Article Text

Abstract
Objectives Healthcare is a fundamental action area in population efforts to address the global disease burden from physical inactivity. However, healthcare professionals lack the knowledge, skills and confidence to have regular conversations about physical activity. This study aimed to: (1) understand the requirements of healthcare professionals and patients from a resource to support routine physical activity conversations in clinical consultations and (2) develop such a resource.
Methods This study used codesign principles across two phases, actively involving relevant stakeholders in an iterative development process. The preparatory phase included a scoping literature review and workshops with multidisciplinary healthcare professionals and patients. The Delphi phase included the development of a draft resource, a three-stage modified online Delphi study and an external review.
Results The scoping review highlighted the importance of addressing time restrictions, a behaviour change skill deficit, the need for resources to fit into existing systems and meeting patient expectations. Consultation included 69 participants across two clinical workshops. They recommended using the internet, valued guidance on all aspects of physical activity conversations and were concerned about how to use a person-centred approach. The Delphi phase, including 15 expert participants, met agreement criteria in two stages to develop the resource.
Conclusion This mixed-methods study delivered an online resource that was codesigned with and based on the requirements of healthcare professionals and patients. The resource presents condition-specific ‘1-minute’, ‘5-minute’ and ‘more minute’ person-centred and evidence-based conversation templates on physical activity in an accessible and usable format to meet the needs of real-life clinical practice.
- Exercise
- Physical activity
- Behaviour
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Healthcare professionals are essential contributors to population efforts to increase physical activity.
The physical activity knowledge, skills and confidence of healthcare practitioners are low.
There is a lack of physical activity tools and educational resources available to help healthcare professionals.
WHAT THIS STUDY ADDS
Healthcare professionals want in-depth evidence on physical activity and specific conditions to be available and presented in an accessible hierarchy using hyperlinks on a web platform so they can choose what they need.
‘1-minute’, ‘5-minute’ and ‘more minute’ person-centred conversations are flexible enough to meet the demands of healthcare professionals and patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
The resource developed during this study will help healthcare professionals talk to people about physical activity and is freely available online at www.movingmedicine.ac.uk
Future research should seek to test the resources developed during this study to determine efficacy and help improve the format and function of resources to better support conversations on physical activity in the management of long term conditions.
Comprehensive evaluation is required of system-wide implementation projects to understand how to use these resources to improve continuity and support people as they journey through healthcare services in their long-term management of health conditions.
Introduction
A strong and rapidly developing body of evidence defines the health risks of physical inactivity and the role of therapeutic physical activity in treating chronic medical conditions.1–3 The WHO recognises physical inactivity as the fourth leading risk factor for global morbidity and premature mortality, being directly responsible for 6% of deaths globally4 and the cause of more deaths than smoking.2
Healthcare is a fundamental component of population-level approaches to addressing the inactivity burden and is essential due to the sector’s contact with, and potential to influence, people living with health conditions.5 6 Individuals living with health conditions are among the least active in society and generally become even less active following diagnosis.2 Consequently, this group stands to gain the most from even small increases in physical activity to treat existing and prevent new medical conditions.7
Healthcare professionals are a central part of the systems-wide approach required to drive change and improve the delivery of physical activity.6 8 Routine person-centred conversations between healthcare professionals and their patients offer a vital intervention area.9–13 Healthcare professionals repeatedly report lacking the skills and confidence required to effectively counsel people living with a health condition on physical activity.14–21
There is a lack of tools and education platforms to operationalise physical activity conversations in healthcare.18 22 Furthermore, generic resources and efforts to improve behaviour change skills in other domains such as smoking cessation and weight loss do not appear to translate to improved physical activity confidence and skills.23 24 Meaningful patient involvement in quality improvement initiatives helps drive quality and innovation and is recommended for novel approaches to clinical resource development.25 Codesign (also called coproduction or cocreation) is an approach that focuses on actively involving all relevant stakeholders to help ensure a design process meets their needs so that educational resources and service provision models are usable in real-life scenarios.26 27 Codesign principles were used in this study to address the following aims:
Understand the requirements of healthcare professionals and patients from a resource to support routine physical activity conversations in clinical consultations
Develop and test such a resource.
Methods
Study design
Two study phases, reflecting the two study aims, are outlined in figure 1. To understand the requirements of healthcare professionals around physical activity conversations, the preparatory phase included a scoping literature review and consultation workshops with multidisciplinary healthcare professionals and patients. The Delphi phase aimed to iteratively develop and test such a resource over three rounds.
