Article Text

Abstract
Objectives. Many patients with COVID-19 suffer from persistent symptoms, many of which may potentially be reversed by high-intensity interval training (HIIT). Yet, the safety and tolerability of HIIT after COVID-19 is controversial. This study aimed to investigate the fidelity, tolerability and safety of three different HIIT protocols in individuals that had recently been hospitalised due to COVID-19.
Methods. The study was a randomised cross-over trial. We compared three supervised HIIT protocols (4×4, 6×1, 10-20-30) in 10 individuals recently discharged after hospitalisation for severe COVID-19. Each HIIT protocol had a duration of 38 min and was performed with a 1-week washout between them. Outcomes included adverse events, exercise training intensity and tolerability assessed by the Likert scale (1–10).
Results. All 10 participants aged 61 (mean, SD 8) years (5 males) completed all three HIIT protocols with no adverse events. High intensities were achieved in all three protocols, although they differed in terms of time spent with a heart rate ≥85% of maximum (mean (SD); 4×4: 13.7 (6.4) min; 10-20-30: 12.1 (3.8) min; 6×1: 6.1 (5.6) min; p=0.03). The three protocols were all well tolerated with similar Likert scale scores (mean (SD); 4×4: 8 (2), 10-20-30: 8 (2), 6×1: 9 (2), p=0.72).
Conclusion. Our findings indicate that recently hospitalised individuals for severe COVID-19 may safely tolerate acute bouts of supervised HIIT as per protocol. This warrants future studies testing the potential of regular HIIT as a rehabilitation strategy in this context.
- physical activity
- rehabilitation
- feasibility
Data availability statement
Data are available on reasonable request. The original data that support the findings of this contribution can be obtained from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Many patients suffering from COVID-19 develop so-called ‘long COVID-19’ which may be prevented or alleviated by targeted rehabilitation.
High-intensity interval training (HIIT) is known to be a time-efficient rehabilitation intervention in several patient populations, notably in those with heart and lung disease.
What are the new findings
Recently hospitalised patients who were mildly to slightly affected by long COVID-19 can satisfactorily complete acute exercise by the three most widely used HIIT protocols, so-called 4×4, 6×1 and 10-20-30 HIIT.
Patients find HIIT both enjoyable and tolerable and we observed no adverse events.
In patients recently hospitalised with COVID-19, the fidelity, tolerability and safety are comparable between the three HIIT protocols.
Introduction
It has become increasingly clear that a substantial proportion of patients suffering from COVID-19 develop so-called ‘long COVID-19’, that is, often invalidating symptoms including dyspnoea, chest pain, exercise intolerance and extreme fatigue, to mention a few, all of which persist way beyond the acute viral infection.1–4 The underlying mechanisms of long COVID-19 are unknown but likely involve residual inflammation in the heart, lungs and vasculature.5 While the need for implementing evidence-based rehabilitation schemes that include exercise training following COVID-19 is imminent, no consensus exists as to how such programmes should be designed.
It is widely appreciated that high-intensity interval training (HIIT) promotes greater health-related benefits than traditional moderate-intensity training in various patient populations despite a reduced time commitment.6–8 However, in the context of COVID-19 rehabilitation and long COVID-19 prevention, it has emerged as a particularly controversial training modality. Hence, several opinion papers and guidelines favour low-intensity exercise with gradual increases in intensity, mostly due to safety concerns.6 9–15 There is nonetheless currently no firm evidence base to argue in favour of this. A recent retrospective study on 28 discharged COVID-19 survivors conversely concluded that HIIT might safely be performed in these patients.16 Furthermore, in contrast to low-intensity and classical endurance exercise training, HIIT may more specifically target residual vascular inflammation, a putative central mechanism of long COVID-19.5 However, it is unknown to which extent it is feasible to implement HIIT in recently discharged patients with COVID-19, that is, whether they can tolerate HIIT without adverse effects.
In the present study, we assessed the fidelity, tolerability and safety of three widely used HIIT schemes in individuals recently discharged after hospitalisation for severe COVID-19.
