physiological and performance profiles to gain a broader context—a non-contact aerobic endurance racing sport (rowing) and contact anaerobic/muscular endurance match sport (rugby).
Participants were recruited via convenience and snowball sampling. Recruitment emails were sent to Rowing Canada and Rugby Canada and their provincial organisations. These were distributed through their alumni email list, monthly newsletter and social media accounts. Prior to starting the questionnaire, potential participants were asked a series of questions to determine eligibility. No personal identifiers were collected, and data were stored on a secure network drive. Informed consent was implied through participation in the questionnaire, and all responses were anonymised.
Patient and public involvement
The survey was pre-tested by an athlete focus group comprised of Canadian female elite athletes (n=5). We tested survey flow, content and ‘burden’ (of time) and as a result, we improved navigation of the survey link so that participants could move freely through the survey and change answers if needed prior to submission, and we included the letter of information within the survey itself rather than as a separate document.
Measurement instruments and definition of constructs
A group comprised of researchers, sports medicine experts and retired athletes with content expertise (JT, KC, MM, MD, VG, PD) developed, pre-tested and assessed the survey for length and flow to minimise response burden. Four sports medicine committee members from Rowing Canada (n=2) and Rugby Canada (n=2) served as content experts. A focus group of five retired elite Canadian female athletes pre-tested the content and clarity of the survey.
The survey included 136 items taking approximately 15–30 min to complete and included the following questionnaires that have demonstrated validity evidence in our study population such as: Hip Disability and Osteoarthritis Outcome Score (HOOS),21 Knee Disability and Osteoarthritis Score (KOOS),22 Foot and Ankle Outcome Score23 and Oswestry Disability Index,24 Generalised Anxiety Disorder–7 (GAD-7)25 and Patient Health Questionnaire–9 (PHQ-9),26 and a modified version of the Low Energy Availability in Females Questionnaire27 to capture career-related data. To determine physical activity levels, we provided participants with definitions and examples regarding light, moderate and vigorous physical activity as per WHO guidelines28 and asked participants how many minutes per week they engaged in these activities. Because adaptive questioning was employed via skip logic, the total number of questions applicable to each respondent varied. Blank text boxes with no word limits were provided for all open-ended questions. Respondents could navigate back through the survey to change and review their answers as needed.
Details regarding the collection of MSK, mental, reproductive, cardiovascular and overall health and coding variables are reported in online supplemental table S1.
Statistical analysis
Descriptive statistics were generated to describe the sample. Continuous data were summarised with means and SD, and categorical data were summarised using percentage and counts separately for rowers, rugby players and all athletes.
Chi-squared tests determined the statistical significance of the unadjusted associations between dichotomous variables. Effect sizes for differences between two group means were expressed using Cohen’s d and Cohen’s h for continuous and dichotomous variables, respectively, such that values greater than 0.8 were determined to be clinically meaningful. Respondents without complete responses for both variables were excluded from the analysis. If expected cell counts were fewer than five, the two-sided Fisher’s Exact test was used. Unadjusted OR with 95% CI are presented.
Statistical tests were performed based on the type of constructs and data distribution to compare our sample to the general population: logistic regression (proportion of individuals meeting physical activity guidelines, clinical cutoffs of depression, anxiety); one sample t-test (age of mothers at childbirth); Mantel Haenszel chi-square test (oligomenorrhea, amenorrhea); and Wilcoxon signed rank test (knee pain, hip pain). When possible, age-stratified comparisons were conducted between the sample and the general population. Data were not matched on other characteristics. Statistical significance was determined at an alpha level of 0.05. All analyses were conducted using SAS software V.9.4 (Cary, North Carolina, SAS Institute).29
Open-ended data analysis
Two authors (EP, KR) used conventional content analysis to code participants’ responses to the open-ended question: ‘What advice would you give to a “rookie” athlete to consider with respect to optimising their health during their competitive career?’. The researchers independently reviewed and tagged data with preliminary codes, then subsequently reviewed 10% of the responses together to ensure coding alignment.30 Frequencies for each code were calculated and salient quotes representing each code were presented in tabular form.
We had 2/136 questions with a rate of missingness of over 5% or three responses. As there was no potential for large bias (large differences on important variables), we still included the overall responses from these participants, and these two data points were excluded from further data analysis.
Results
Sample characteristics
Based on sport records and alumni databases, there were 310 elite female rowers and rugby players eligible for this study (120 rugby+190 rowing athletes). From a total of 80 initial respondents, 6 did not meet eligibility criteria on the first two questions and their responses were removed from further analysis. Seventy-four respondents (24% response rate) were included in the study, 30 rowing and 44 rugby athletes. The average age was 45 (±9) years, and the average age at retirement was 29 (±4) years. The average duration of retirement was 15 years (range 2–40). Athletes participated on their national team for an average of 6 years and in 18 international events. See table 1 for complete demographic information.