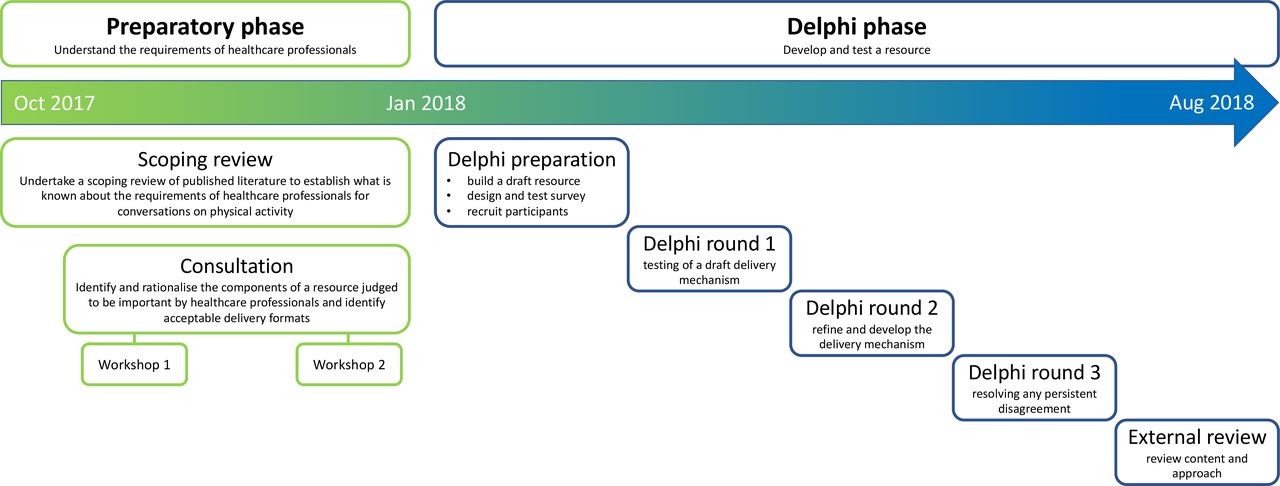
Structure and objectives of each Delphi study phase.
Codesign principles were employed throughout, engaging multidisciplinary healthcare professionals who will use the resource and people living with medical conditions with whom the healthcare professionals will use it. The Delphi method was chosen for its ability to collate a diverse set of expert opinions anonymously and without social pressure or a ‘bandwagon effect’.28 29 Codesign enabled the Delphi phase of the study to focus on the iterative development of a resource that repackaged the physical activity evidence base into a clinically relevant and accessible format with input from a range of stakeholders through the generation of ideas and solutions rather than just in-depth analysis.30–32
Patient and public involvement
Patient representatives identified through patient support groups of local charities attended the workshops. In the workshops, they were spread between groups to help understand and discuss the balance of perspectives required for conversations on physical activity in clinical practice. Their opinions directly informed resource design, and they subsequently contributed to external review and the development and dissemination of patient-facing information resources.
Preparatory phase
Scoping review
We undertook a scoping review following the five-stage protocol by Arksey and O’Malley reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews checklist.33–35 The review explored published literature, guidelines and online resources, aiming to gain a broad overview of the context of physical activity consultation in healthcare. It addressed two research questions: (1) what is known about the effectiveness and acceptability of physical activity consultations in healthcare? and (2) what is known about strategies to implement routine physical activity conversations in healthcare?35
Consultation
We led two focused, interactive workshops informed by results from the scoping review (see online supplemental file 2). The workshops aimed to identify and rationalise the components of a resource judged to be important by healthcare professionals and identify acceptable delivery formats. Through professional contacts, we identified two multidisciplinary regional specialist networks to participate in the workshops. The first workshop focused on inflammatory rheumatic disease and the second on musculoskeletal pain. We summarised results from the workshops and organised them thematically to inform the development of a draft resource in the Delphi phase.
Supplemental material
Delphi phase
We used a modified electronic Delphi process to collect data from remote contributors and facilitate automated data collection.36 37 We used the commercial software ‘SurveyMonkey’38 for the survey rounds and followed the Conducting and REporting Delphi Studies guidelines throughout.32
Building a draft resource
We commissioned a design agency and gave them a design brief based on findings of the preparatory phase. Design agency members also attended preparatory phase workshops to improve their understanding of the content and objectives. We developed a wireframe draft resource in conjunction with the design team through meetings, phone calls and email communication. The wireframe resource enabled the exploration of content, navigation and function during round 1 of the Delphi study without requiring the investment of a complete website build.
Developing and testing the survey
We developed and tested an online survey based on the structure and content of the wireframe resource, which reflected the development priorities outlined during the preparatory phase. Three clinicians not involved in the study piloted the survey before distribution to ensure usability by testing the structure and wording.28 39 We kept the completion time target below 30 min to reduce participant fatigue.40
Participant recruitment
We formed an expert panel by purposive sample to generate a deliberately heterogeneous group of multidisciplinary participants with expertise covering healthcare, physical activity, behavioural change and digital education.
