Article Text

Abstract
Objectives The objective was to determine recent cross-sectional trends in health-related fitness (HRF) in secondary school students by studying the 13–14 years old age group repeatedly over 6 years, considering parallel national trends in physical education (PE).
Methods Height, weight, broad jump, grip strength, 20 m shuttle run and throwing and catching skills were measured by the same research team using standardised techniques from 2014 to 2019. Trends in these HRF measures were assessed by linear regression, adjusting for school, sex and height. Interactions with fitness and body mass index (BMI) were tested. The number of PE lessons reported in the UK Annual School Workforce Census between 2010 and 2019 for all state-funded secondary schools was analysed.
Results Grip strength (B=−0.60, 95% CI −0.78 to –0.41), broad jump (B=−1.16, 95% CI −1.99 to –0.34), 20 m shuttle run (B=−1.85, 95% CI −2.58 to –1.12) and throwing and catching skills (B=−0.12, 95% CI −0.15 to –0.08) declined significantly over the study period. There was a greater reduction in broad jump and grip strength in adolescents with low fitness and a greater reduction in fitness and motor competence in adolescents with normal BMI. These declines coincided with a 16% reduction nationally in secondary school PE between 2010 (333 800 hours) and 2019 (280 725 hours).
Conclusion Adolescent HRF has declined in recent years, in parallel with PE lessons. Declines were observed across all young people and particularly those of low fitness and normal BMI. To reach the majority of young people, policy makers could increase PE in schools to increase activity and prevent worsening fitness and health in future generations.
- adolescent
- aerobic fitness
- secondary school
- physical activity
- physical fitness
Data availability statement
No data are available. Due to ethical approval, which does not allow data sharing during or after the study, there are no data that can be shared.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Health-related fitness measures have been declining in primary schoolchildren.
What are the new findings
Adolescent health and fitness measures have decreased from 2014 to 2019.
Adolescents with low cardiorespiratory fitness (CRF) show a greater reduction in muscle strength and power compared with adolescents with high CRF.
Normal-weight adolescents show a greater reduction in CRF and motor competence compared with overweight/obese adolescents.
Introduction
Muscle strength and cardiorespiratory fitness (CRF) are related to cardiovascular disease.1 CRF and muscle strength can be modified through activities. Thus, the importance of achieving a physically active lifestyle that incorporates activity of a high enough intensity in adolescence to improve CRF and muscle strength is critical for healthy development and the prevention of disease in later life.2 The importance of other factors, including motor competence (MC) and fundamental sports skills during childhood and adolescence, is emergent as determinants that relate to both initial engagement and longer term participation in physical activity (PA) and sport.3 Indeed, the relationship between MC and PA has been described as reciprocal in nature whereby MC and the individual’s perception of skill affect their ability and confidence to participate in PA.4 5 This may affect CRF and muscle strength.5 6 MC, muscle strength and cardiovascular fitness7 may be vital for achieving better cardiovascular and metabolic health, and for reducing the risk of non-communicable diseases such as hypertension, diabetes and obesity in later life.8
School is a critical period whereby MC, sporting skills, strength, power and fitness are built in all young people.9 10 However more recently, as PA has been documented to decline with age,11 particularly when children transfer to secondary school,12 there is a need to systematically monitor muscle strength, CRF and MC in school-age students. To date, there is little information on these measures in secondary schoolchildren and a need to assess these alongside health markers in all school-age children.13
Most young people attend school by statute and limited evidence indicates that the majority of school-age students accumulate most activity within school physical education (PE), which also provides an opportunity for regular measurements of fitness and health.14 15 Therefore, schools are an important site both for achieving and monitoring, health and fitness profiles, given evidence of recent increases in adolescent obesity,16 associated childhood diseases of inactivity17–19 and the importance of PE to the activity profiles of most students. We set out to determine recent cross-sectional trends in fitness and health indicators for secondary school students and whether parallel national trends in PE lesson time could offer a possible explanation.
