Article Text

Abstract
Physical activity (PA) has evidence-based benefits for physical, social and mental health, but investigation of how PA interventions for patients with chronic disease affects their PA practice up to 1 year after programmes are rare. Moreover, few studies document how the context and intervention mechanisms of PA programmes affect sustainable PA practice and its determinants. The present protocol describes a mixed methods study comparing the effectiveness and conditions for the effectiveness of two PA resumption programmes (a hospital-led and a community-based programme). Using a comparative longitudinal study, 60 patients (3-month duration) will be followed for 1 year though four data collections: before (T0) and at the end (T1) of the intervention, 6 months (T2) and 1 year (T3) after the start of the programme. The primary outcome will be PA practice in min/week and categorised as light, moderate or vigorous (using International Physical Activity Questionnaire (IPAQ)), and secondary outcomes will include sedentary time in min/week (IPAQ), quality of life evaluated though the physical and mental composite scores (‘Medical Outcome Study Short Form 12’), and enjoyment using four statements rated from 1 to 5, a high score being synonymous of enjoyment (Intrinsic Motivation Inventory). Qualitative data on further determinants of PA practice and intervention mechanisms will be collected. The expected results will offer the opportunity to understand how the intervention context contributes to a more effective, sustainable PA practice. Trial registration number: NCT04954209.
- physical activity
- sports rehabilitation programs
- chronic
- non-communicable disease
Data availability statement
No data are available. Study is about to start.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Physical activity (PA) has evidence-based benefits for physical, social and mental health and is an integral part of treatment for chronic diseases. Unfortunately, patients who have been sedentary or far from PA practice have difficulties sustaining this PA practice after PA resumption programmes.
What are the new findings
This study will provide a better understanding of the intervention effectiveness of two different PA resumption programmes (hospital-led and community-based) among patients with long-term disease as well as the intervention mechanisms and determinants (psychological, social and community) of sustainable PA practice during and after these PA resumption programmes.
Introduction
In 2017 in France, 10.7 million patients (17% of the insured population)1 were diagnosed with at least 1 of the 30 chronic diseases defined as ‘diseases with an expensive and long-term treatment, which can be paid by the health insurance’.2,3 Moreover, the prevalence of patients with chronic disease has increased by 4% between 2006 and 2011 and 5% between 2011 and 2017.4 Beyond affecting individual health, chronic diseases also have high financial cost, estimated at €86 billion in 2015 in France.5 Furthermore, wide disparities have been observed in social6 and territorial1 inequalities, with higher prevalence of chronic disease in deprived areas.
One factor playing a key role in chronic disease prevention and management is physical activity (PA). Evidence has demonstrated the benefits of PA on physical, social and mental health.7 As stated in the French government’s guidelines,8 PA is now considered as an integral part of chronic disease treatment.9 The WHO recommends at least 150–300 min of moderate-intensity PA, or 75–150 min of vigorous-intensity PA, or an equivalent combination of moderate-intensity and vigorous-intensity aerobic activity, per week for adults in the general population and adults with chronic conditions.10
In 2019 in France, 61% of patients were recommended to practice PA by their doctors, and 36% of these were directed toward a PA resumption programme, ‘programmes passerelles’.11 Designed for people who want to maintain or improve their health by practicing PA, PA resumption programmes are defined as ‘resumption programme(s) of adapted PA, framed by professional coaches, limited in the time, aimed to improve the physical condition, to make people practicing in autonomy, safety, regularly and persistently’.12
Both community-based and medically supervised programmes have shown mixed results in improving sustainable PA practice. A review showed that half of included community-based PA programmes showed positive PA outcomes. A literature review of exercise referral schemes showed a significant increase in the number of sedentary people becoming moderately active but also poor participation and observance. A second review showed no long-term impact on PA practice of exercise referral schemes.13 14 In other words, previous studies have expressed doubts over the effectiveness of the programmes, especially because of the non-sustainability of PA practice.15
Previous studies have shown different factors affecting patients’ commitment to PA resumption programmes16 17: practice conditions and motivation (eg, enjoyment, feeling of self-efficiency, quality of life); sociodemographic factors, education and knowledge (eg, benefits of PA, disease management); and medical factors (improvement of health condition, pharmaceuticals). Moreover, a literature review of programme design showed that key factors for sustainable practice were perceived support, defined goals and motivation, professional advice and supervision during and after the programme, incentives, social engagement with other participants and accessibility.15
To further contribute to the understanding of PA resumption programme mechanisms for sustainable PA practice, the present study, part of the PERSISTE project (Promotion et pERennité de l’activité phySIque SantE—Promotion and sustainability of health enhancing PA), will compare the effectiveness (maintenance of PA practice up to 1 year after the programme) and conditions for the effectiveness (health determinants and intervention mechanisms influencing PA practice) of two PA resumption programmes (one hospital-led and one community-based) on PA practice from entering the programme to 1 year later.