According to recommendations for a Delphi study requiring in-depth feedback and continuity, 15 is a sufficient number of participants.31 41 42 We identified potential participants through professional and academic networks and established research interests with relevant publications. We invited participation by direct email, and where participants did not reply to the initial contact, we sent one further invitation email.
Following round 1, we contacted all participants by email and invited them to participate in round 2. In addition, three reminder emails were sent out for those who had not completed the second-round questionnaire: (1) a repeat of the initial invitation 2 weeks before the survey closing, (2) a reminder at 1 week and (3) a final reminder 2 days before survey closure.
Delphi rounds
Round 1 of the online Delphi aimed to test the structural components of the wireframe website and appraise preliminary design concepts. Round 2 involved testing a website built following round 1. Finally, round 3 enabled the resolution of any persistent disagreement if necessary.
Between-round feedback
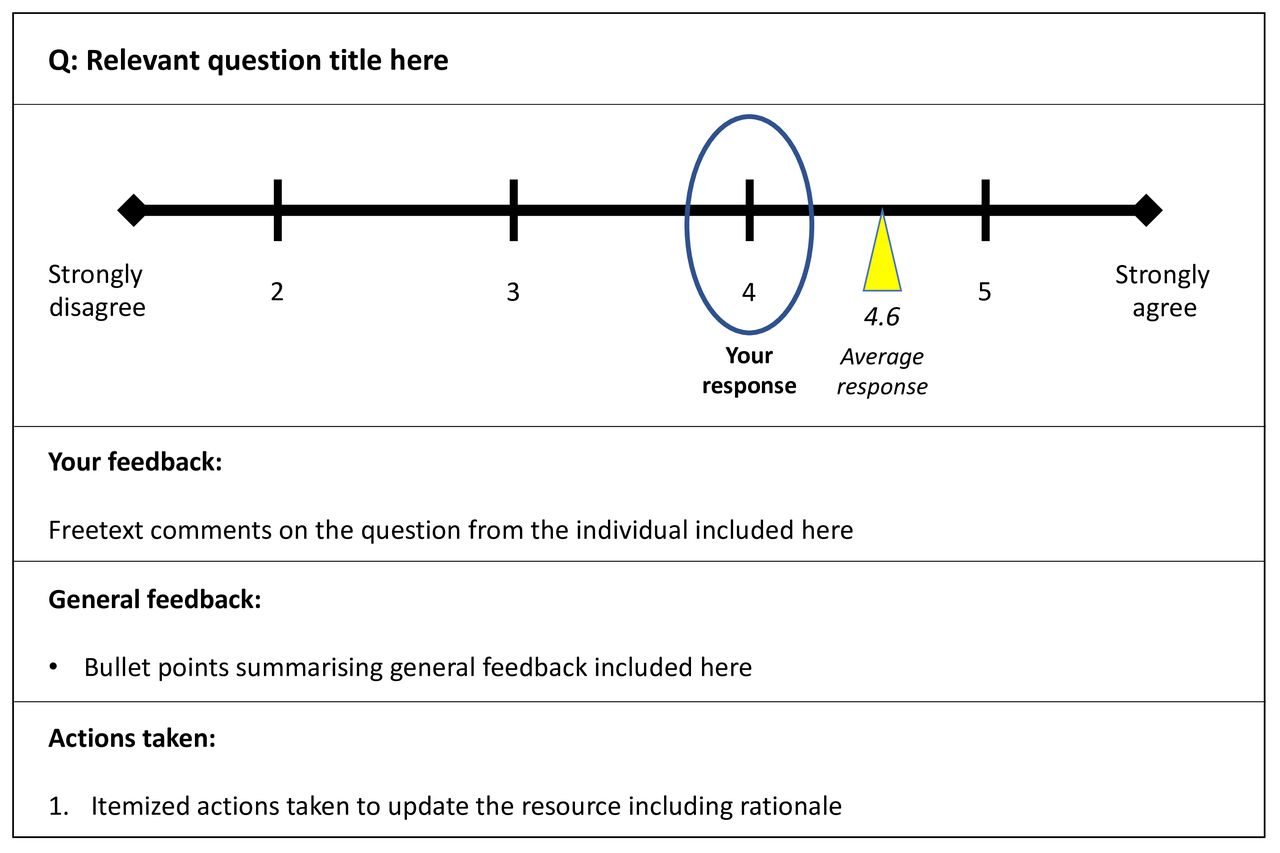
Following each round, we prepared and distributed individualised feedback comparing individual responses to the group average for each question. This was a straight reproduction of the participant’s own words to avoid biasing responses in subsequent rounds.42 We also provided all participants with a summary of free-text feedback and a comprehensive list of and rationale for all actions taken (see figure 2).

Format for individualised feedback on each question.
