Article Text

Abstract
Objectives This study determined the feasibility of delivering a 12-week structured physical activity programme during chemotherapy to older adults recently diagnosed with metastatic gastrointestinal (GI) cancer.
Methods This study used a single-cohort design. Older adults (aged ≥65 years) diagnosed with metastatic oesophageal, gastric, pancreatic or colorectal cancer who planned to initiate chemotherapy were enrolled. The physical activity programme included a combination of aerobic, flexibility, strength and balance modalities delivered by a certified cancer exercise trainer during chemotherapy infusion appointments, then translated and sustained at home by participants. The co-primary endpoints included: (1) accrual of 20 participants in 12 months and (2) physical activity adherence of ≥50%.
Results Between March and October 2018, 29 participants were screened, and 20 were enrolled within 12 months (recruitment rate: 69% (90% CI: 55% to 83%); p<0.001), meeting the first co-primary endpoint. The median age of participants was 73.3 years (IQR: 69.3–77.2). At week 12, 67% (90% CI: 48% to 85%) of participants adhered to ≥50% of the prescribed physical activity (p=0.079 (statistically significant)), meeting the second co-primary endpoint. From baseline to week 12, accelerometer-measured light-intensity and moderate-intensity to vigorous-intensity physical activity increased by 307.4 (95% CI: 152.6 to 462.2; p<0.001) and 25.0 min per week (95% CI: 9.9 to 40.1; p=0.001), respectively. There were no serious or unexpected adverse events. The median overall survival was 16.2 months (8.4–22.4).
Conclusion These results establish the feasibility of a larger scale randomised controlled trial that enrols older adults with metastatic GI cancer and delivers a structured physical activity programme during chemotherapy.
Trial registration number NCT03331406.
- exercise
- accelerometer
- cancer
- death
- physical activity
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Reduced physical function predicts poor quality of life, chemotherapy toxicity and premature death in adults with metastatic cancer.
Despite the importance of preserving physical function in patients with metastatic cancer, few therapeutic options exist, and there is no standard of care.
WHAT THIS STUDY ADDS
This study established the feasibility of delivering a 12-week structured physical activity programme during chemotherapy to older adults recently diagnosed with metastatic gastrointestinal cancer.
Objectively measured light-intensity physical activity increased by 307.4 min per week (95% CI: 152.6 to 462.2), and moderate-intensity to vigorous-intensity physical activity increased by 25.0 min per week (95% CI: 9.9 to 40.1).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
These results establish the feasibility of a larger scale randomised controlled trial that enrols older adults with metastatic gastrointestinal cancer and delivers a structured physical activity programme during chemotherapy.
Introduction
At the time of diagnosis of metastatic gastrointestinal (GI) cancer, 70% of patients are aged ≥65 years.1 Within the first 12–24 weeks of starting chemotherapy, 40%–60% of patients with metastatic GI cancer will experience a substantial and sustained decline in physical function.2–4 Reduced physical function predicts poor quality of life,5 chemotherapy toxicity6 7 and premature death.8 Despite the importance of preserving physical function in patients with metastatic cancer,9 few therapeutic options exist, and there is no standard of care.10
The decline of physical function may result from the age-related and treatment-related impairments in aerobic capacity,11 ambulatory activity,12 13 and muscle strength and mass.14 15 Randomised controlled trials of older adults without cancer demonstrate that structured physical activity preserves or prevents the deterioration of physical function.16 17 Among patients with early-stage cancer, physical activity increases aerobic capacity,18 ambulatory activity,19 muscle strength and mass,20 and preserves self-reported physical functioning.21 22 However, older adults with cancer have been under-represented in clinical trials, and the evidence establishing the feasibility of physical activity in patients with metastatic cancer receiving chemotherapy remains limited.23 24
This pilot study aimed to determine the feasibility of delivering a 12-week structured physical activity programme to older adults recently diagnosed with metastatic GI cancer. The co-primary endpoints to establish feasibility included: (1) recruitment of 20 participants within 12 months and (2) demonstration that at least 50% of participants adhered to at least 50% of the prescribed physical activity programme.
Materials and methods
Study design
This pilot and feasibility study used a single-cohort design.