Research hypothesis
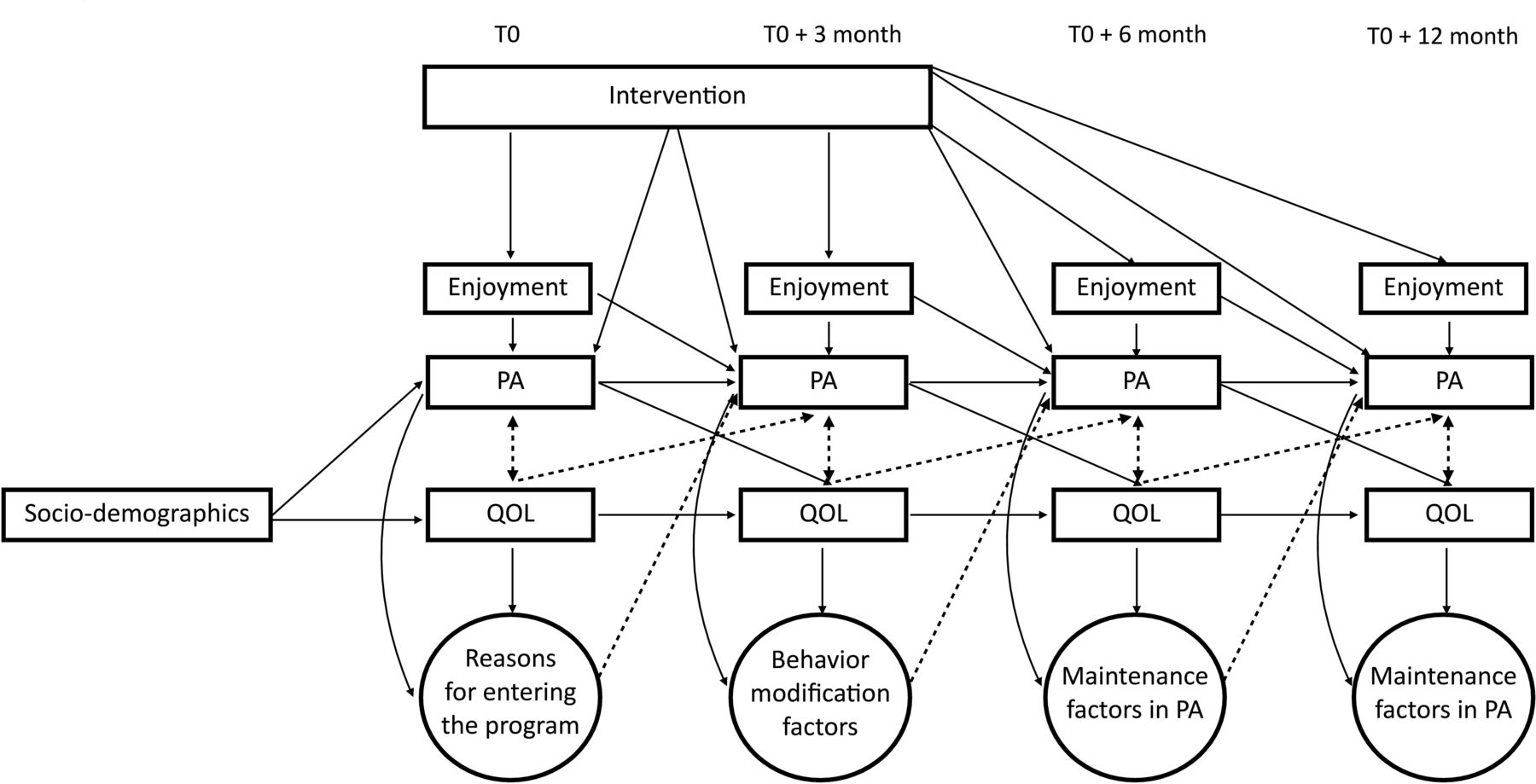
To evaluate the effectiveness of PA resumption programmes, we postulate that in comparison to a hospital-led programme, a community-led programme (including discovery sessions by local sports clubs) will increase light, moderate and vigorous PA practice and organised sports activities at 6 months and 1 year after entering the programme, which in turn will increase quality of life at 6 months and 1 year after entering the programme (see figure 1). We will also conduct an exploratory analysis to examine which PA determinants (eg, enjoyment measured quantitatively via questionnaire) and PA resumption programme mechanisms (identified from the qualitative data) support sustainable PA practice.
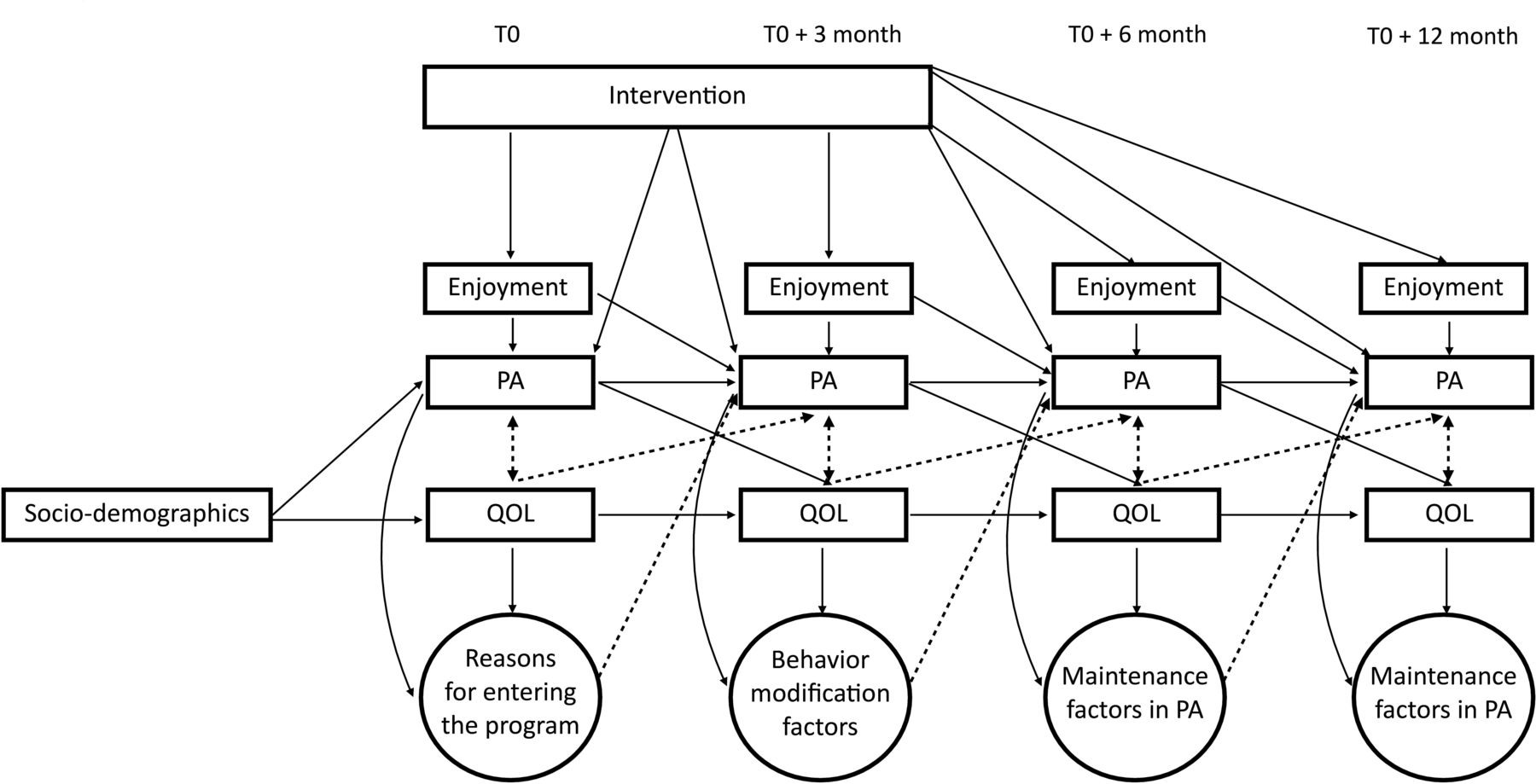
Presumed interactions between sociodemographics data, intervention variables, physical activity (PA), quality of life (QOL), enjoyment in PA and qualitative data from interviews.
Methods
Research design
The present study is a multicentre, longitudinal observational comparative study with a convergent parallel mixed methods design.18 The multicentred, observational and comparative study involves observing two PA resumption programmes, the first hospital led and the second community based, without modifying or altering the ongoing programme. The design is longitudinal in that patients are followed for 1 year (T0, T0+3 months, T0+6 months, T0+12 months) (figure 2).