Delphi consensus criteria
In keeping with described methods,32 39 42 we defined satisfactory agreement (consensus) ‘a priori’ according to the criteria outlined in figure 3.

Definitions of consensus in each phase of the Delphi process.
External review
We identified three external groups to review the Delphi study’s outputs and circulated resources electronically to these groups after completing the Delphi rounds requesting open-text feedback via email. The objective of this feedback was to review the content and assess the feasibility and applicability of the approach recommended by the Delphi group. The groups were:
An academic external validation group appointed through the Moving Medicine initiative.
Funding and commissioning bodies at the Faculty of Sport and Exercise Medicine, Sport England and Public Health England.
Collaborating professional bodies including the Royal College of Physicians, Royal College of Nurses, Royal College of General Practitioners, Chartered Society of Physiotherapists, Academy of Medical Royal Colleges, the British Association of Sport and Exercise Medicine and the patient representatives of charities who had participated in the working groups.
Results
Preparatory phase
Scoping review
The scoping review identified 616 references for screening (n=596 from databases and n=20 from hand searching). Following screening and removal of duplicates, 48 studies were included for analysis. Narrative results were synthesised thematically as they emerged from the data.35 Online supplemental file 1 presents a summary of relevant findings.
Supplemental material
Consultation
A total of 70 attendees took part in the face-to-face clinical workshops that took place in Oxford (autoimmune rheumatic disease) and Birmingham (musculoskeletal pain) in 2018 (see table 1). Healthcare professionals from a range of rheumatology, musculoskeletal and chronic pain services across England attended the workshops. The groups included doctors, nurses, physiotherapists, clinical