Materials and methods
Data on height, weight, broad jump, grip strength, 20 m shuttle run and throwing and catching skills were collected by the same research team using standardised techniques in adolescents aged 13–14 years (UK Year 9) over 6 years from 2014 to 2019. A representative sample of three schools from the Oxfordshire region were contacted, covering a broad socioeconomic demographic, and were enrolled in the study, with formal consent from the head teacher. Measurements were carried out as part of enhanced PE lessons at the schools. These lessons formed part of the screening process to recruit participants into three clinical studies (Exploring the Impact and Feasibility of a Pathway to Sport and Long-term Participation in Young People (EPIC; NCT02517333), The Rhythmic Motor Learning in Children with Developmental Coordination Disorders (EPIC2; NCT03150784) and the Oxfordshire Sedentariness, Obesity and Cardiometabolic Risk in Adolescents—A Trial of Exercise in Schools (OxSOCRATES; NCT04118543)). These studies involved public input at the design, conduct and dissemination stages.
Setting
Each school sent a comprehensive information sheet, prepared by the research team and reviewed by the relevant ethics board, to all parents. The schools were custodians of the data and the parents or guardians were asked by their school to complete a form if they objected to their child’s anonymised data being analysed by the research team (opt-out informed consent). The average opt-out across all three schools was <5%.
Participants
All students were enrolled in Year 9 at the start of the academic year of 2014 or each subsequent year until 2019. Exclusion criteria consisted of any known medical conditions that could explain deficits in movement or the inability to participate in general PA. These included pathology in cognitive, neurological, musculoskeletal, behavioural or visual function. This was screened using a Physical Activity Readiness Questionnaire.20
Procedure
Data collection took place in each school’s sports hall during timetabled PE lessons. Each exercise measure was set up at individual stations and the students rotated between them in groups of 4–5. Each station was controlled by an experienced researcher from Oxford Brookes University, with each session supervised by two PE teachers from the school. Not all measurements were carried out at each time point. Data were not collected for the 20 m shuttle run, the ball catching task and grip strength in 2014. Furthermore, there were no broad jump data in 2018.
Measures
Height and weight were measured with a portable Harpenden Stadiometer (Holtain, Crymych, UK) and a SECA medical 770 digital floor scale (SECA, Hamburg, Germany), respectively. Participants were dressed in light sports clothing and were instructed to remove their shoes. Height and weight were used to calculate body mass index (BMI), which is presented as age and sex-independent z-scores (WHO).21 A battery of health-related fitness (HRF) measures was then assessed, including grip strength, broad jump, CRF and MC.
Grip strength was used as a proxy of total muscle strength as they are strongly correlated in adolescents.22 The Takei TKK 5001 hand-held dynamometer (P&A Medical, Chorley, UK) was used to evaluate the highest grip strength from a maximum of three attempts. Each participant was instructed to squeeze the dynamometer as hard as possible, while they were in a standing position with their elbow fully extended and their arm resting comfortably by their side.
Power was measured using the broad jump, as it has been strongly correlated with a one-repetition maximal leg extension test.23 Participants were instructed to stand with both feet behind a marked line and jump as far as possible, landing with their feet together. The longest jump out of two attempts was recorded.
CRF was measured using the 20 m shuttle run test.24 25 Participants were instructed to run back and forth between two markers that were 20 m apart. The time required to run between each marker became shorter as the test progressed, requiring participants to run faster. The participants were verbally encouraged to produce a maximal effort and were withdrawn from the test when they failed to reach the marker within the allotted time on three consecutive occasions, or they withdrew from the test themselves. The total number of shuttles that they achieved was recorded as their score.
Over the study period, two very similar throwing and catching tasks were used to assess upper limb MC. The first was the alternate hand ball toss.26 In this, each participant threw a tennis ball in an underarm action against a wall and attempted to catch it with the opposite hand. The number of successful catches in 30 s was recorded. The second was the ‘catching with one hand’ measure from the Movement Assessment Battery for Children-2 age band 3 (11–16 years).27 28 In this, each participant threw a tennis ball with one hand at a wall and attempted to catch it with the same hand. The number of successful catches, out of 10 attempts for each hand, was recorded. Although these two assessments differ slightly in their difficulty, they are highly correlated. Therefore, their rank order would be expected to be similar or the same in most populations. On this basis, we converted each measure to their z-scores (SD score) so that rank order could be compared between these groups.
The total number of hours dedicated to teaching PE was collected from the UK Annual School Workforce Census.29 In this census, all state (UK)-funded secondary schools reported the total hours of PE lessons taught each year to students from year 7 to year 13 (11–17 years old).