Participants
Participants were eligible if they were aged ≥65 years, had a diagnosis of histologically confirmed oesophageal, gastric, pancreatic, or colorectal cancer that was metastatic or locally advanced (unresectable), and initiated first-line cytotoxic chemotherapy within 4 weeks of study enrolment (participants could have received prior therapy if completed ≥6 months before the start of first-line chemotherapy for metastatic disease). Eligible participants self-reported <150 min per week of physical activity at baseline,25 had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, self-reported being able to walk 400 m (approximately one city block) without sitting, leaning, or the help of another person or walker, provided voluntarily signed informed consent and had an estimated life expectancy of >3 months.
Participants were ineligible if they had known or suspected brain or other central nervous system metastases, uncontrolled cardiac or pulmonary disease, were pregnant or breast feeding, or had any other condition that could impede testing of the study hypothesis, making it unsafe to engage in the physical activity programme, or made the participant not available for end-of-study assessments (determined by the investigative team).
Under approval of a Health Insurance Portability and Accountability Act (HIPAA) waiver, potentially eligible patients were identified by the study coordinator, who systematically screened all relevant oncology clinic schedules for new or follow-up appointments. The study coordinator contacted the healthcare provider to request permission to approach the patient as patients were identified. After obtaining approval, the study coordinator approached the potential participant during a clinic visit to provide information about the study and complete informed consent.
Structured physical activity programme
A certified cancer exercise trainer delivered the structured physical activity programme during chemotherapy infusion appointments (eg, requiring no additional appointments for participation), then translated and sustained at home by participants. The physical activity programme was 12 weeks. The programme included a combination of aerobic, flexibility, strength and balance activities, as used in the Lifestyle Interventions and Independence for Elders (LIFE) clinical trials programme.16 17 The LIFE physical activity programme was tailored to the unique needs of patients with metastatic cancer (table 1). All participants were provided with a pedometer to objectively monitor their aerobic activity and variable ankle weights for strength activity. Physical activity goals were individualised based on each participant’s baseline physical fitness and functional status level. The programme included a weekly goal of 150 min of aerobic activity, consistent with the Physical Activity Guidelines for Americans.26 Participants completed flexibility activities following each bout of walking. Participants completed lower extremity muscle strengthening exercises (three sets of each exercise for 10 repetitions) using variable weight ankle weights. Balance training was introduced as a complement to the aerobic and strength components. The programme included in-person instruction, home-based activity and telephone behavioural support. On the weeks that chemotherapy was not administered, the exercise trainer phoned the participant to promote exercise adherence, discuss barriers to exercise and review any changes in symptoms due to chemotherapy to develop goals for the following study week. Physical activity goals were modified in response to illness, injury or treatment-related symptoms. The programme was guided by the social cognitive model of behaviour change to improve physical activity self-efficacy, goal setting and outcome expectancy.27
How the physical activity programme in the Lifestyle Interventions and Independence for Elders (LIFE) clinical trials was adapted and tailored in this pilot study of older adults with metastatic gastrointestinal cancer
Primary outcome measures
The co-primary endpoints to establish feasibility included: (1) the rate of accrual onto the study protocol and (2) adherence to the physical activity programme. Co-primary study endpoints were selected because the investigators considered the ability to recruit the target population and deliver the intervention equally important to establish feasibility for a larger scale, randomised trial designed to evaluate the efficacy of physical activity on an objectively measured physical function endpoint.
The rate of accrual co-primary endpoint was quantified as the number of days required to enrol 20 participants. The study was required to recruit 20 patients within 12 months. This endpoint was chosen to ensure that an adequate sample size could be expected to be recruited for a larger phase II multicentre trial within the scope of a research project grant programme (eg, 3-year recruitment time horizon).28 29
The adherence to the physical activity programme co-primary endpoint was quantified as the proportion of days the prescribed aerobic, flexibility, strength and balance activities were completed. Adherence was quantified from daily self-reported exercise logs that included documentation of pedometer step counts. To achieve this endpoint, the study was required to demonstrate that at least 50% of participants adhered to at least 50% of the prescribed physical activity programme. This adherence rate was chosen based on the accepted feasibility threshold for early phase clinical trial programmes.30
Secondary outcome measures
Secondary study outcomes were selected to refine and streamline the delivery and implementation of the structured physical activity programme to the target population. The secondary endpoints included: (1) rate of retention, defined as the proportion of participants who completed the study; (2) rate of assessment measure completion, defined as the proportion of participants who completed all physical function and questionnaire data collection (described below); (3) rate of adverse events, defined as the proportion of participants who experience at least one fall, hospitalisation, or musculoskeletal injury that was determined to be possibly, probably, or definitely related to the study. A post hoc descriptive endpoint was the proportion of participants who died during the 12-week study and after study completion.