academics and medical students. In addition, we identified patient representatives through local patient groups from the National Rheumatoid Arthritis Society and the Arthritis and Musculoskeletal Alliance, an umbrella body in the UK connecting patient organisations and professional bodies across musculoskeletal health. Design and communication specialists from the project design team also attended. See online supplemental file 2 for more detail.
Professional mix in the preparatory workshops
As outlined in table 2, the headline themes identified were components to support healthcare professionals directly, clinical considerations for translating evidence into practice and developing a mechanism to support access to knowledge in routine clinical care.
Summary of consultation workshop recommendations
Delphi phase
Building a draft resource
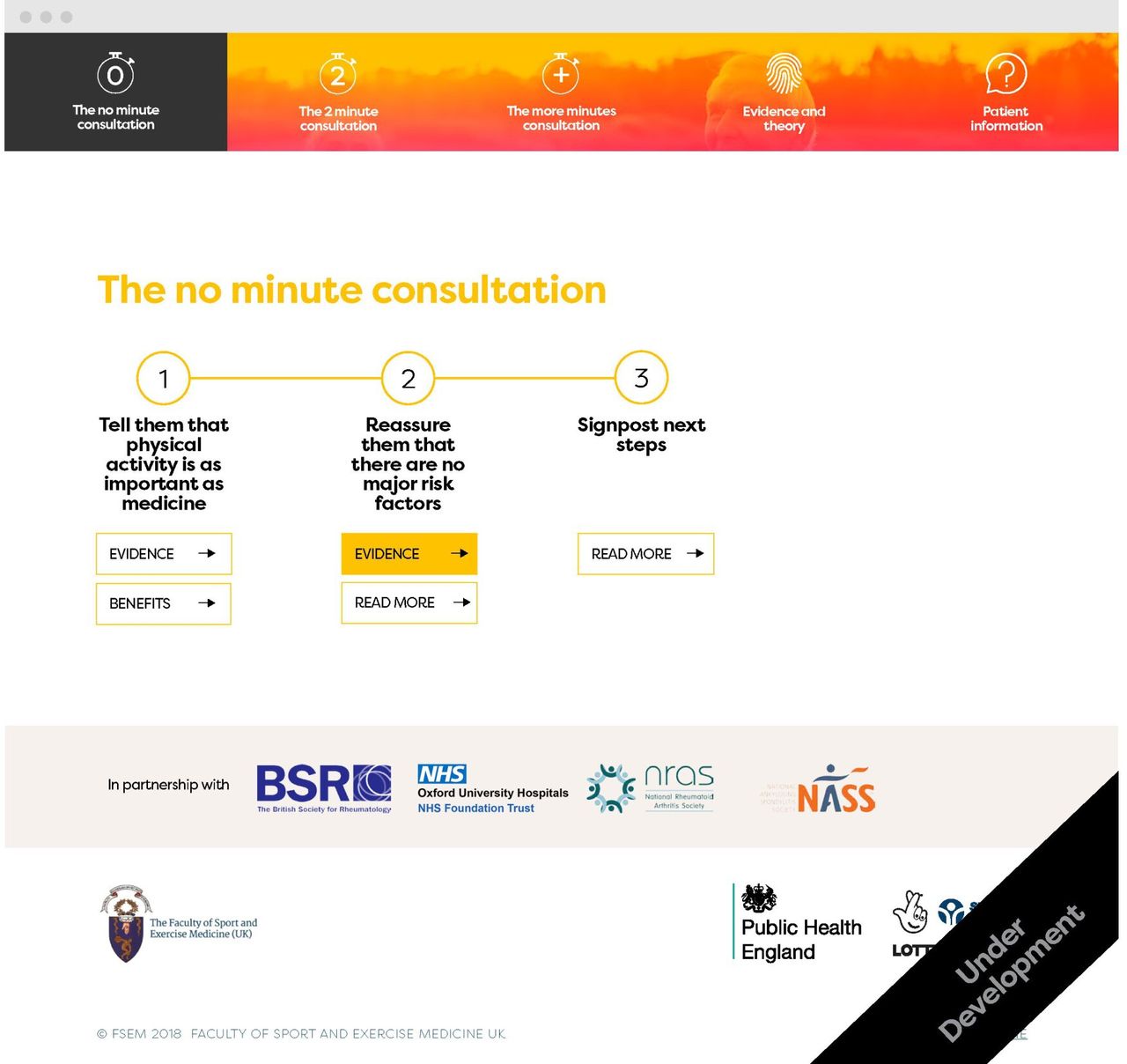
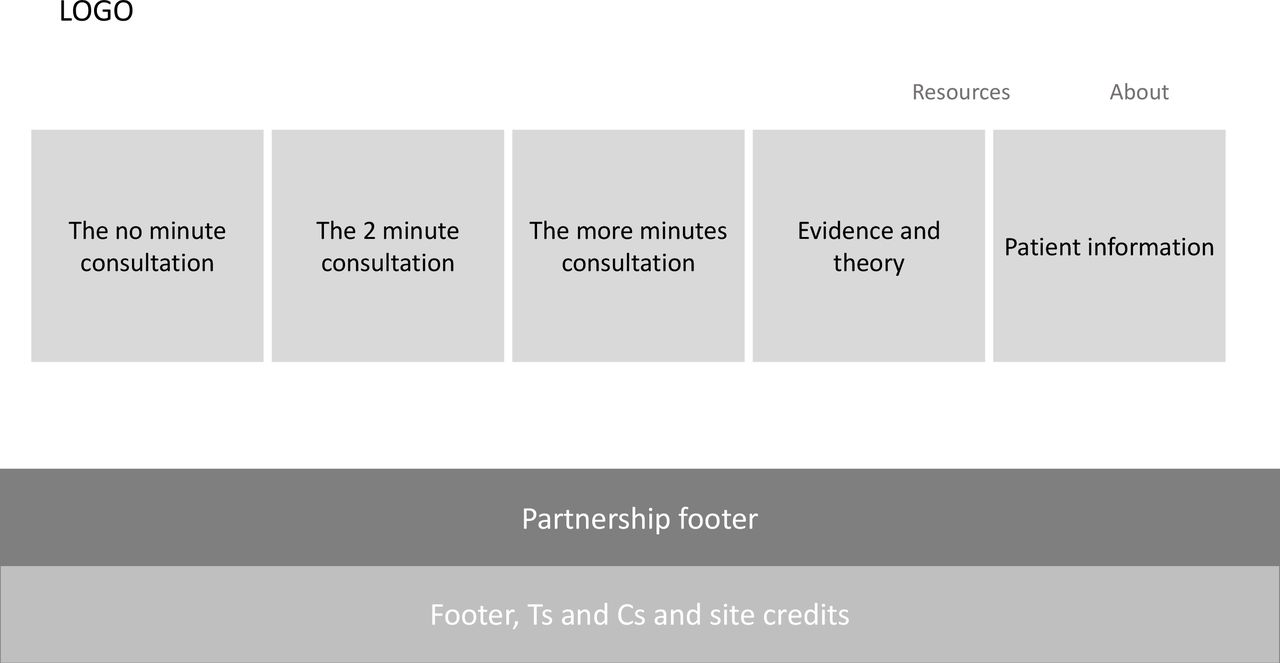
Workshop participants identified the internet as an acceptable and scalable environment to host a resource to support conversations in everyday clinical practice. Using a website also enables delivery of the complexity of information identified as necessary. Table 3 maps preparatory phase recommendations onto solutions generated during the iterative build of the wireframe website (see figure 4).
Generating design solutions from preparatory phase recommendations

Landing page for the UX-PIN wireframe website.
Developing and testing the survey
We identified the following problems during survey piloting:
Errors in question format, including mistakes in a matrix table
Confusing question layouts when viewed on mobile devices.
Testing recommended that the classically used nine-point scale as per the original RAND UCLA method32 39 was an inappropriately long set of numbers for the digital screen. We selected a six-point scale instead, with the added advantage that it obliged participants to commit to either agreeing or disagreeing with statements.