Statistical analysis
Statistical analysis was performed using STATA (V.16.1, StataCorp, College Station, Texas). All data were found to be normally distributed on visual inspection of histogram plots. Little’s missing completely at random (MCAR) test was used to assess the missingness of the data.30 Independent t-tests were used to assess the difference in HRF measures between sexes. Linear regressions were performed to assess the temporal trends of each HRF measure. These relationships were also assessed for interactions with fitness and BMI z-score over time. Each model was adjusted for school31 and sex because school catchment areas differed by Index of Multiple Deprivation (IMD).32 Grip strength, broad jump and ball catching were all additionally adjusted for height to account for inherent advantages of greater physical size in these measures. CRF was split into low (30 shuttles), medium (50 shuttles) and high (70 shuttles) tertiles, and BMI categories were determined by WHO thresholds (<1 z-score=normal weight, ≥1 to 2 z-scores=overweight and >2 z-scores=obese). Statistical significance was defined as p<0.05.
Patient and public involvement
Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
A total of 2651 participants took part in school screening assessments between September 2014 and December 2019. A summary of HRF measures is given in table 1, showing the expected sex differences in height, strength, fitness and upper limb MC. There was a statistically significant difference in BMI z-scores between sexes, but the magnitude of this was clinically unimportant. All participants had data on sex and 94% had complete data on height and weight. In 2014, only broad jump was assessed and was recorded for 84% of participants. In 2018, all HRF measures except broad jump were assessed and were available for 62% of participants that year. In other years, 80.4% of participants had complete HRF data sets. Some missing data were due to lesson time limitations. For all years except 2014 and 2018, we tested for data MCAR and showed that the missingness of data on sex (p=0.16), BMI (p=0.50) and fitness (p=0.17) was random.