Methods
Study design, participants and randomisation
The study was performed from September to December 2020 at the Centre for Physical Activity Research at Rigshospitalet in Copenhagen, Denmark.
Ten recentlyk hospitalised individuals who had recovered from the acute phase of severe COVID-19 infection were included. Severe acute respiratory distress syndrome coronavirus 2 was confirmed by a PCR from a pharyngeal swap in all cases, and the COVID-19 was considered as severe when it had required hospitalisation with oxygen supplementation. Recovery from COVID-19 was defined as the time of hospital discharge. In terms of eligibility, the inclusion criteria were hospitalisation-requiring COVID-19, age ≥40 years and ≤10 L oxygen requirement during hospitalisation. Exclusion criteria were atrial fibrillation/flutter, acute myocarditis, health conditions that prevent from participating in the exercise training intervention, and treatment with interleukin-6 receptor antagonists.
Participants underwent baseline testing, including a medical health interview and examination, arterial office blood pressure measurement, 12-lead ECG, a whole-body dual-energy X-ray absorptiometry, pulmonary function testing (dynamic spirometry, whole-body plethysmography and single-breath diffusing capacity to carbon monoxide). A maximal oxygen consumption (V̇O2max) test was performed on a bicycle ergometer with a 5 min warm-up, immediately followed by a 15 Watt increase every minute until exhaustion. Participants completed a Post-COVID-19 Functional Status Scale (PFASS) questionnaire,17 which yields a score from 0 to 4, where 0 indicates no functional limitations, 1 negligible functional limitations, 2 slight functional limitations, 3 moderate functional limitations and 4 severe functional limitations.
The participants were allocated to the random sequence by which order they would complete and evaluate the three HIIT protocols in a cross-over design as described below. Randomisation was performed by a researcher with no other role in the study who generated a block randomisation schedule with balanced permutations stratified by sex. The block sizes were not disclosed to ensure concealment, and participants were blinded for the sequence allocation until just before initiating the given HIIT session. To maintain blinding, the randomised sequence was delivered by email to a study investigator. The study investigator informed the participant before each training session which HIIT protocol to perform.
No changes in the trial design were made after the start of the experiments. It was not appropriate or possible to involve patients or the public in designing, conducting, reporting or disseminating our research. The original data that support the findings of this contribution can be obtained from the corresponding author on reasonable request.
Exercise training interventions
The three different HIIT protocols, including the specific training designs, are detailed in table 1. The duration of the three HIIT protocols was matched in exercise duration (38 min). A 10 min warm-up was followed by a block of interval exercises, with a duration between 21 and 25 min depending on the specific protocol, aiming at reaching a specific percentage of maximal heart rate (HRmax) for 4×4, maximal workload (Wattmax) for 6×1 or subjective effort for 10-20-30 (further details in table 1). This was followed by a variable cool-down period (3–7 min) depending on the protocol. All exercise sessions were supervised by educated personnel.
Structure of the three different high-intensity interval training protocols
Fidelity and tolerability
Fidelity was assessed by participant adherence to the prescribed training (dose reduction or dose modification) and the achieved intensity (table 1). The latter was evaluated by rate of perceived exertion (RPE) after each interval (6–20 Borg scale)18 and after completed training (1–10 Borg scale),19 as well as from minutes above 85% of HRmax. Furthermore, enjoyment and perceived tolerance were evaluated by the 10-point Likert scale.20
The primary qualitative evaluation of the HIIT protocols was an a priori defined composite endpoint based on three parameters: (1) participant adherence (fidelity), (2) a 10-point Likert scale (tolerability) and (3) adverse events (safety). This was displayed by a red-amber-green system inspired by a previous publication21 (table 2). The lowest of the three parameters determined the overall red-amber-green rank of the given HIIT protocol in the individual participant. No changes in outcomes were made after the start of the experiments.