Navigation of the wireframe website confused users, so we included images with detailed instructions to improve navigability.
Participant recruitment
We contacted 29 individuals, and 19 agreed to part-take in round 1 of the study. Only 15 of 19 participants completed the survey in round 1 despite reminder emails, so only these participants were sent the round 2 survey. Ten of 15 of these participants responded to the round 2 survey. Table 4 demonstrates participant demographics.
Demographic and professional characteristics of Delphi expert panel
Delphi round 1
Overall, agreement levels were high in round 1 (see table 5, full results are available in online supplemental file 3). However, there were two instances of participants registering a score or set of scores out of keeping with their free-text responses. We contacted these respondents directly to clarify their responses, and in each instance, there was an error or misunderstanding. For example, one respondent answered the scale of 1–6 the wrong way around, and another failed to open the design mock-ups answering the design-specific questions on the strength of the wireframe website. These issues were rectified and were not ongoing issues for other participants.
Supplemental material
Overview of Delphi consensus results
We analysed and collated free-text responses thematically (online supplemental file 3). Where free-text responses were relevant but unclear or incomplete, we contacted the respondents by email and, in one case, telephoned to further clarify the meaning. Given the high levels of agreement, free-text responses identified most changes required following round 1. We made the following major changes following round 1:
Revision of the conversation thread to further encourage patient-led decision making incorporating motivational interviewing theory and focusing on a ‘guiding’ rather than ‘telling’ approach.
Shortening the ‘2 min’ conversation.
Inclusion of patient-facing outputs for clinicians to hand out.
Removal of the ‘theory and evidence’ page in favour of evidence statement ‘pop-ups’ to make navigation and accessibility more straightforward.
Inclusion of a pop-up for out-of-date browsers advising software update and optimisation for mobile devices to make usage less reliant on National Health Service (NHS) IT infrastructure.
Delphi round 2
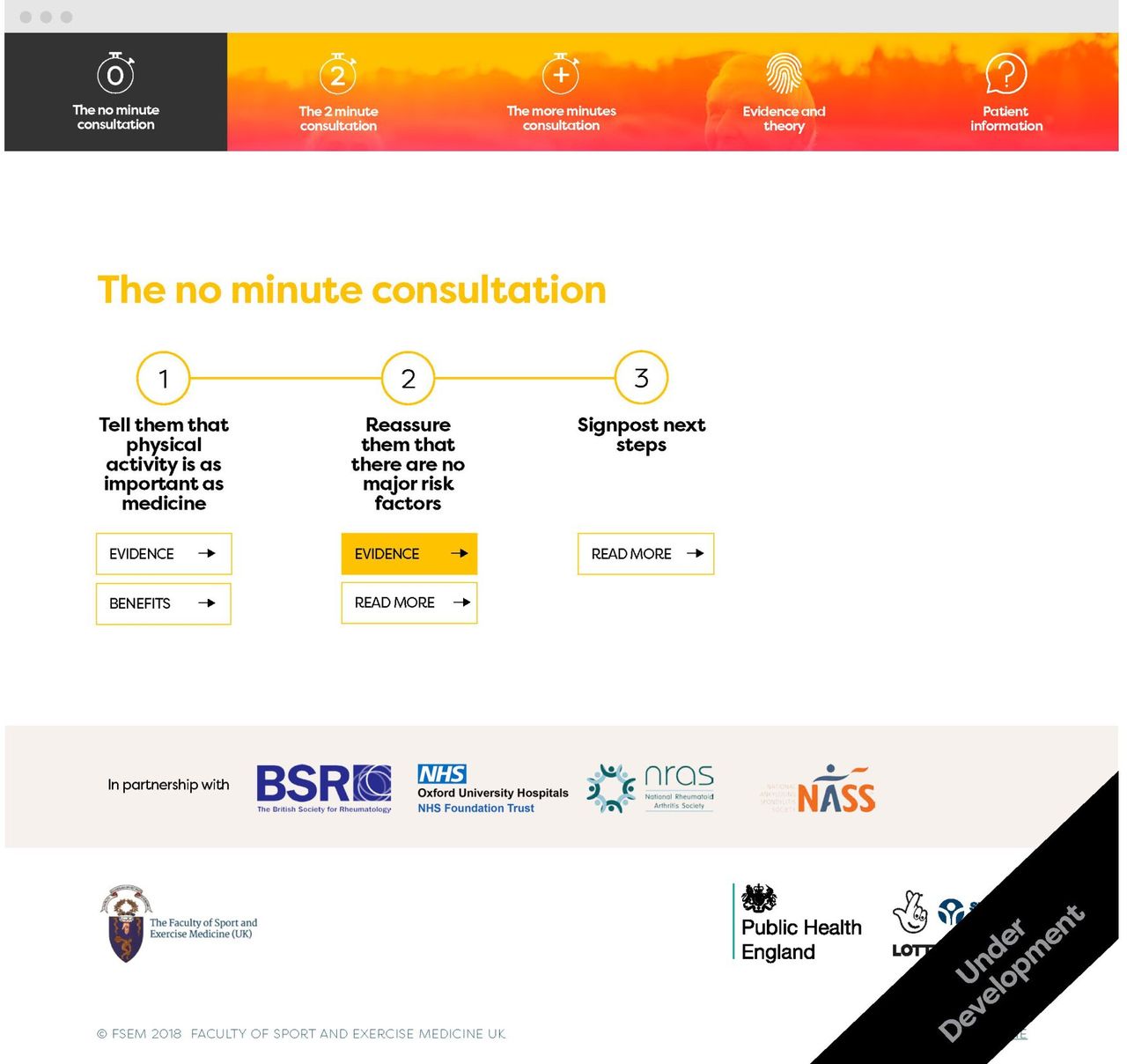
We built a draft website incorporating recommendations from round 1 for testing in round 2 of the Delphi (see figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Condition-specific landing page for a 0 min conversation on the draft website for phase 2.