Summary characteristics
Across the three schools, IMD ranged from the 1st to the 4th quintile and regression analyses were adjusted accordingly. Analyses were also adjusted for sex, given significant sex differences in HRF measures (table 1). Grip strength, broad jump and ball catching were additionally adjusted for height.
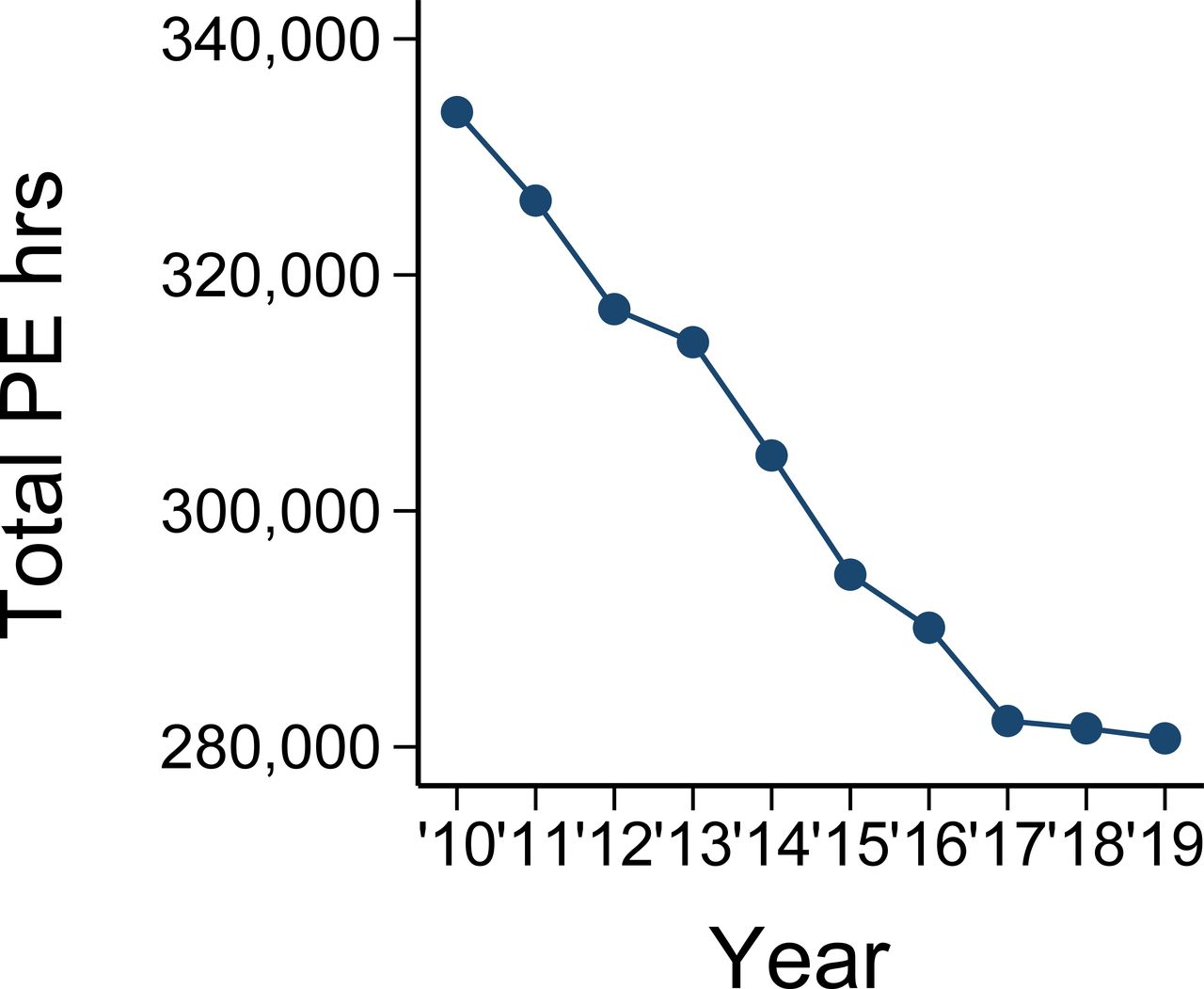
Figure 1 shows the total amount of time dedicated to PE lessons across all state-funded secondary schools in the UK from 2010 to 2019. In total, PE hours decreased by 53 075 (16%) from 333 800 in 2010 to 280 725 in 2019. We chose to report a wider temporal window than is encompassed by our HRF assessments, to better illustrate the overall trend and because declines in taught PE in earlier years may have impacted on our students before they reached Year 9.

The total hours of taught physical education (PE) lessons for secondary school (11–17 years old) students from 2010 to 2019.
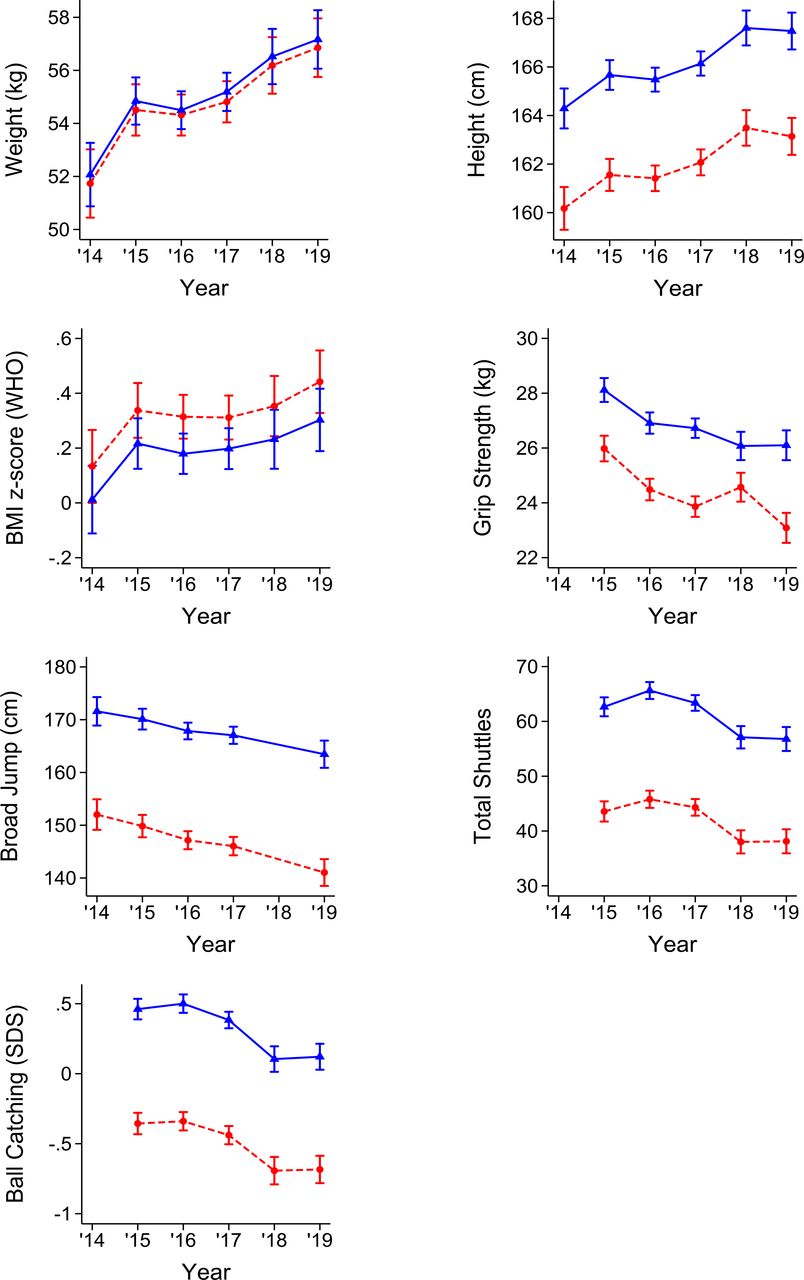
Table 2 reports the linear trends of each HRF measure over time. Height and weight have increased significantly since 2014. There was no significant trend in BMI z-scores over the same period. Grip strength, broad jump and total shuttles reduced significantly with time. Thus, strength, power and CRF levels have all decreased in adolescents aged 13–14 years since 2014–2015 with a parallel increase in body weight and height but not in adiposity. Furthermore, upper limb MC has significantly decreased since 2015. To illustrate these trends, the marginal means of each HRF measure are plotted by sex in figure 2.
Trend analysis of linear regressions of health and fitness measures over time for adolescents aged 13–14 years

Estimated marginal means and 95% CIs of health-related fitness measures from 2014 to 2019. The solid blue lines and triangles represent boys and the red dashed lines and circles represent girls. BMI, body mass index; SDS, SD score.