Demographic information of survey respondents (n=74)
Injury history and MSK health
MSK health during athletes’ careers
Sixty-three of the 74 respondents (85%) reported a combined total of 115 MSK injuries that either altered their ability to perform or kept them out of training/competition for greater than 1 week during their career. Thirty-six (31%) were reported in the lower back (21 rowing, 15 rugby), 34 (30%) in the knee (6 rowing, 28 rugby), 27 (23%) in the foot or ankle (all rugby) and 18 (16%) at the hip/groin (4 rowing, 14 rugby) (figure 1). Eleven athletes (15%) reported no injuries during their careers.
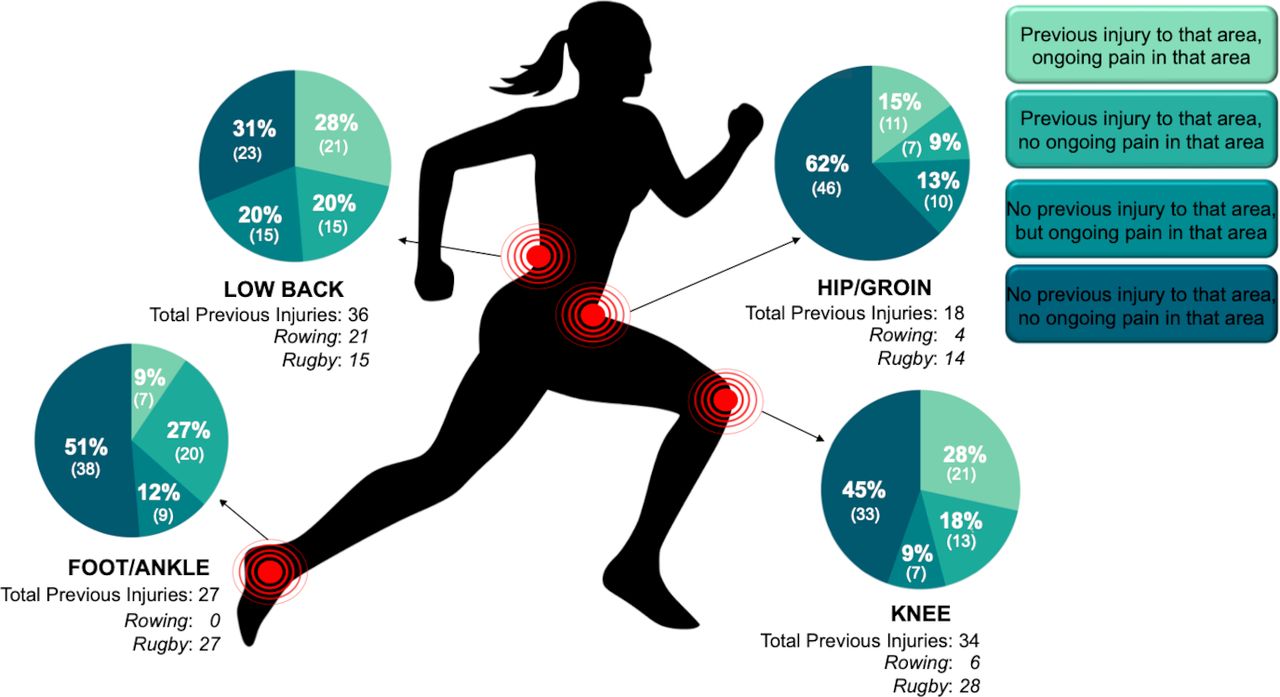
Number of reported injuries during competition and ongoing pain in the hip/groin, knee, foot/ankle and low back.
Current MSK pain
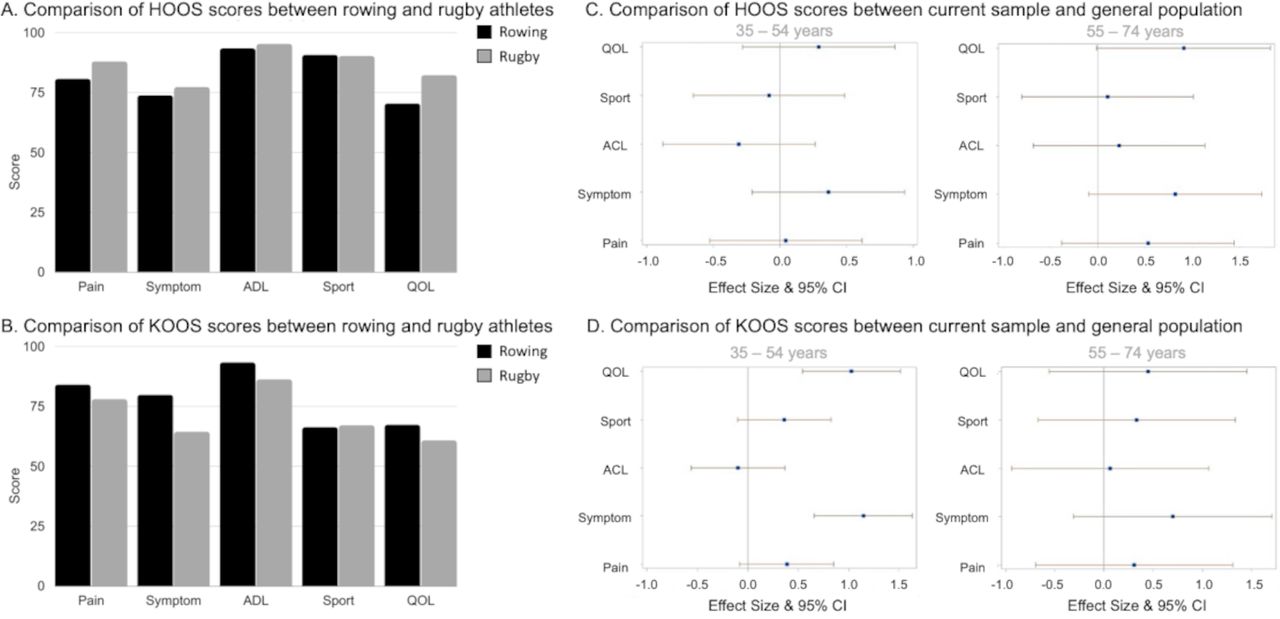
Of the 63 respondents that reported they sustained an injury during their career, 42 (67%) reported ongoing pain in the same region within the last year. Twenty-one (4 rowing, 