Red-amber-green system designed to evaluate the three high-intensity interval training protocols
Safety
At the baseline visit, all participants underwent a medical health interview and examination to assess health status. The following contraindications and precautions were considered: acute or recurring chest pain or systolic blood pressure >200 mm Hg±diastolic blood pressure >100 mm Hg. Safety during exercise training was assessed as the following, which also served as termination criteria: onset of angina, signs of poor perfusion (confusion, nausea, lightheadedness, central cyanosis), requests to terminate (eg, due to intolerable dyspnoea), and physical or verbal manifestations of severe fatigue. A 12-lead ECG was obtained after each HIIT session to assess whether there was evidence of arrhythmia or myocardial ischaemia.
Statistics
The HIIT protocols were compared using analysis of covariance (ANCOVA) modelling for training intensity (minutes above 85% of HRmax), the Likert scale, RPE and PFASS. Unless otherwise stated, data are reported as mean (SD) or median (IQR). The sample size was determined on what was feasible within the local context under considerations of reducing the number of participants to exposure of potential harms. All analyses were performed using GraphPad Prism, V.7.02 (GraphPad Software) or STATA/SE (StataCorp) V.16.1, and a two-tailed p<0.05 was considered statistically significant.
Results
The study flow diagram is shown in figure 1. A total of 10 participants were enrolled and randomised and complied with the three HIIT protocols, and all participants were thus included in the analysis (attendance 100%). Baseline characteristics, including lung function and PFASS scores, are presented in table 3. All participants except for one with a restrictive pattern had normal ventilatory capacity, while five had reduced diffusing capacity (mild reduction in three cases, moderate-to-severe in two cases). Generally, the