The interactions between CRF and the trends of HRF measures are illustrated for three tertiles of CRF in figure 3. There were significant interactions for broad jump and grip strength, with the steeper declines in these measures for the low CRF segment of the population compared with those with higher CRF. Figure 4 shows the interactions between BMI and year for each HRF measure. There were significant interactions for CRF and MC, with steeper declines in these measures in the normal-weight segment of the population and no real change in those who were overweight or obese.
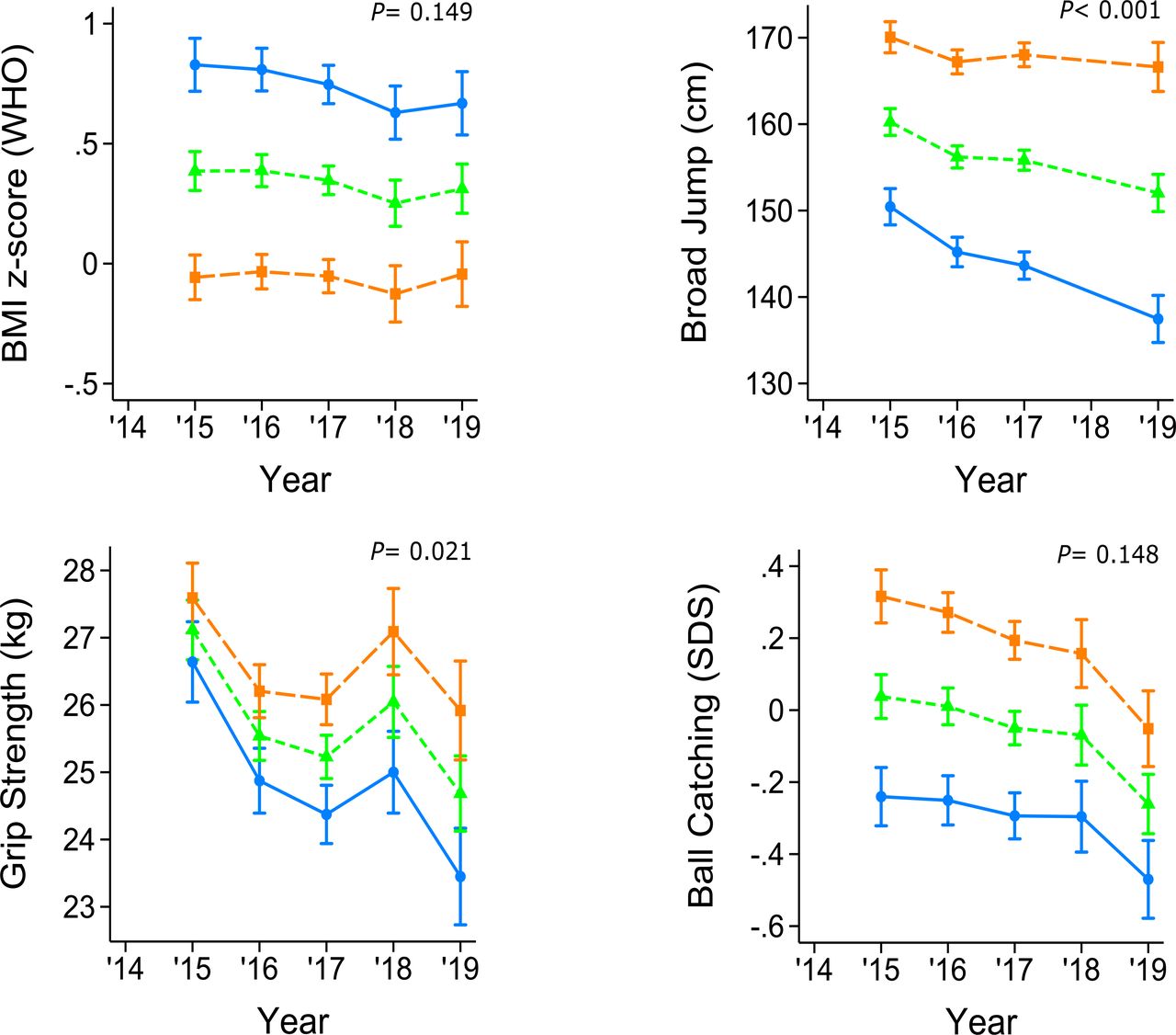
Estimated marginal means and 95% CIs illustrating the interactions between fitness and year for three fitness tertiles: low fitness (blue circles with solid line), moderate fitness (green triangles with short dashes) and high fitness (orange squares with long dashes). BMI, body mass index; SDS, SD score.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimated marginal means and 95% CIs illustrating the interactions for body mass index (BMI) and year for three BMI categories: obese (orange squares with long dashes), overweight (green triangles with short dashes) and normal weight (blue circles with solid line). SDS, SD score.
Discussion
Over 6 years, from 2014 to 2019, we observed a declining trend in CRF, MC, muscle strength and power, alongside positive trends for weight and height, but not BMI, in UK adolescents. These changes in HRF measures coincided with a reduction in PA through taught PE hours across UK secondary schools. Our findings are the first demonstration in adolescents that the declines in HRF measures that are similar to those that have been reported in younger children are also occurring in UK secondary schools and may in part be related to declining PE.13 33 34 We demonstrate declines in MC, which have not been reported before, and which are likely to