{kind=link}
{kind=link}
Scheme of the comparative study. IPAQ, International Physical Activity Questionnaire; IMI, Intrinsic Motivation Inventory; SF-12, 12-item Short Form.
The design will use a parallel mixed methods QUANT+QUAL study because in the first phase, quantitative data (attendance, quality of life, motivation assessed by questionnaires) and qualitative data (interviews on the reasons for continuing or abandoning PA practice) will be collected at the same time (parallel) and combined during data analysis (convergent). In other words, quantitative data will inform the PA, organised sport practice and quality-of-life evolution, whereas qualitative data will explore wider PA practice determinants and intervention mechanisms.
Study settings
The present study will be based on two PA resumption programmes implemented in Seine-Saint-Denis, a socially deprived area outside of Paris: the community-led programme Le Défi Forme Santé (DFS) in La Courneuve and a hospital-led programme in the Bondy area, at the Centre Hospitalier Universitaire Jean Verdier (CHU JV).
Both programmes target sedentary people with long-term diseases and offer a 3-month adapted PA programme. They share similar objectives: to support patient’s engagement and sustainable, autonomous PA practice. Nevertheless, they differ in their content and organisation leadership. The DFS programme welcomes patients outside of a medical structure, in different community locations (indoors and outdoors), and offers activities such as muscle strengthening, aquafit sessions and Nordic walking. The programme also encourages local sports clubs to recruit participants by offering specific sessions in the programme or inviting them to practice their own sport. The CHU JV programme is fully integrated into the hospital’s sports medicine and rehabilitation department. All care is provided within the hospital itself. Patients will experience cardiovascular work, muscle strengthening and other fun and play activities. In both programmes, the sessions will last from 1 to 2 hours and will be supervised by educators in adapted physical activities and/or sport–health educators. Participants will be encouraged to practice at least three sessions per week at the JV CHU and up to five at the DFS. During the programmes and outside of the supervised sessions, participants will be encouraged to adopt an active lifestyle, but will not be especially encouraged to practice PA autonomously given the volume of supervised practice.