Other measures
Light-intensity and moderate-intensity to vigorous-intensity physical activity (minutes per week) were quantified using a triaxial waist accelerometer (ActiGraph GT3X+) with established intensity thresholds.31 Four days of valid wear with ≥600 min each day were required for analysis. Handgrip strength was quantified using a hydraulic dynamometer (Jamar).32 Aerobic capacity was quantified by the long-distance (400 m) corridor walk.33 Lower extremity function was quantified by the Short Physical Performance Battery (SPPB), a standardised measure that includes walking, balance and strength.34 35 The Medical Outcome Survey Short Form (SF)-36, and Functional Assessment of Cancer Therapy (FACT-G, V.4), were used to quantify the patient-reported health-related quality of life.36 37 Follow-up measures were collected during a chemotherapy infusion visit after the 12-week physical activity intervention. Baseline characteristics, including the type of GI cancer, sites of metastases and ECOG performance status, were obtained from healthcare provider records. Questionnaires developed by the National Center for Health Statistics were used to ascertain demographic characteristics. A validated self-reported questionnaire ascertained adverse events related to physical activity (eg, musculoskeletal injury).38 Overall survival was monitored using the medical record and death registry.
Statistical analysis
A target accrual of 20 participants was selected on what investigators hypothesised to be a reasonable sample size to accrue at a single site over a 1-year time horizon. Twenty participants would provide sufficient data to calculate the rate of accrual onto the study protocol and stable estimates regarding the extent to which participants could adhere to the prescribed physical activity programme. Under the null hypothesis of a 5% recruitment rate, a 25% recruitment rate would provide 79% statistical power for a one-sided test hypothesis test with an alpha error of 10% (eg, a p value less than 0.10 would be declared statistically significant). Under the null hypothesis for a 25% physical activity adherence rate, a 50% adherence rate provides 83% statistical power for a one-sided hypothesis test with an alpha error of 10%. The null hypotheses for both outcomes were set at the point at which investigators would be unwilling to pursue a larger scale trial (eg, 1 in 20 patients who were approached choose to enrol in the study and one-quarter of all prescribed physical activity could be completed). The ability to simultaneously reject both hypotheses would provide sufficient confidence to move this study into a larger setting designed to evaluate efficacy. Rates and CIs were calculated using the binomial method.39 Changes in accelerometer-measured physical activity were used as an objective measure to supplement self-reported physical activity logs. All other analyses are descriptive and hypothesis-generating.
Patient and public involvement
No patients or members of the public were involved in the design, conduct, reporting or dissemination plans of our research.
Results
Between March and October 2018, 29 patients were assessed for eligibility and 20 participants were recruited, with primary data collection completed in January 2019. Of the nine patients who were not enrolled, six were ineligible because they were already sufficiently physically active and three reported a general theme of being overwhelmed with their recent diagnosis and unwilling to assume additional demands on their time.
The first co-primary study endpoint to recruit 20 participants within 12 months was met; 29 participants were screened, and 20 were enrolled over 240 days (recruitment rate: 69% (90% CI: 55% to 83%); p<0.001). The median (IQR) time from diagnosis of metastatic cancer to study enrolment was 26 days (14–43), and the physical activity programme was initiated with a median of 10 days (7–14) after study enrolment.
The median age of enrolled participants was 73.3 years (69.3–77.2); six (30%) participants were aged ≥75.0 years (table 2). Participants were most often diagnosed with pancreatic cancer (n=13 (65%)), had liver metastases (n=14 (70%)) and had baseline ECOG performance status of 1 (n=14 (70%)). After enrolment and before providing baseline study measures, two participants withdrew due to declining health (n=1) and transition to hospice care (n=1; figure 1).