impact on future exercise habits and cardiorespiratory health in these year groups. Notably, we found that over this period, fitness and MC have been declining more in normal-weight young people than their overweight peers. This may be particularly important as their normal weight could mean that their declining health status is less likely to be detected. We also found that strength and power are declining more steeply in people with low CRF compared with those with higher CRF. One possible reason for this is that such individuals may not participate in sport or fitness-related activities outside of school and thus be entirely reliant on the structured exercise training that PE delivers. Considering that adolescent measures of cardiorespiratory and muscle fitness are strongly related to morbidity in adulthood,35 36 and are better predictors than similar measures made earlier in life,37 our research reveals a worrying trend in HRF that may cause burgeoning health problems in future adult populations.
Low-grip strength and power in children and adolescents are four times more likely to persist into adulthood compared with high strength and power.37 Previous evidence indicated that a reduction of 1 SD in childhood grip strength is associated with 34% greater incidence of pre-diabetes or type 2 diabetes in adulthood.38 Based on this, our finding of a 0.2 SD reduction in adolescent grip strength over the last 5 years might be expected to result in a 7% increase in pre-diabetes or type 2 diabetes in future adult populations. Given that the annual UK economic burden of these disorders was estimated at £11.7 billion in 2012 and is likely to have risen since,39 this decline in adolescent HRF would correspond to at least £820 million greater costs per year in future populations if it is representative of a UK-wide change. This highlights an urgent need for regulated HRF monitoring in schools and political/educational interventions designed to reverse the trends illustrated here.