participants were only mildly to slightly affected by persisting COVID-19 symptoms according to PFASS scores, with the highest score of 3 in one individual. The primary reason for not participating was feeling too weak to exercise after the infection.
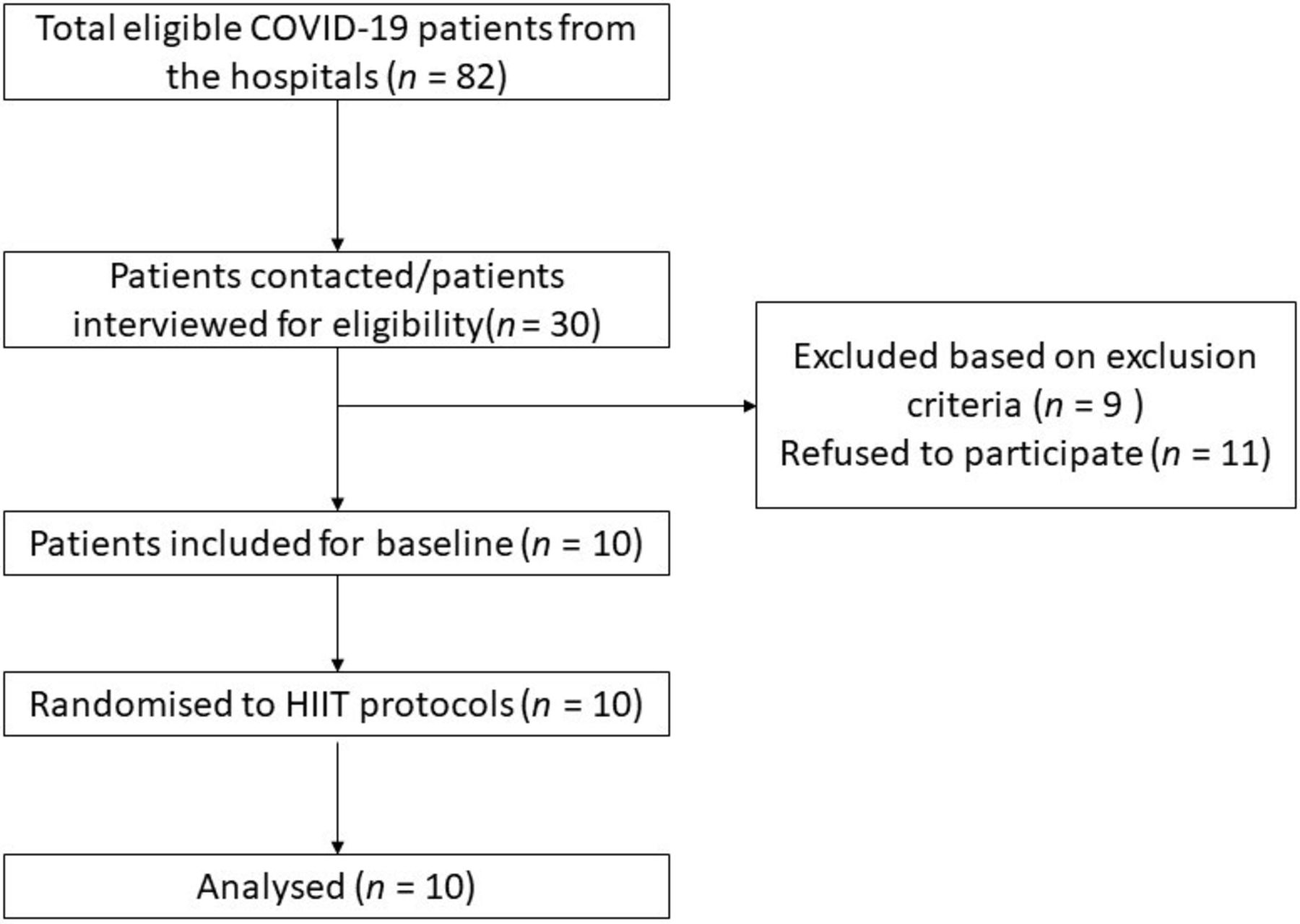
Study flow chart. Flow chart of participants included in the study.
Baseline characteristics
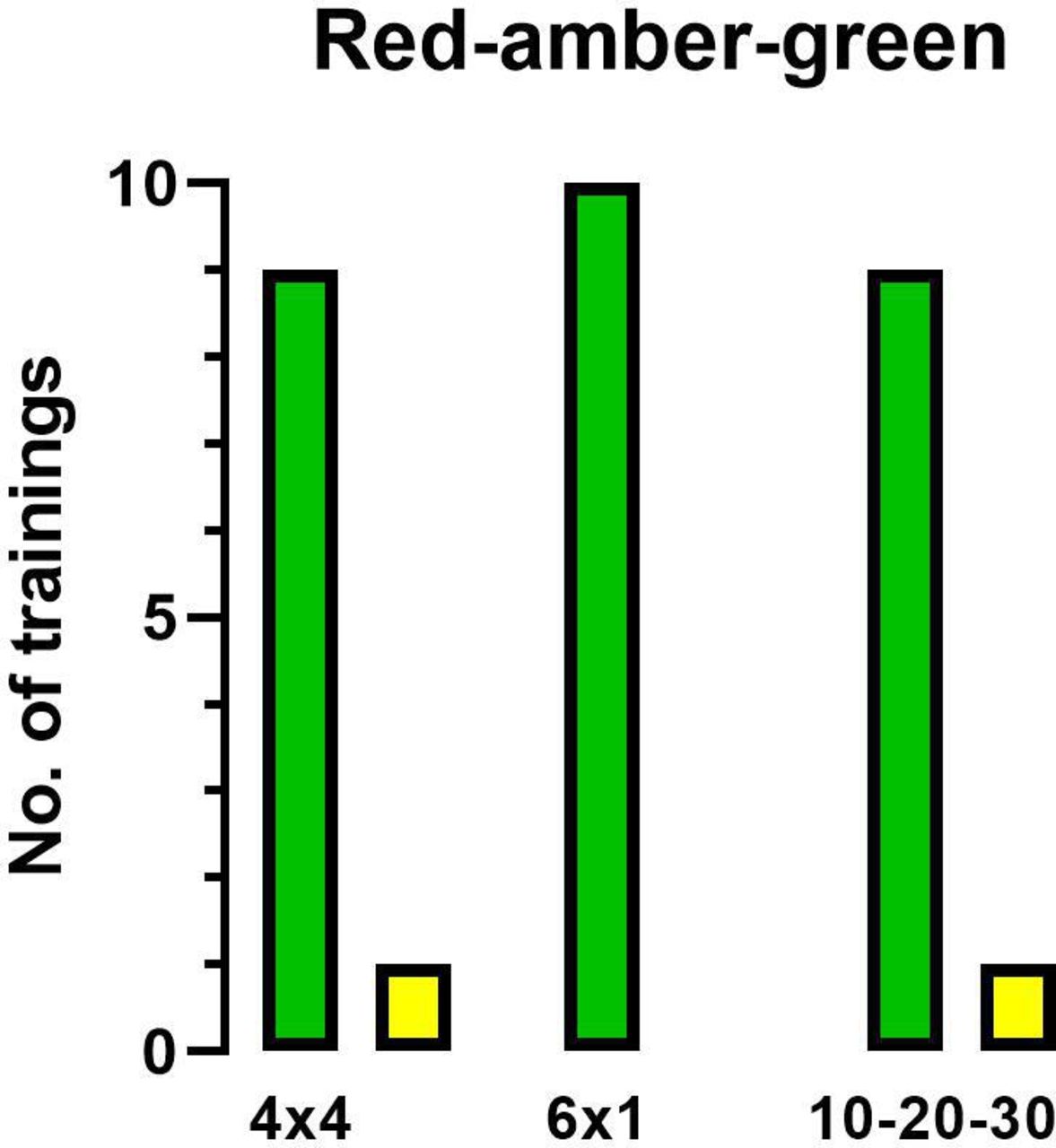
Outcomes of the three HIIT training protocols were compared by a red-amber-green design (table 2). No ‘red’ training sessions occurred, and only 1/10 training session in 4×4 was amber due to a low Likert score (tolerable: 3/10), and 1/10 in the 10-20-30 was amber due to inadequate time spent >85% of HRmax as prescribed. The rest of the training sessions were reported as green, which means all three HIIT protocols are tolerable and safe (figure 2). No adverse events were reported during the study, and no angina or ECG changes were seen after HIIT training.