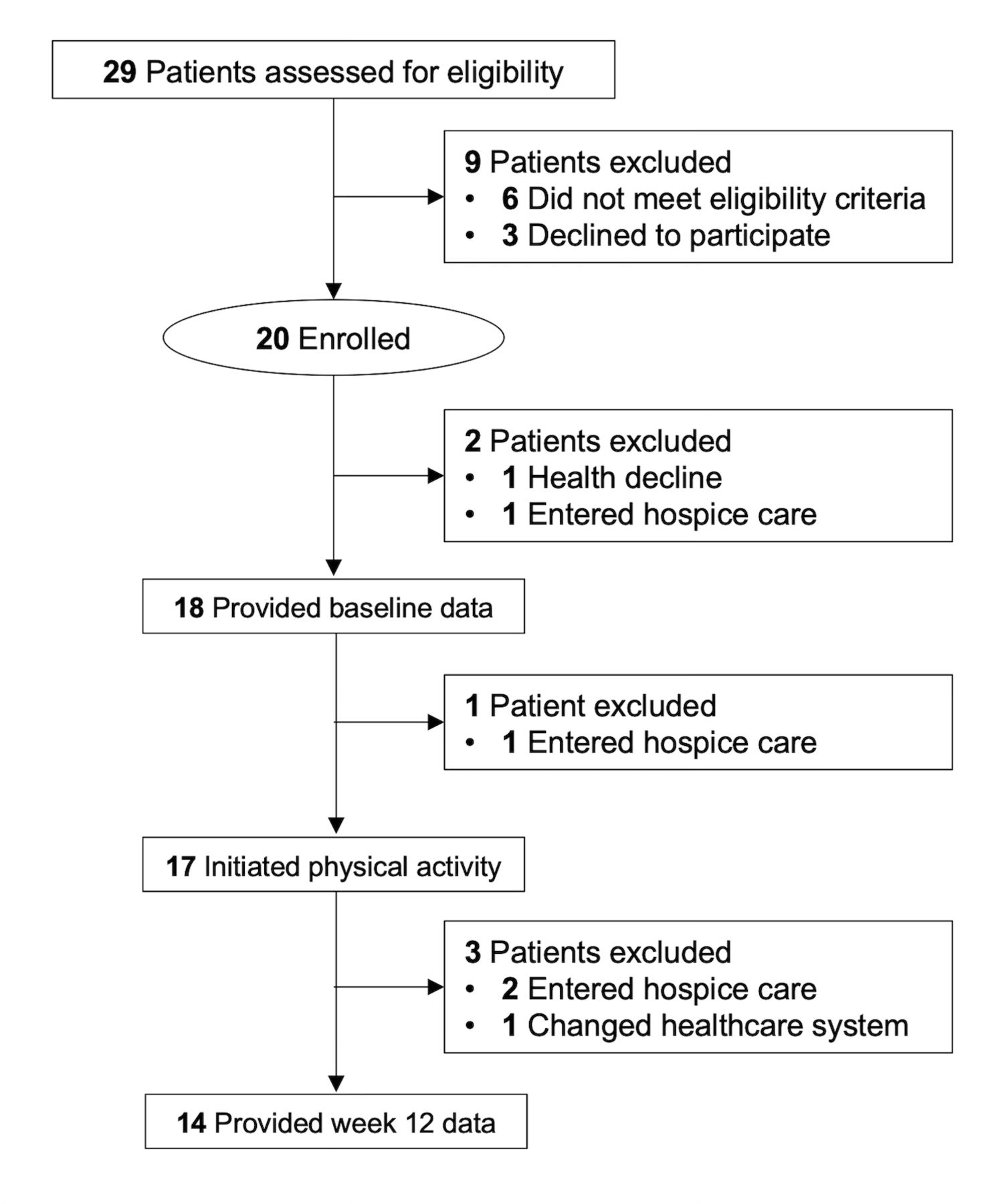
Flow of participants.
Characteristics of study participants (N=20)
Among the 18 participants who provided baseline study measures, the median handgrip strength was 32.5 kg (26.0–36.0), 400-metre walk time was 5.5 min (4.9–6.5), SPPB score was 11 (10–12) and 4-metre gait speed was 1.0 m/s (0.9–1.3), indicating good objectively measured physical function. At baseline, the median SF-36 physical health subscale score was 50.0 (30.6–67.5), mental health subscale score was 47.5 (36.6–57.5) and FACT-G score was 64.0 (33.7–82.5), indicating a good self-reported quality of life.