Reflecting the high levels of consensus in round 1 of the Delphi (table 5), we dropped 10 questions for the second survey. However, despite achieving consensus in round 1, we repeated question 11 because of significant changes to the relevant content due to free-text feedback.
In round 2, 12 consensus areas achieved high agreement, 6 moderate agreement and 1 low agreement. In addition, we observed moderate agreement for navigation, the achievability of content, the physical activity calculator and the signposting of organisations. See online supplemental file 4 for full results.
Supplemental material
Delphi round 3
The inclusivity of design elements recorded low agreement (59%) in round 2. Free-text responses demonstrated that this was because the draft website only included one image. We did this intentionally to reduce build complexity at the draft stage. Ultimate plans were for a socioethnically diverse photograph carousel to feature in the final site, but we did not share this detail with respondents through oversight. We informed respondents of this solution by email, who were satisfied with the approach, and we did not need to proceed to a formal third round of the Delphi.
We revised the website following the amendments suggested in round 2. We then shared the website with the Delphi participants via email, inviting them to comment on the revisions. We received no further comments.
External review
After completing the Delphi study, we distributed the website to the predetermined external review groups. We invited feedback via open comments by email. Responses were unanimously positive, and no content changes were recommended. We received advice on launch, dissemination and engagement.
Discussion
This mixed-methods study represents a unique effort to understand and address the requirements of healthcare professionals and people living with health conditions regarding conversations on physical activity in clinical practice. Results from an extensive preparatory phase, including scoping review and workshops, informed the development of an open-access online resource developed iteratively with expert Delphi consensus. The resultant resource combines published evidence, consensus opinion and practical advice from clinical specialists in a time-sensitive, person-centred, practical format to bridge the gap between evidence and clinical practice.
Codesign
Despite convincing evidence and numerous national guidelines defining the vital role of physical activity across UK healthcare,1–3 11 21 43–45 the translation of knowledge from research to clinical practice remains limited across professional disciplines.14–18 21 46 To address this, we employed codesign principles, which ‘offers the chance for clinicians to reconsider the purposes of medicine and for patients and other stakeholders to have their voices heard and respected’.47 We listened to a wide range of healthcare professionals and patients to understand clinical practice requirements.27 We interpreted this in the context of published evidence and recommendations to make a draft solution that we tested and refined through the Delphi study. This iterative, user-centric approach enabled us to create a novel person-centred solution designed to adapt to day-to-day practice challenges that are not just scientifically right but also responsive to real life.48 Our resource will help address the lack of tools and training opportunities on physical activity counselling for staff in the NHS and elsewhere.18 22
Undertaking codesign is challenging. We worked hard on finding a balance between the development of the delivery mechanism alongside the evolution of the content. At times, this confused participants and led to mixed survey responses. A strength of the Delphi process was the ability to gain clarity and consensus on a wide range of options taking into account various individual opinions.30
Structuring information
Integrating a design team from the outset enhanced the design process, helping make sense of feedback and translating it into functional solutions. For example, time is an ever-present barrier to conversations on physical activity,23 49 50 and user groups recommended addressing this barrier at the outset of a resource designed to support clinical practice. The Delphi group recommended a time-based approach on conversations templates of 1, 5 and more minutes, reflecting behavioural change approaches recommended by the National Institute for Health and Care Excellence (NICE)10 and other physical activity initiatives.21 Working through solutions to this with the design team enabled the production of practical solutions that we then tested and refined through the Delphi process.