17 rugby) reported knee pain, 21 (9 rowing, 12 rugby) reported low back pain (76% reported minimal and 24% moderate disability), 11 (4 rowing, 7 rugby) reported hip/groin pain, and 7 (all rugby) reported foot/ankle pain. Outcome scores are reported in figure 2.
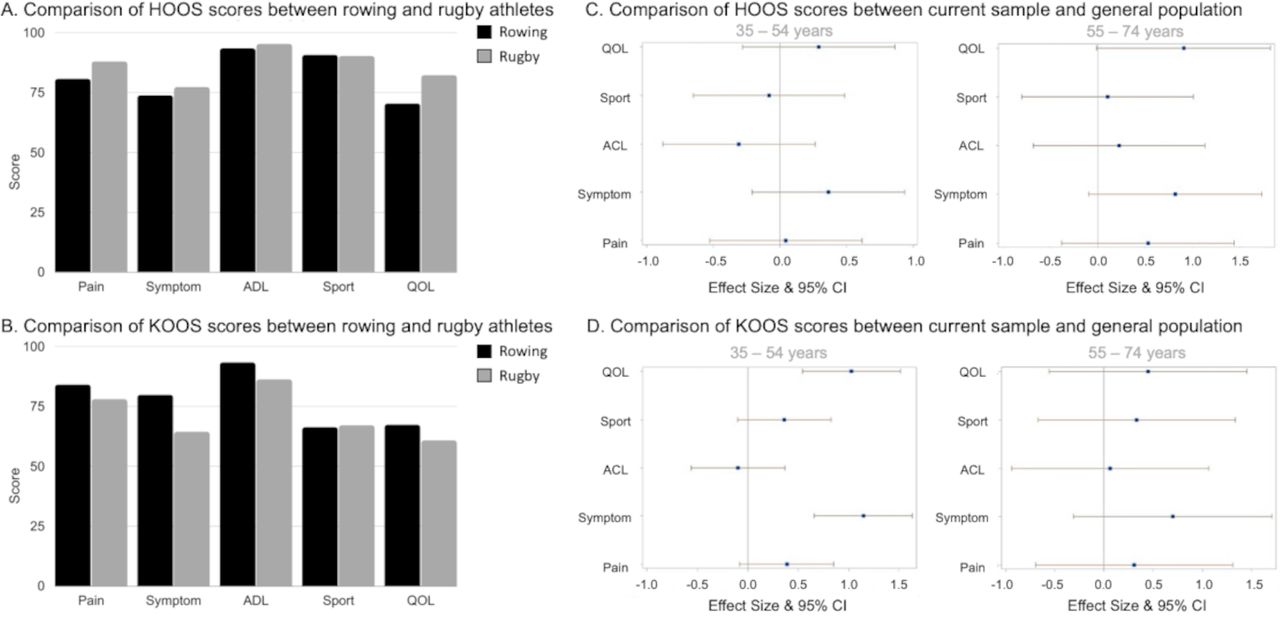
Average musculoskeletal outcome scores for hip, knee, foot and ankle and low back pain among respondents reporting injuries during their career and ongoing pain within the last year (A). Reported HOOS (B) and KOOS (C) between participants in current study sample who reported ongoing hip or knee pain compared to samples of the general population for pain, symptom, ADL, sport and QOL in 35–54-year olds and 55–74-year olds. ADLs, function in daily living; FAOS, Foot and Ankle Outcome Score; HOOS, Hip Disability and Osteoarthritis Outcome Score; KOOS, Knee Disability and Osteoarthritis Score; LBDI, Oswestry Low Back Disability Index; QOL, quality of life; Sport ADLs, function in sport and recreation.