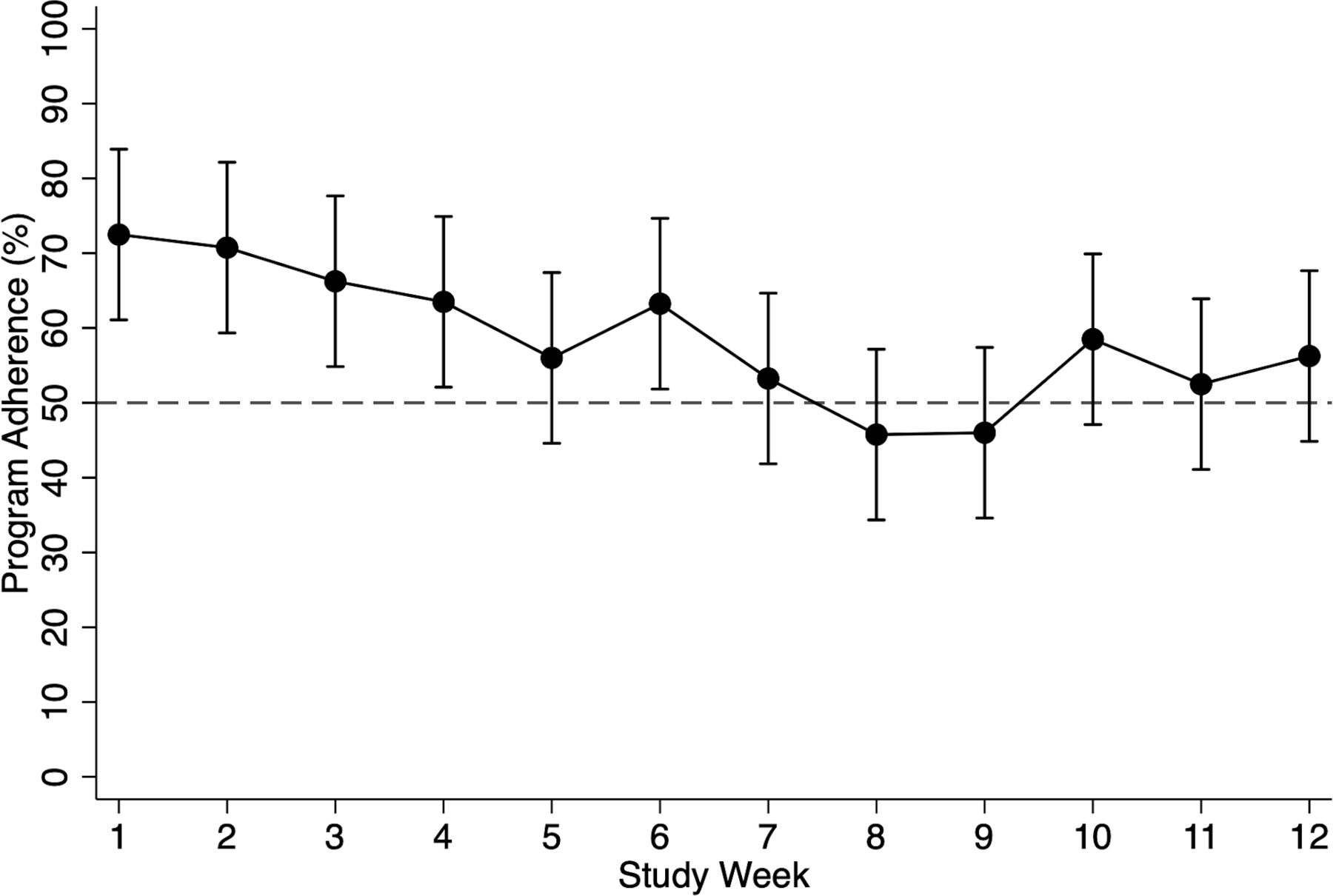
One participant did not begin the physical activity programme due to declining health (this participant was analysed as having 0% physical activity adherence in the analysis). Two participants transitioned to hospice care after starting the physical activity programme. One participant transitioned care to another health system (these participants were analysed as having 0% physical activity adherence after transitioning out of the study). The second co-primary study endpoint to demonstrate that at least 50% of participants adhered to at least 50% of the prescribed physical activity programme was met; at week 12, 67% (90% CI: 48% to 85%) of participants adhered to at least 50% of the prescribed physical activity programme (p=0.079 (statistically significant); figure 2). From baseline to week 12, light-intensity physical activity increased by 307.4 min per week (95% CI: 152.6 to 462.2; p<0.001) and moderate-intensity to vigorous-intensity physical activity increased by 25.0 min per week (95% CI: 9.9 to 40.1; p=0.001; table 3).