Sample size
The primary outcome of the study will be PA practice at 6 months and 1 year after the programme. According to preliminary data collected from 255 people for a Master 2 Sports Sciences thesis,19 57% of the people involved in the DFS programme continued to practice PA at 6 months. From a review of the literature13 on the effectiveness of hospital-based PA programmes, we estimate that 20% of participants will reach the recommendations for PA practice at 6 months and 1 year after the CHU JV programme. Assuming that 57% of the DFS patients and 20% of the CHU JV patients will reach the PA recommendations, with a 5% alpha risk and a power of 80%, we will need at least 52 participants, 26 in each group (epiR package 0.9–96) to compare the two programmes. Assuming a 10% dropout rate (three patients/location) during follow-up, we can expect to include and follow a total of 60 patients, or 30 patients per programme: three patients included per month per programme for 12 months.
Recruitment
The inclusion criteria will be 18 years of age and older, having a long-term condition, enrolled in the DFS or CHU JV PA resumption programme between October 2021 and September 2022, ensured medical fitness to participate in the PA programme and being informed and giving oral consent to participate.
Measurement
Individual demographic and socioeconomic criteria collected by questionnaires will include age, sex, education level, socioprofessional category, type of professional activity, marital status and socioeconomic status. Medical criteria will include the type of chronic disease. In both programmes, the primary outcome will be the amount of light, moderate and vigorous PA measured by using the International Physical Activity Questionnaire (IPAQ). The IPAQ is a validated international questionnaire that has been translated into several languages,20 including French, and has been used across similar samples. The IPAQ will be used to measure PA level over the previous 7 days (in min/week and categorised as light, moderate or vigorous) based on three indicators: frequency, duration and intensity. Sedentary behaviour (in min/week) will also be measured over the previous 7 days.21 Secondary outcomes will include a record of attendance at sessions during the resumption programme, participation in organised sport practice and sedentary behaviour. Further secondary outcomes are quality of life and enjoyment in PA practice.
Quality of life will be evaluated by the Medical Outcomes Study 12-item Short Form (SF-12) questionnaire, validated at the international level, including in French.22 The SF-12 questionnaire is a general health assessment questionnaire evaluating two dimensions: the physical composite score and the mental composite score divided into eight subdimensions (PA; life and relationships with others; physical pain; perceived health; vitality; limitations due to mental state; limitations due to physical state; mental health) and questions the individual about the last 4 weeks.
Enjoyment in PA will be measured by using the Intrinsic Motivation Inventory (IMI) Questionnaire. This scale, not validated in French but used in different studies23 among the sport population, determines the enjoyment in the practice of PA over a given period. Using four statements (eg, ‘I liked the activities I did’), responses are rated on a scale of 1–5, from 1, ‘strongly disagree’, to 5, ‘strongly agree’. A high score indicates a high level of enjoyment of PA.
Further PA determinants investigated by interview will include reasons for entering the programme, intraprogramme factors that modified PA behaviour (pedagogy, timeframe, relationships etc), territorial characteristics affecting PA practice, and qualitative information on the practice of PA after the programme (type of activity, autonomous, supervised, in which structure).
Data collection
Data will be collected at inclusion (T0, at enrollment in the PA resumption programme), at 3 months (end of the bridging programme), and at 6 and 12 months after inclusion. Data will be recorded in each participant’s individual tracking book, and semistructured interviews will be recorded.
Inclusion in the study (T0) will be performed by the sport–health educator at the time of enrolment in the PA resumption programme. The study will be presented to patients who meet the inclusion criteria. The sport–health educator will inform the patient and orally collect the patient’s non-opposition to participate as well as non-opposition to use of the patient’s data. If the patient agrees, the sport–health educator will collect sociodemographic data and administer the IPAQ, IMI and SF-12. The patient will then be informed of a future face-to-face or telephone appointment for a semistructured individual interview with the principal investigator about the reasons for entering the programme. The patient will be given a letter of information in the follow-up booklet on the progress of the study along with the contact details of the principal investigator of the research. A similar procedure will apply at each data collection, including questionnaire collection by the programme educator and interview with the principal investigator (see table 1 for details).