Compared with an age-matched general Swedish population, there were no differences in HOOS scores for athletes (pain: p=0.967; d=0.05 [−0.53, 0.61], symptom: p=−0.354; d=0.37 [−0.21, 0.94], ADL: p=0.773; d=−0.31 [−0.88, 0.26], sport: p=0.938; d=−0.08 [−0.65, 0.49], quality of life (QOL): p=0.781; d=0.29 [−0.28, 0.86]) (figure 2C). Among athletes aged 35–54, mean KOOS scores for the Symptom and Quality of Life (QOL) subscale were lower in comparison to the general population (symptom: p=0.197; d=1.15 [0.66, 1.63]; QOL: p=0.312 d =1.03 [0.54, 1.51])31 (figure 2D). Large effect sizes were not detected for other KOOS subscales between athletes and the general population when stratified by age.
Concussion history
Twenty-five players (34%; 1 rowing, 24 rugby athletes) were diagnosed with at least one concussion during their professional career (average 2±1). Forty respondents (54%) reported suffering a suspected concussion but were not formally diagnosed by a medical professional.
Mental health
Anxiety and depression
Six respondents (8%) reported current moderate to severe anxiety with a GAD-7 score of 10 or more compared with 31% of Canadian women aged 15–65 (n=10 698) who reported moderate to severe anxiety in a 2020 survey.32 Unadjusted and age-adjusted analyses showed that athletes had significantly lower odds of having anxiety compared with the general population (crude OR: 0.19 [0.08–0.45], p<0.0001]; age-adjusted OR: 0.16 [0.06–0.38], p<0.0001; h=0.61).
Five respondents (7%) reported current moderate to severe depression with a PHQ-9 score of 10 or more compared with 8% (n=108) in the Canadian general population from the 2017 to 2018 Canadian Community Health Survey.33 Unadjusted and age-adjusted analyses showed that athletes had lower odds of current depression, but these results were not significant (crude OR: 0.86 [0.34 to 2.17], p=0.7467; age-adjusted OR: 0.75 [0.26 to 2.14], p=0.5903; h=0.04). We also asked, ‘While competing with the national team, did you ever want or need support from a psychologist or psychiatrist for personal mental health?’ and 22 (30%) responded yes.
Harassment and abuse
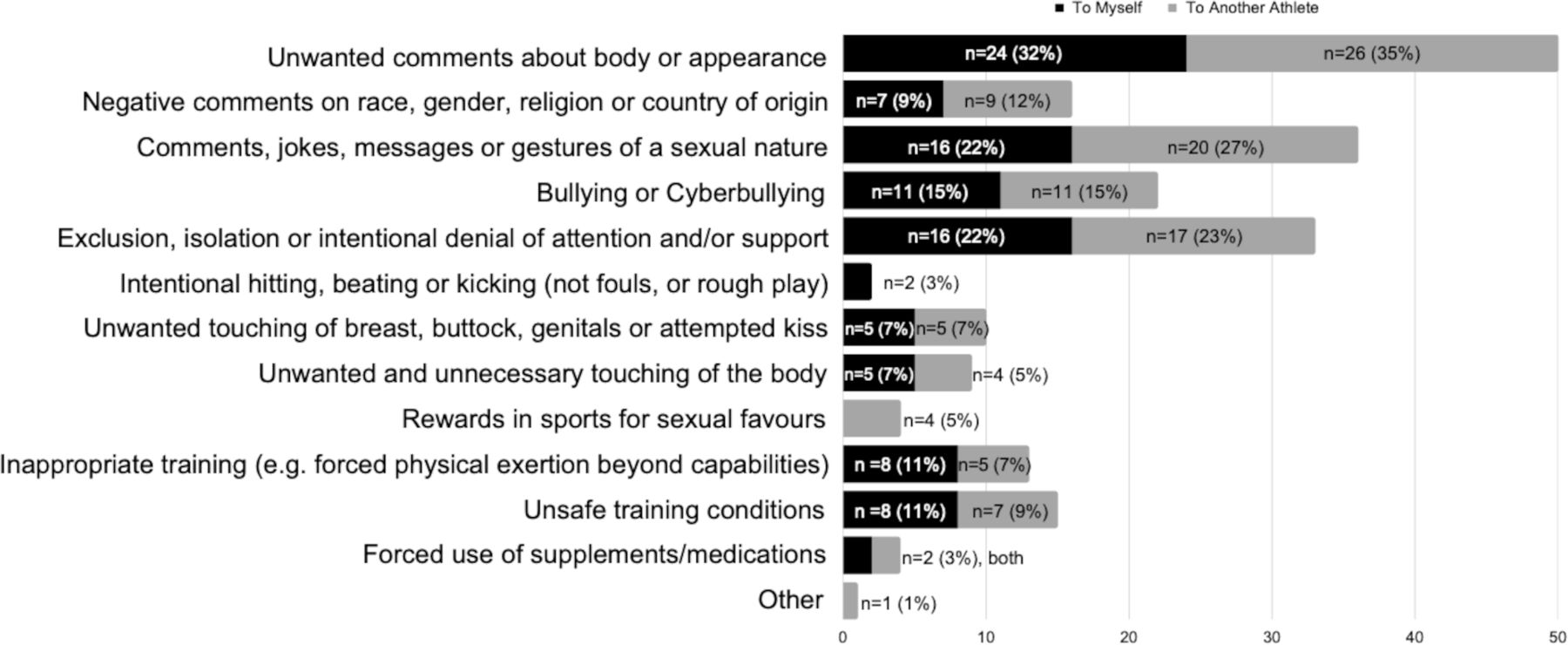
Fifty-nine respondents (80%) indicated that they experienced or witnessed at least one type of harassment and/or abuse (figure 3). Unwanted comments about athletes’ bodies or appearances were most often perpetrated by a coach (24 (32%) experienced; 26 (35%) witnessed), followed by peer athletes. Twenty-five respondents (42%) identified a family member or friend to be the perpetrator, 7 (12%) an official and 27 (46%) did not identify the perpetrator.