Adherence to the physical activity programme by study week. Error bars depict 95% CIs.
Accelerometer physical activity outcomes at baseline and change at week 12
The retention rate at week 12 was 78% (90% CI: 62% to 94%). Among participants retained at week 12, the rate of assessment measure completion was 100%. From baseline to week 12, we observed a non-significant decline in handgrip strength (−2.6 kg (95% CI: −5.7 to 0.4)), but 400-metre walk time (−0.01 min (95% CI: −0.1 to 0.1)), SPPB score (−0.1 points (95% CI: −3.3 to 3.1)) and gait speed (−0.02 m/s (95% CI: −0.13 to 0.09)) remained stable. The SF-36 physical health subscale score modestly but non-significantly declined (−3.4 points (95% CI: −9.6 to 2.7)), whereas the mental health subscale score modestly but non-significantly increased (7.8 (95% CI: −1.7 to 17.3)); the FACT-G score declined on average, but variation was wide (−4.4 (95% CI: −20.5 to 11.6)).
There were no adverse events that were determined to be considered by the medical investigator as definitely, probably or possibly related to the study. No participants died during the 12-week intervention. The median overall survival was 16.2 months (8.4–22.4); 70% of participants were alive at 12 months (figure 3).

{kind=link}
{kind=link}
{kind=link}
Overall survival of study participants. Dashed vertical line represents end of physical activity programme. Shaded bands depict pointwise 95% CIs.
Discussion
The co-primary endpoints of this pilot and feasibility study of physical activity for older adults with metastatic GI cancer were met. Twenty participants were recruited within 12 months and at least 50% of participants adhered to at least 50% of the prescribed physical activity programme. In addition, the accelerometer-measured light-intensity and moderate-intensity to vigorous-intensity physical activity increased by 307 and 25 min per week, respectively. No unexpected or serious safety signals were identified, and no participants died during the 12-week intervention. This pilot and feasibility study provides critical foundational data to inform a randomised trial designed to evaluate the efficacy of physical activity on an objectively measured physical function endpoint.
The population of older adults with metastatic GI cancer face dual challenges: (1) the decline in physiological reserve due to both metastatic cancer and ageing; and (2) the toxicities from treatment.40 41 The unfavourable synergy from ageing with cancer and chemotherapy—a double hit to key physiological systems—manifests as accelerated declines in function.42 43 We hypothesise that the deterioration of physical function in patients with cancer is from age-related and cancer treatment-accelerated declines in aerobic capacity,11 ambulatory activity,12 13 and muscle strength and mass.14 15 Supporting this hypothesis is the observation that patients with cancer have a lower aerobic capacity,44 ambulatory activity,45 muscle strength46 and muscle mass,47 compared with matched control participants who do not have a history of cancer.
Examining the feasibility of a structured physical activity programme in older adults with metastatic GI cancer was motivated by the observation that participation in physical activity is one of the strongest predictors of physical function among older adults without cancer.48 49 Physical functions, such as walking or locomotion, have been a primary emphasis of natural selection throughout human evolution.50 This has resulted in redundant sets of physiological systems—including the cardiovascular, pulmonary, neurological and musculoskeletal—that work in conjunction to enable physical function. When one physiological system becomes compromised, other systems compensate.51 Consequently, declines in physical function become clinically evident only when this extensive network of physiological reserves becomes depleted, and other compensatory systems have failed.52 This decline in physical function erodes quality of life,5 increases the likelihood of experiencing chemotherapy toxicities,6 7 which constrains opportunities to receive additional life-sustaining therapies and consequently increases the risk of death.8 We have proposed physical function as a biomarker that synchronously describes the performance and coordination of various physiological systems that may be impaired because of ageing and cancer treatment.53
The increase of 307 min per week light-intensity physical activity and 25 min per week of moderate-intensity to vigorous-intensity physical activity may be clinically valuable. Higher volumes of light-intensity physical activity are associated with a reduced risk of developing mobility disability among older adults.54 Moderate-intensity to vigorous-intensity physical activity is associated with dose-dependent changes in the SPPB and gait speed, and relatively small increases (~48 min per week) in moderate-intensity to vigorous-intensity physical activity are associated with meaningful reductions in the risk of major mobility disability.55 In a meta-analysis of 11 studies, higher volumes of light-intensity physical activity were associated with a lower risk of death, independently of the volume of moderate-intensity and vigorous-intensity physical activity.56 It is important to recognise that accelerometer-defined light-intensity physical activity may be consistent with the energy expenditure of moderate or vigorous-intensity physical activity in older adults.57
Recently introduced treatment options for patients with metastatic GI cancers have significantly extended overall survival. Among patients with metastatic colorectal cancer, overall survival has improved threefold in the past 20 years.58 Among patients with metastatic pancreatic cancer, a chemotherapy regimen consisting of oxaliplatin, irinotecan, fluorouracil and leucovorin compared with gemcitabine as first-line therapy improves overall survival by 40%.59 Among patients with metastatic gastric cancer, a combination of nivolumab and chemotherapy compared with chemotherapy alone as first-line therapy improves overall survival by 30%.60 This has created an opportunity to develop interventions that prevent the loss of physical function to maximise quality of life while patients receive life-prolonging therapy.61
There are limitations to this study. The principal limitation is the small sample size of recruited participants from a single cancer centre. It is possible that the participants who chose to enrol in this study were not like patients who did not enrol. The intervention length was limited to 12 weeks, which precludes our ability to comment on the ability of participants to adhere to this programme over a longer time horizon. Our study was not designed with the intent of conducting extensive null hypothesis significance testing on study outcome measures.