Data collection and measurement of variables
Data analysis
A descriptive analysis will be performed for all variables collected at each measurement time. Univariate and multivariate analysis of variance (ANOVA and MANOVA) will be used for comparing the two programmes, controlling for confounders and statistical assumptions to run such analysis. Specifically, ANOVA and MANOVA will be used to compare light, moderate and vigorous PA; sedentary time; and compliance with the programme. A similar analysis will be used for secondary outcomes (quality of life, enjoyment). PA trajectories will be identified, to examine PA profiles of patients through time, in particular at the four times (T0, T1 (T0+3 months), T2 (T0+6 months), T3 (T0+12 months)), by investigating PA, quality of life and enjoyment using a ‘latent class growth analysis’ method. This will permit factors determining whether individuals meet PA recommendations or not to be identified. The relations between the variables (as shown by figure 1) will be modelled by structural equation modelling by using AMOS software.
The qualitative data analysis will help refine the determinants of continued PA practice (see table 2 for details) by using a thematic coding and if necessary, quantification of qualitative data.24 Interviews will be fully transcribed, and a thematic content analysis will involve using Nvivo software.
Description of the mixed method design
The integration of qualitative and quantitative data will include the use of quantitative data as a basis for the qualitative study. In addition, the qualitative data from the exploratory question will be used to complete the analysis in order to specify the effect of discovery sessions organised by local sport clubs on the DFS resumption programme.
Discussion
There has been a recent development of PA resumption programmes in France.25 However, mixed results from previous literature reviews12–15 limit the ability to understand the effectiveness of such programmes, or how they can be implemented effectively to support sustainable PA practice in patients with chronic disease. Considering the evidence-based benefits of PA and its recognition as treatment for chronic conditions,8 understanding how PA determinants and the intervention context could best support patient long-term engagement remains a challenge. Recent research has focused on community-based26 or hospital-based27 PA programmes, but the present work is unique in comparing how these settings could support sustainable PA practice. The mixed methods protocol, based on the experience of patients in two PA resumption programmes, should allow for identifying wider political, social, territorial, psychological PA determinants as well as the intervention and contextual mechanisms affecting sustainable PA practice. The collection of quantitative and qualitative data should allow for better coverage of the plurality of factors, for a whole systems approach, not just focusing on the individual level.15 The analysis of the data should highlight the interactions between the determinants from the individual to settings as well as their effects and interactions over time. The results of the study should allow for understanding which PA resumption programmes work, for whom and how, to support sustainable PA practice.
Data availability statement
No data are available. Study is about to start.
Ethics statements
Patient consent for publication
Ethics approval
The French National Person Protection Committee (Comité de Protection des Personnes) has approved the study (protocol no. 2021-A01863-38). Before filling out the questionnaires, participants will read the letter of information about the study on the first page, and will give their written passive consent (using the following statement: ‘by filling this questionnaire you agree that your data could be used for the present research’) to participate in the questionnaire leaflet directly. In addition, before starting the interviews, their oral active consent will be collected though the question: ‘do you agree to respond my questions and to be recorded’? Participants will be informed that they can drop out of the study at any time without consequences.
Acknowledgments
The authors acknowledge the surgeons responsible for the two programmes, Anne-Louise Avronsart and François Lhuissier; and the main sport and health educators, Lamine Camara, Romain Yhuel.
Footnotes
Contributors OR, AVH and AV made substantial contribution to the conception of the design of the protocol and gave feedback on the manuscript. OR, AVH and AV read and approved the submitted version of the manuscript.
Funding This project was funded by the “Comité Départemental Olympique et Sportif de Seine Saint Denis”. The funding is dedicated to project management, data collection and analysis. Intellectual properties belong to the research team
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.