Number of respondents who reported experiencing each type of harassment and/or abuse themselves or witnessed it occurring to another athlete.
Reproductive/endocrine health
Seven (9%) respondents reported a reproductive or endocrine disorder diagnosis, including polycystic ovarian syndrome, fibroids, subfertility, uterine septum and endometriosis. Six (8%) respondents reported thyroid disease and one (1%) reported a diagnosis of breast cancer.
Disordered eating/eating disorder history and body shape satisfaction
Three respondents (4%) reported having an eating disorder diagnosis in their lifetime. When asked about body shape satisfaction, 38 (51%) reported being usually or always satisfied with the shape of their body. Twenty respondents (27%, 13 rowing athletes, 7 rugby athletes) reported that a coach or staff member suggested they lose weight. Nearly half (45%) of the time it was suggested for a specific performance or health-related reason and nutritional support was subsequently offered.
Menstrual history
Fifty-five respondents (74%) reached menarche between the ages of 12–14 years, consistent with general population data.34 Thirty-three respondents (45%) experienced amenorrhea (cessation of menstrual cycles for at least 3 consecutive months) outside of pregnancy. Rugby players were 88% less likely to experience menstrual irregularities than rowers (OR=0.12 [0.03 to 0.47]; p<0.001; h=0.82).
Compared with the general population, athletes had higher age-adjusted odds of ever having oligomenorrhea, (OR=1.65 [0.78 to 3.48], p=0.177; h=0.16) and significantly higher odds of ever experiencing amenorrhea (OR=6.10 [2.67 to 13.96], p<0.0001; h=0.52).35 Of the 17 respondents who had reached menopause, the mean age of first symptom onset or diagnosis of menopause was 48.2±3.3 years. This is younger than the general Canadian population mean age of natural menopause of 51 years,36 although data on first symptom onset are not available.23
Pregnancy history
Sixteen (22%) respondents never tried to conceive, 47 participants (65%) delivered at least one child (see online supplemental table S2), 6 (8%) were unable to conceive, 5 (7%) had not carried a pregnancy to term. Of the 47 who delivered at least one child, 6 (8%) reported difficulties conceiving (requiring fertility treatments) but eventually delivered a child. Most respondents gave birth after retiring from sport, however three rugby players gave birth during their competitive career. The average age of first-time mothers was 33 years old (range 27–43 years old), 3.5 years older than the general population (29.4 years).37 There was a greater percentage of athletes reporting twin pregnancies (p=0.0157), and fewer reporting gestational diabetes (p=0.0016), postpartum depression (p=0.0015) or urinary incontinence (p=0.024) than the general population (figure 4).
Supplemental material

Percentage of respondents who reported experiencing conditions during pregnancy, delivery or postpartum compared to samples from the general population. an=50 for the current study sample (47 respondents who delivered a child and 3 respondents who were pregnant at the time of completing the survey). bn = 47 for the current study sample (47 respondents who delivered a child). *p < 0.05.