Given the long list of components required by clinicians (table 2), we were unclear on how to prioritise information. Although a novel approach to conversational design, ranking systems are a recommended and successfully used tool in Delphi studies.51 52 We used a drag and drop mechanism to develop a practical conversation sequence combining all the workshop groups’ requirements, and a web-based solution helped us deliver on all aspects.6 53
The overwhelming volume of evidence around physical activity in the management of long-term conditions can present an imposing barrier to the practice of evidence-based medicine.54 Information is understood and retained better when delivered in small chunks following sound design principles.55 56 A web platform enabled the refinement of a system capable of publishing information in layers to address these two factors. An example was moving the supporting evidence base from long-text format to ‘pop-ups’ on the strength of Delphi feedback.
The Delphi group reinforced the importance of getting the wording right for a conversation guide to move away from a ‘telling’ language style and meet the healthcare requirements identified in the consultation phase. A traditional didactic style of consultation runs the risk of ‘victim blaming’ and fails to support successful behavioural change.48 This shift in approach can also help healthcare practitioners foster supportive relationships and facilitate improvements in care delivery, benefitting users outside the realm of conversations on physical activity.57
Limitations
The Delphi group’s skill mix ensured a balance of clinical, behavioural and academic input. However, the group did not represent all healthcare practitioners, potentially limiting the resource’s usefulness for unrepresented groups such as social prescribers. In addition, consultation was only undertaken with two groups of medical specialists. Therefore, it is possible that the structure developed to suit autoimmune rheumatic disease and musculoskeletal pain does not best support conversations in other long-term conditions. As a UK-focused study, we reviewed clinical guidelines published in English, but this may reduce applicability to global healthcare environments. We do not know if searching published manuscripts and clinical guidelines in other languages would have generated additional insights or messages that would have impacted this work.
Survey fatigue is an inherent risk of Delphi studies and may explain participants’ observed dropout rate through the rounds.28 Removing 10 questions for the second round had a minimal impact on the average completion time, which changed from 32 min in round 1 to 28 min in round 2. This may reflect that users put aside 30 min to fill out the questionnaire or that the 10 respondents who completed round 2 were more committed to giving feedback on the project. Despite being lower than the average reported dropout rate in Delphi studies,28 the loss of five participants limited the range of opinions contributing to round 2. Dropout risks regression to the mean and may have contributed to the very high agreement levels seen in round 2.29
Future research should seek to test the resources developed during this study to determine efficacy, understand implementation strategies and help improve the format and function of resources to better support conversations on physical activity in the management of long-term conditions. In addition, future Delphi studies focusing on similarly complex topics may benefit from recruiting a larger panel.
Conclusion
This mixed-methods study represents a unique effort to understand and address the requirements of healthcare professionals and people living with health conditions to improve their conversations on physical activity. The preparatory phase identified limited time, a lack of knowledge around physical activity and low confidence in behaviour change skills as fundamental challenges for healthcare professionals. Addressing these requirements, the Delphi phase led to the development of a resource offering ‘1-minute’, ‘5-minute’ and ‘more minute’ person-centred and evidence-based conversation templates for healthcare professionals. The resource is now freely available online at www.movingmedicine.ac.uk.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The research proposal was submitted to the UK National Health Service (NHS) Research Authority and Medical Research Council decision-making tool, which confirmed that NHS Research Ethics Committee review was not required. All participants of the Delphi and workshop groups provided informed consent by agreeing to participate in the study following a detailed description of what participation entailed. No research team or Delphi members stood to gain financially or otherwise from decisions taken in the Delphi study and all feature as authors of this manuscript. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to our collaborating partners, Sport England and Public Health England, for their support of this work and all clinicians and patients who contributed to the workshops in the preparatory phase. We would like to thank David Nunan for his advice and support on how to address the aims of this study critically. The successful realisation of this project has been in large part due to the energy, skills and creativity of the design team One Ltd. We are hugely grateful for their tireless work and passionate commitment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drhamishreid
Collaborators We would like to thank the Moving Medicine development group who gave their time and expertise to this Delphi study: Andrew Murray, Beverley Hall, Clare Scott-Dempster, George Bownes, Jim Kerss, Jo Foster-Stead, Joanna Lambert, John Rogers, Joseph Lightfoot, Jumbo Jenner, Lisa Stephens, Mark Batt, Martyn Standage, Paul Kelly and Vicky Lawson.
Contributors HR and NJ conceptualised, planned and led the delivery of this study. HR, RS and JB led the workshops. HR and JC designed and delivered the Delphi study. All authors contributed to decision making between Delphi rounds and the write up of the manuscript, which HR, JC and RC led. HR accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding Sport England provided funding to support this work through money from the National Lottery as part of the Moving Health Professionals Programme. £823 was spent during the preparatory phase of this project, with costs allocated to participant travel, consumables and hire of facilities. Staff costs totalled £17 000, while £408 was spent on software.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.