Acquiring muscle power in adolescence has also been shown to reduce the risk of adult metabolic syndrome.36 Evidence from Fraser et al36 suggests adolescents with high muscle power have a lower relative risk (0.26) of acquiring metabolic syndrome in adulthood, compared with adolescents with low muscle power. Our current study reports a 0.3 SD decline in adolescent muscle power over the past 6 years and this, in combination with low muscle strength, may have an additive effect on future morbidity. Our current findings clearly highlight a need to assess children and adolescent muscle strength and power and to consistently monitor them over time.13
A number of different factors such as PA enjoyment, self-perceived MC and extracurricular factors such as access to supervised PA and exercise equipment may explain these reductions in fitness, MC and muscle strength and power.40 41 A number of studies have reported that very few children and adolescents are meeting the recommended guidelines for daily PA.42 Part of this inability to meet the guidelines may be as a result of reduced opportunities for young people to be physically active. We propose that one environment where all children and adolescents spend the majority of their time and have access to regular PA is school. Data suggest that school is where the majority of PA is performed by children and adolescents and that this is largely in PE lessons.15 These PE lessons provide young people with the opportunity for regular PA and provide greater exposure to vigorous forms of PA, which yield better health outcomes compared with moderate forms of PA.14 Structured PE lessons may also train students better in MC and coordination skills that are important for engendering a desire to exercise outside of PE and thus have extended benefits. Our study is the first to report that the number of taught PE lessons has declined continuously and steeply over the past decade. Although our study was not designed to test the impact of PE lessons on HRF directly, it seems empirically unlikely that there would be no detrimental effects of declining exposure to PE, given the well-known benefits of exercise. These reductions in HRF measures may have been further exacerbated by a change in the type of PE lessons provided.43 Evidence from the Fit to Study project indicated that very few students are performing any significant degree of PA within the PE lesson and the majority of lessons taught are ones in which the lowest levels of PA and exercise intensity are recorded.43 This should lead to further research exploring, which PE lessons produce the highest amount of PA while allowing the students to learn the required fundamental movement skills.
Strengths and limitations
Our study has some notable strengths and limitations. The sample size was large and addressed whole-year groups at the same age over up to 6 years in schools that together represent a broad socioeconomic section of society. However, the samples were all drawn from a single county and may, therefore, not be representative of changes throughout the UK. The serial cross-sectional design does not address changes within the same cohort of students. This limited our ability to address whether some changes preceded others and might, therefore, be causal. However, this was not the intention of this study, which was designed to address serial cross-sectional trends in a public health context. The study also did not address exposure to PE or PA levels in or out of school in the individuals studied and cannot therefore directly address the possibility that declining CRF was caused by other declines in PAs. Nevertheless, we propose there is strong evidence that PE may be important for overall PA in this age group14 15 and flag the national evidence of declining exposure to PE.29
Conclusion
This study is the first to report declining CRF, MC, muscle strength and power in recent years in a relatively large and diverse sample of UK adolescents. This has coincided with a drastic reduction in the number of taught PE lessons over the last decade. We also add evidence that muscle strength and power are declining quickest in adolescents with low fitness while CRF and MC are declining most in normal-weight adolescents. We suggest that a programme of monitoring should be a priority in all school-age children and adolescents and interventions could be swiftly established in schools, which focus on increasing PE lessons frequency and duration to reverse these adverse trends, thereby preventing expected, costly and serious adverse consequences for future population health.
Supplemental material
Data availability statement
No data are available. Due to ethical approval, which does not allow data sharing during or after the study, there are no data that can be shared.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Oxford Brookes University Research Ethics Committee (UREC 140844 in 2014; 161033 in 2016) or the University of Oxford Medical Sciences Interdivisional Research Ethics Committee (MS IDREC R54302/RE001 in 2018), and the University of Oxford Central University Research Ethics Committee (CUREC R54302/RE005). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all three Oxfordshire schools that took part in this study and each of their Heads of Department for Physical Education. Their hard work on top of a very demanding schedule was greatly appreciated. In addition, we would like to thank all the students and staff within the Centre for Movement, Occupational and Rehabilitation Sciences (MOReS) at Oxford Brookes University for assisting with the data collection. Professor Helen Dawes is supported by the Elizabeth Carson Trust and the NIHR Oxford Biomedical Research Centre.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HD was the author acting as guarantor.
Funding Action Medical Research for Children (GN2445); Chartered Society of Physiotherapy Charitable Trust (GN2445); British Heart Foundation (FS/18/22/33479); Community Sport Activation Fund; PF Charitable Trust.
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.