Cardiovascular health
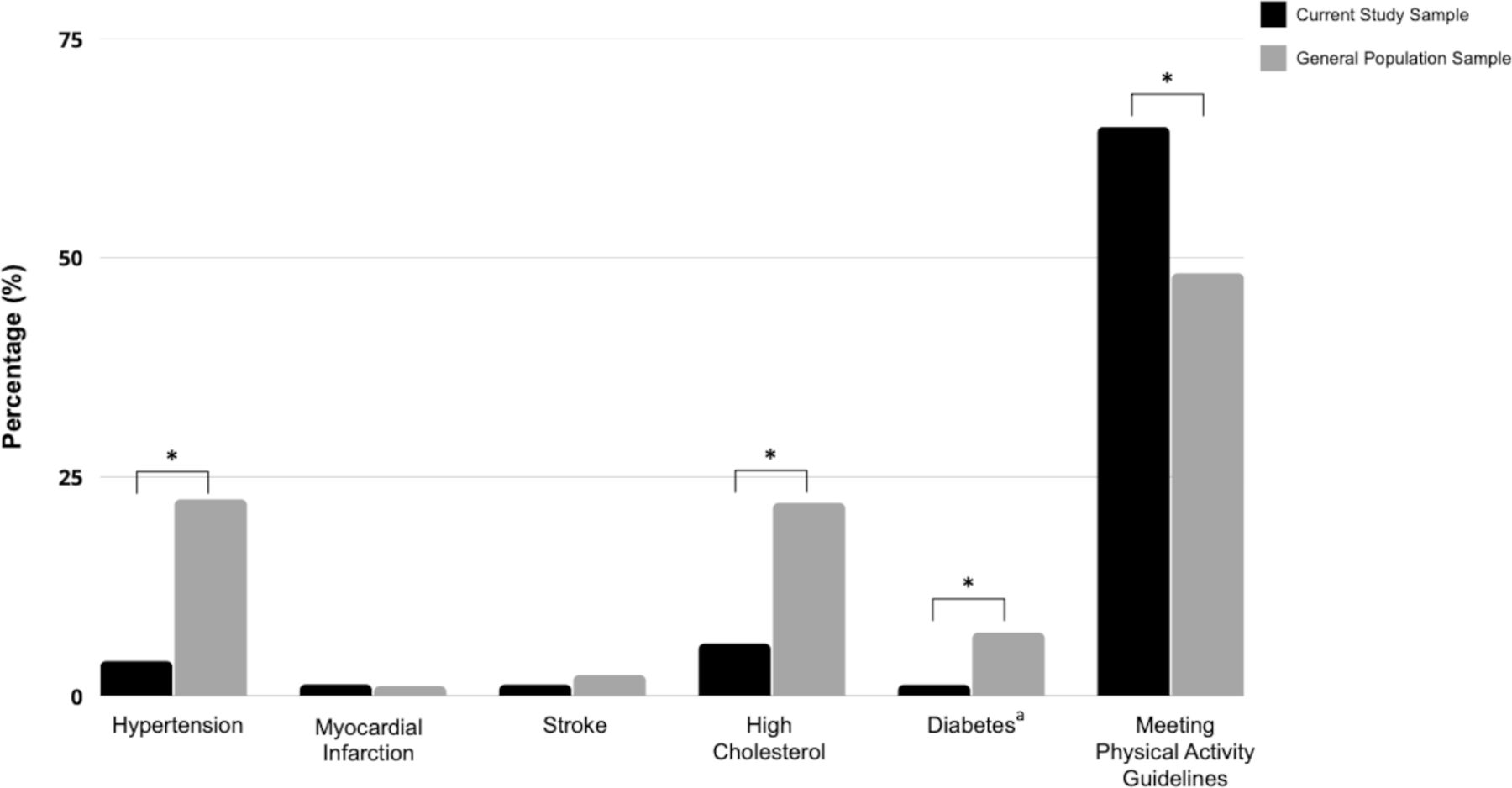
The proportion of participants meeting physical activity guidelines was significantly higher than the general population (p=0.0041), though once adjusted for age, there was no significant difference observed in the odds of meeting physical activity guidelines between retired female athletes and general Canadian population (age-adjusted OR=1.44 [0.88 to 2.32], p=0.1400; h=0.34) (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of respondents who reported cardiovascular conditions or reported meeting current physical activity guidelines compared to the general population. aType 1 and type 2 diabetes included. *p < 0.05.
There were fewer athletes reporting hypertension (p<0.0001), high cholesterol (p=0.0009) and diabetes (p=0.0496) than the general population.
Self-reported quality of health
When reflecting on their time on the national team, 62 respondents (84%) rated their general health as above average or excellent. At the time of retirement, this number fell to 53 (72%); and for current health increased again to 60 (82%). Summaries of open-ended responses about self-rated health are presented in table 2. Respondents cited that the training environment, team culture, teammate and family support were positive external influences on their health, whereas the lack of financial resources had a negative external influence (see table 3 for examples). They recommend rookie athletes, however, prioritise injury prevention and recovery over performance (table 4).
Summaries of open-ended responses about self-rated health currently and recalled immediately post-retirement, and during training and competition
Summaries of open-ended responses about positive and negative external influences on health
Summary codes, frequencies and illustrative quotes for advice to rookies
Discussion
This is the first known study to explore post-retirement reproductive, endocrine and cardiovascular health characteristics in a female elite athlete population. This study adds to the understanding of MSK and mental health characteristics following elite rowing and rugby participation. Novel insights were gained regarding retired female athletes’ perception of their participation in elite sport and its impact on their overall and current health. Retired elite rowers and rugby players reported above average to excellent health and if given the choice, would compete again. They recommend rookie athletes, however, prioritise injury prevention and recovery over performance.