There are strengths to this study. This study successfully recruited older adults, who are often under-represented in clinical trials. Moreover, study participants had a variety of GI malignancies, such as pancreatic cancer, which are less commonly studied in the context of lifestyle modification trials. This study used an evidence-based physical activity programme that has been proven efficacious in preventing a functional decline in healthy older adults.16 17 The physical activity programme was tailored to the unique needs of patients with metastatic cancer. The physical activity programme required minimal equipment and was predominately home based in a manner that could be broadly disseminated in a nationwide trial. Moreover, during the COVID-19 pandemic, virtual physical functioning assessments were validated for cancer survivors,62 and the implementation of these methods may improve the accessibility of clinical trials to older adults.63
Conclusion
Prolonging the overall survival of patients with metastatic GI cancer is an important clinical objective. However, of even greater importance is that extensions in overall survival include a preserved capacity to live independently and function well. Upon commencing life-sustaining chemotherapy, many older adults with metastatic GI cancer experience precipitous declines in physical function. Despite the importance of preserving physical function in this vulnerable population, few therapeutic options exist. Preventing physical function decline is an important goal in providing evidence-based, patient-oriented, geriatric palliative cancer care. The results from this study establish the feasibility of a larger scale randomised controlled trial that recruits older adults with metastatic GI cancer and delivers a structured physical activity programme during chemotherapy.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted following Good Clinical Practice and the ethical principles in the Declaration of Helsinki. The study protocol and informed consent document were reviewed and approved by the Institutional Review Board of Dana-Farber/Harvard Cancer Center (protocol #17.350) before engaging in study-related activities. All participants provided written informed consent and received approval from their qualified healthcare provider to enrol in the study.
Acknowledgments
We thank Melissa Harris, Phillip Nauta and Harrison Travis for assistance with accelerometer data curation and analysis.
References
Footnotes
Contributors JCB and JAM contributed to conceptualisation and project planning. JCB, EB and JAM had full access to the data in the study and take responsibility for the integrity and accuracy of the data analysis. All authors performed interpretation of data. All authors contributed significantly to the writing of this paper. All authors have read and approved the final version of the manuscript to be submitted. JCB is responsible for the overall content as the guarantor of this report.
Funding This work was supported by the National Cancer Institute of the National Institutes of Health under Award Number R00-CA218603; the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under Award Number P30-DK072476; and the National Institute of General Medicine Sciences of the National Institutes of Health under Award Number U54-GM104940.
Competing interests JCB reported receiving grants from the National Institutes of Health and the American Institute for Cancer Research. JC reported research funding to his institution from Merus, Roche and Bristol Myers Squibb; he reported research funding from Merck, AstraZeneca, Esperas Pharma, Bayer and Tesaro; he reported honorarium for being on the advisory board of Syros Pharmaceuticals and Blueprint Medicines. MY reported receiving grants from Janssen Pharmaceuticals and personal fees from UpToDate for peer review services. JM reported receiving personal fees from Taiho for grant review for the National Comprehensive Cancer Network, fees for serving on the advisory boards of COTA Healthcare and Ignyta Single, and institutional support from Boston Biomedical for a clinical trial outside the submitted work.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.