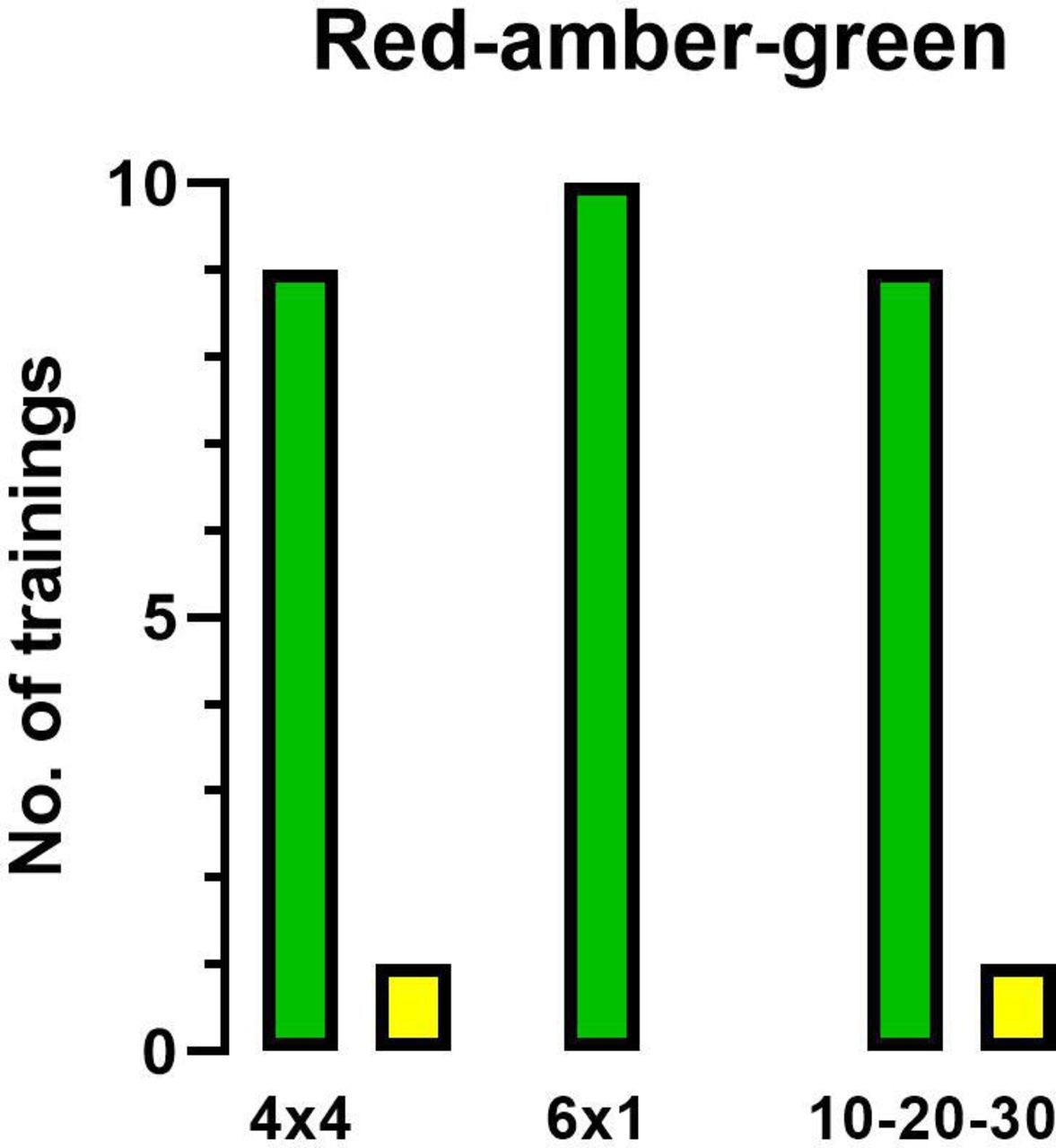
Red-amber-green. Number of ‘red’, ‘amber’ and ‘green’ training sessions of the three high-intensity interval training protocols.
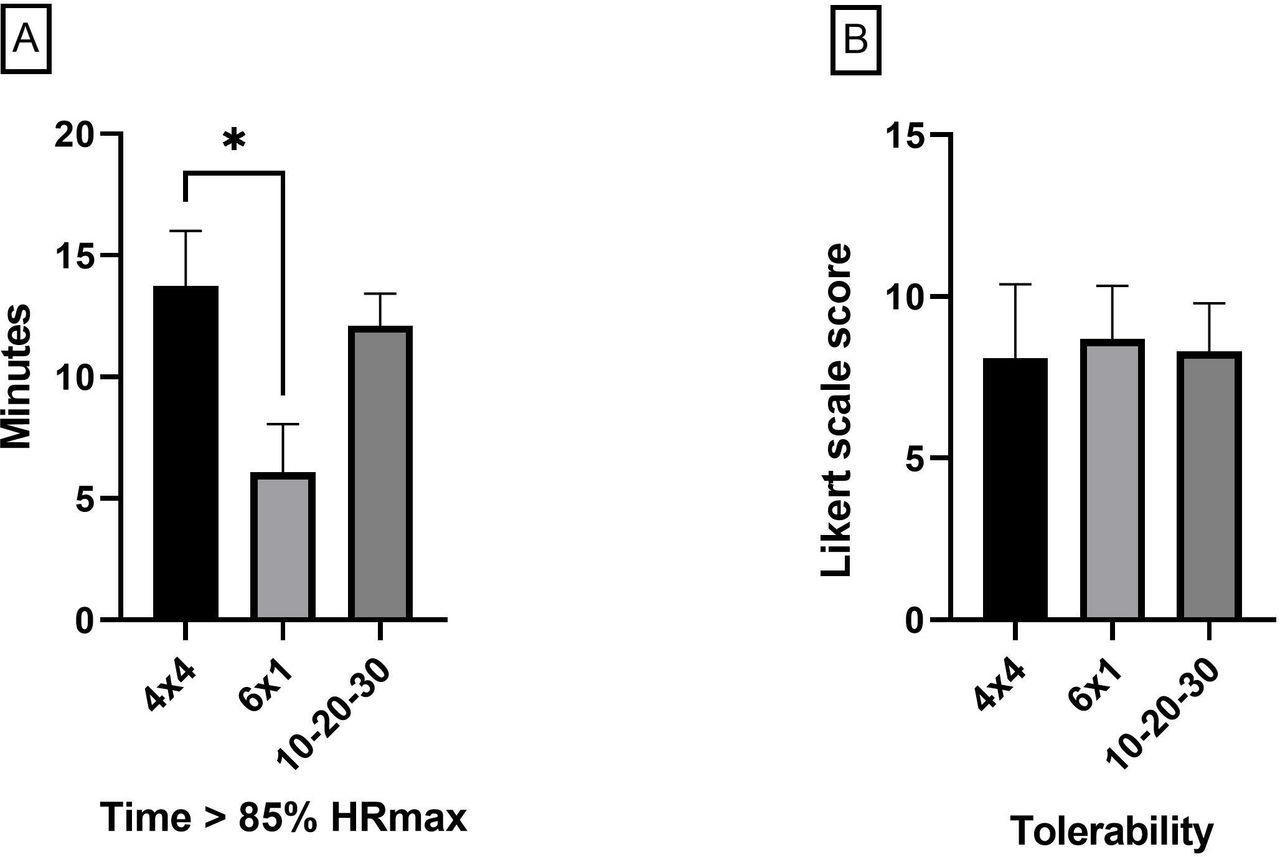
There was a between-protocol difference in terms of the exercise intensity when dichotomously assessing for time spent with a heart rate ≥85% of HRmax (figure 3A). In contrast, tolerability as assessed by Likert scale scores (figure 3B) and RPE (4×4; 5 (2), 6×1; 5 (2), 10-20-30; 6 (2); p=0.28) did not differ between protocols. When considering HR and RPE changes non-dichotomously, largely similar objective and subjective measures of intensities were observed throughout each protocol (online supplemental figures 1 and 2).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Intensity and tolerability. (A) Intensity: time spent with a heart rate >85% of maximum for each protocol. (B) Tolerability rated by the Likert scale. Data are presented as mean (95% CI); *p=0.028. HRmax, maximal heart rate.
Discussion
This study compared the fidelity, tolerability and safety of three HIIT protocols conducted on individuals recently hospitalised with COVID-19. Our findings indicate that HIIT is feasible regarding fidelity, tolerability and safety, regardless of the specific protocol.
No adverse events occurred in any of the HIIT protocols. These results are in line with a previous study on COVID-19 survivors,16 as well as several studies on other ‘high risk’ patient groups such as ischaemic heart disease and heart failure in whom it is considered safe.6 22 Thus, we consider it unlikely that HIIT should be associated with a high risk of acute adverse cardiovascular events. This concern was raised in The Stanford Consensus Statement for Post-COVID-19 Rehabilitation as one of the primary arguments against HIIT use in these individuals.23 However, studies with regular exercise are needed to determine the long-term safety of HIIT in this context.