Sports-related injuries and MSK health
Retired female athletes rated MSK health as a priority topic in retirement. We chose to include recording of ‘milder’ injuries that typically resolve in under 4 weeks (sprains/strains/concussion but which still may have had a devastating effect on competitions), as well as ‘ability to perform’ to capture those whose injuries may have allowed them to return to sport, but not to the same level they were accustomed to. Injuries sustained during respondents’ careers resulted in no difference in pain or activities of daily living in retirement than a general population comparator. However, other symptoms (clicking, stiffness etc.) and lower QOL scores were reported more often in athletes aged 35–54. These findings contrast with previous studies on retired male elite rugby players38 and professional male football and rugby athletes that reported a higher prevalence of OA than when compared with the general population.39 As well, in a survey of retired male and female Olympians it was reported that 40% of the respondents reported functional limitation from sport-career injuries.40 Respondents in our study were physically active, non-smokers and generally free of cardiovascular disease. As osteoarthritis is a multifaceted disease that results from both mechanical and metabolic processes,41 respondents’ general good health may have mitigated poor MSK characteristics. Prior studies38 40 42 did not report on smoking status, physical activity levels or cardiovascular disease, therefore further research is needed to establish associations.
High rates of concussion in rugby players highlight a need for further research into long-term cognitive health in this population. There was also a high rate of reporting concussions without formal diagnosis, which should be further explored. This may reflect lack of awareness of the diagnosis and/or repercussions, particularly in those athletes who retired many years ago. Female athletes are at a higher risk of a concussion, and this may increase their predisposition to adverse long-term cognitive and neuropsychological outcomes post-retirement.5 While female football players typically outperform the general public in cognitive testing,43 retired female athletes with a greater relative frequency of heading the ball and a history of multiple diagnosed concussions scored lower on verbal memory and fluency cognitive performance tests than their age-matched controls.5
Mental health during the transition from sport into retirement
The lower rates of anxiety and similar rates of depression reported by our respondents compared with the general population are consistent with a recent systematic review and meta-analysis that noted lower rates of anxiety and depression in former elite athletes (26%) than in current athletes, yet slightly above the general population.44 We gained further insights from the open-ended questioning in our retired athletes, with many reporting that their mental health suffered at the time of retirement; one athlete described being ‘mentally shattered’ despite a high level of physical fitness. Transition out of sport can be accompanied by a loss of identity and with resultant impacts on mental health sequalae,45 and healthcare providers and sport organisations have a duty of care to support end of career transition from sport.
Harassment and abuse
Nearly half of our participants reported that harassment and/or abuse was either likely or very likely in their sport, consistent with a similar survey study of male and female elite aquatic athletes.46 This finding underscores a need to increase efforts to protect female athletes from a hazard to their mental18 and physical health. Addressing abuse and harassment is a critical priority, and all members of sport have a duty of care to ensure a safe sporting environment. Female athletes have been identified as being particularly vulnerable to gender-based violence in sport. The IOC Consensus statement on harassment and abuse (non-accidental violence) provides several recommendations for action specific to sport organisations, healthcare providers, researchers and athletes.47 Future studies should explore harassment and abuse and their long-term effects on mental health.
Reproductive and endocrine health
Amenorrhea was common (45%) in our respondents, but the long-term effects on injury risk, fertility, physical and mental health for retired athletes were unknown. The presentation of RED-S may be unrecognised by athletes and coaches.48 For example, one athlete described struggling with ‘low iron/ferritin, stress fractures, overtraining, and low body fat levels, which I feel all impaired my performance and tolerance of the training load’, although RED-S was not specifically reported by any athlete. Lack of awareness and support surrounding reproductive and endocrine health was a recurring theme from our participants and should be prioritised via educational initiatives, periodic health evaluations, and counselling.
The IOC Expert Group on exercise and pregnancy in recreational and elite athletes indicated that studies of the reproductive health of retired and active elite female athletes are a priority.14 In our participants, the high rates of amenorrhea, older age at childbirth and trend towards earlier symptoms/onset of menopause may denote a narrower ‘reproductive window’ for female athletes warranting further investigation.
Retired athletes who desired to be parents face a difficult choice. Calls for better supports for elite athletes have been made13 49 including providing education about pregnancy and fertility options during and after athletes’ sports careers and are strongly recommended. By doing so, athletes can make informed decisions about their reproductive health.
Cardiovascular health
The impact of intense athletic training on the female heart is relatively unknown. Male endurance athletes have an approximately five-fold higher risk of AF, along with higher rates of arrhythmias and other cardiac findings than male non-athletes.16 In our study, 2/74 (3%) respondents reported AF, in line with other research,50 yet both were rowers—representing 7% of this group. In contrast, one study examining sex differences in AF rates in cross-country skiers demonstrated that female skiers had a lower incidence of AF and stroke than the general population .51
Our study adds much needed information on the cardiovascular risk profile of the female athlete, finding similar results to prior findings in male athletes.52 Physical activity levels can drop precipitously after transitioning out of sport,53 but in our population, physical activity levels remained high and may partially account for their healthy cardiovascular risk profile. More studies are needed so that athletes can make informed decisions about long-term implications of training on their cardiovascular health.
Strengths and limitations
The athlete voice and context45 are strengths of this study, as we sought the experiences of athletes via open-ended questions and pre-tested our survey with athletes prior to data collection. Limitations include the small response rate and large time frame since retirement which made it difficult to detect statistically significant differences in some characteristics. As effect size is independent of sample size, the present study reported the substantive significance to ascertain public health relevance and/or clinically significant findings. The detection of large effects between groups is supported by high statistical power regardless of the small study sample. The largest observed non-significant findings should be considered for inclusion in larger definitive studies. The retrospective nature of cross-sectional surveys may introduce recall bias, and current symptoms may be falsely attributed to previous injuries. This survey relied on self-reported physical activity and health, outcomes, whereas objective measures and prospective study designs would strengthen findings. The dichotomization of overall from the 5-item Likert scale resulted in a loss of information but allowed for the investigation of the association between elite sport and higher rated health.
Clinical significance
For longer lasting, healthier and more satisfying athlete careers, clinicians and sport stakeholders should consider holistic athlete health, during and after athletes’ careers. Clinicians have a duty of care to help support a healthy interpersonal environment54 and sport culture including asking about mental health concerns, harassment and abuse. Clinicians should similarly promote healthy eating behaviours and adequate energy intake, and long-term reproductive health and pregnancy planning as needed—these conversations should begin during an athlete’s career and include education and resources. After-career support can play a pivotal role for female athletes during the transition to retirement to promote healthy behaviours55 including counselling on physical activity levels, mental health, rehabilitation of unresolved MSK injuries and reproductive health as indicated. Larger prospective studies are needed with objective measures, as are trials including co-designed interventions to address priority areas.
Several key areas of retired female athlete health warrant further attention to address current gaps in knowledge including the long-term effects of injuries sustained during female athletes’ careers, RED-S and fertility characteristics and the effect of intense training on cardiovascular health. Further research findings and policy work should also target mental health during the transition from sport, as well to mitigate reporting of harassment and abuse, and concussion. Finally, researchers should focus on athletes’ reasons for retirement, as these may have affected their personal experience during their transition from elite sport.
Conclusion
This is the first study to explore post-retirement health characteristics in several key areas of female athlete health, namely reproductive, endocrine and cardiovascular health. Retired elite rowers and rugby players reported having above average to excellent health and if given the choice, would compete again. We identified several female athlete health domains that deserve further attention to ensure long-term athlete health including the long-term effects of injuries sustained during female athletes’ careers, RED-S, fertility characteristics and intense training on cardiovascular health. Our findings point to a critical need for increased injury prevention and health protection efforts during a female athlete’s career, at the time of transition out of sport and beyond (box 1). By increasing our understanding of long-term health in female elite athletes, sport organisations, stakeholders and healthcare providers will be better equipped to support these athletes during and after their careers, where the effects of intense training may impact them the most.
Recommendations for sport stakeholders to improve post-retirement health in female athletes via the socioecological model56
Individual level—athletes: connect with former and current athletes about health questions and concerns throughout competitive years. Consider reaching out to a healthcare provider for education and resources on post-retirement health. Report harassment and abuse when it happens. Adopt healthy lifestyle behaviours including physical activity post-retirement.
Interpersonal level—coaches/parents/teammates: implement and encourage effective injury and illness prevention strategies during athletes’ careers. Emphasise mental health as a key component before and after retirement. Ensure a Safe Sport environment through policy development and implementation, reporting mechanisms, and victim support services. Support safe postpartum and post-injury return to sport.
Interpersonal level—physicians and healthcare providers: normalise discussions about female health considerations, including menstrual health, pregnancy and parenting, at each stage of an athlete’s career; advocate for better sport policy for athletes who wish to become pregnant and stay in their sport; and consider offering post-career health consultations for relevant physical and mental health issues.
Interpersonal level—strength and conditioning coaches and trainers: help athletes set physical health goals as they transition out of competition.
Organisation level—managers: provide financial support for third-party health counselling and career counselling for athletes. Sport organisations: establish support groups or networks in retirement for elite female athletes, establish Safe Sport policies to raise awareness and prevent harassment and abuse. Ensure fair pregnancy/postpartum policies and adequate financial support.
Community level—prioritise injury and illness prevention during athletes’ careers.
Policy level—create and promote Safe Sport policies to prevent and decrease abuse and harassment, and injury prevention policies (eg, concussion prevention and awareness). Ensure fair pregnancy/postpartum policies and adequate financial support.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study received ethics approval from Western University’s Research Ethics Board (number 118403). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JaneSThornton, @margo.mountjoy, @VGouttebarge
Contributors JT had the idea for the study, conducted the literature search, prepared the original draft and is the guarantor. PD, MD, VG, MLM and KC provided expert insight into the development of the questionnaire. CR and SDC performed the data collection. JY, KM and MS conducted the data analysis. KR and EP performed data collection and analysis. All authors critically commented on previous versions of the manuscript and read and approved the final manuscript.
Funding This work was supported by the Sport Information Resource Centre Researcher/Practitioner Match Grant.
Competing interests JST is an Editor of the BJSM.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.