We found that while all three HIIT protocols were well tolerated, the greatest intensity, given by the time spent above 85% of HRmax, was achieved by 4×4. Time spent above 85% of HRmax was chosen since HIIT is widely defined as training intensities at 85%–90% of HRmax.7 24 The cut-off, 85% of HRmax, is arbitrarily defined, and the supplemental graphic overview shows that all protocols performed well with high RPE and HR reaching maximum in all protocols. These findings, combined with the strong physiological rationale for HIIT, highlight it as an attractive option for COVID-19 rehabilitation. This is further invigorated when considering the widespread and disease-specific vascular inflammation in COVID-19 that persists after the acute viral infection and which is thought to contribute to the very diverse cluster of symptoms associated with long COVID-19.25 Potentially, this may be specifically counteracted with HIIT, where the pronounced changes in vascular shear stress that occur between intervals combined with the effects of anti-inflammatory myokines that are released from working skeletal muscle in an intensity-dependent manner may enhance endothelial repair and dampen proinflammatory processes within the vascular wall.5
The high composite intensity achieved is the best-documented means for increasing maximal oxygen consumption (V̇O2max) and exerting beneficial cardiovascular effects. HIIT has thus been reported to be superior to continuous endurance training in several patient groups.7 26 These include patients with hypertension, ischaemic heart disease and heart failure, in which V̇O2max has furthermore been noted as the single best predictor of mortality.27 28 It remains to be determined whether this is also the case in various lung diseases, such as chronic obstructive pulmonary disease. Still, HIIT has been noted to be associated with higher adherence in these patients, conceivably because the intermittent nature of HIIT reduces ventilatory demand and thus exertional dyspnoea and perceived breathing effort.29 30 This may also apply to patients recovering from COVID-19. Even though the present study is small scale in this context, and larger randomised controlled studies are warranted, we posit that HIIT should also be considered among the preferred training modalities in the rehabilitation post-COVID-19.
A strength of the study is the randomised sequence of the exercise training protocols, which eliminated systematic carry-over effects of the previous training protocol. Another strength is that this is the first study testing HIIT protocols post-COVID-19 in a supervised manner. Moreover, our research investigated the fidelity, tolerable and safety of three various HIIT protocols with different work or intensity periods, thus enabling between-protocol comparisons.
Some limitations should be considered when interpreting the results of this study. First, our results may be affected by selection bias because the main reason for declining participation was feeling too weak to exercise, which may indeed be a symptom of long COVID-19. Our results regarding fidelity and tolerability may thus have been different if we had studied these patients, which arguably represent the group that may benefit the most from targeted rehabilitation. Another important limitation is the small study size (n=10) which limits the conclusions, particularly when considering the heterogeneity of the participants. Furthermore, we only tested the fidelity, tolerability and safety to acute HIIT and cannot draw any firm conclusions regarding training over extended periods. Even though we expect a HIIT-based rehabilitation scheme over an extended period to be feasible, this remains speculative.
In conclusion, we found that individuals recently recovered from COVID-19 could successfully and safely complete three acute bouts of the most widely used HIIT protocols. Our findings highlight that HIIT should be evaluated as a rehabilitation strategy for post-COVID-19 in future randomised controlled trials.
Data availability statement
Data are available on reasonable request. The original data that support the findings of this contribution can be obtained from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted per the Declaration of Helsinki with oral and written informed consent from all participants before inclusion and approved by the Scientific Ethical Committee of the Capital Region of Denmark (H-20033733 including amendment 75068 and 75799) and the Danish Data Protection Agency (P-2020-781) and pre-registered at ClinicalTrials.gov (NCT04549337).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @cresp_research @ronan_berg @cfas_dk
FF and IER contributed equally.
Contributors Conceptualisation: RHC, RMGB, MR-L. Methodology: RHC, RMGB, VR, MR-L, RKM, BLM. Formal analysis: FF, IER, RHC, RMGB, MR-L. Investigation, FF, IER, JBB, RSR, ML, SJ, RHC, RMGB, BLM, RKM. Supervision: RMGB, RHC. Resources: RMGB, RHC. Writing—original draft: FF, IER. Writing—review and editing: All authors contributed. Visualisation: FF, IER, MR-L.
Funding The Centre for Physical Activity Research (CFAS) is supported by a grant from TrygFonden, and the Centre of Inflammation and Metabolism (CIM) is a member of DD2—the Danish Center for Strategic Research in Type 2 Diabetes (the Danish Council for Strategic Research, grant nos. 09-067009 and 09-075724).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.