Article Text

Abstract
Objectives Chronic painful insertional Achilles tendinopathy is known to be difficult to manage. The diagnosis is not always easy because multiple different tissues can be involved. The plantaris tendon has recently been described to frequently be involved in chronic painful mid-portion Achilles tendinopathy. This study aimed to evaluate possible plantaris tendon involvement in patients with chronic painful insertional Achilles tendinopathy.
Methods Ninety-nine consecutive patients (74 males, 25 females) with a mean age of 40 years (range 24–64) who were surgically treated for insertional Achilles tendinopathy, were included. Clinical examination, ultrasound (US)+Doppler examination, and surgical findings were used to evaluate plantaris tendon involvement.
Results In 48/99 patients, there were clinical symptoms of plantaris tendon involvement with pain and tenderness located medially at the Achilles tendon insertion. In all these cases, surgical findings showed a thick and wide plantaris tendon together with a richly vascularised fatty infiltration between the plantaris and Achilles tendon. US examination suspected plantaris involvement in 32/48 patients.
Conclusion Plantaris tendon involvement can potentially be part of the pathology in chronic painful insertional Achilles tendinopathy and should be considered for diagnosis and treatment when there is distinct and focal medial pain and tenderness.
Level of evidence IV case series.
- achilles
- tendinopathy
- tendinosis
- surgery
- ankle
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings
The plantaris tendon can potentially be involved in patients with chronic insertional Achilles tendinopathy and should be considered for diagnosis and treatment.
Distinct medial tenderness during clinical examination is suggestive of plantaris tendon involvement in chronic insertional Achilles tendinopathy.
Ultrasound and colour Doppler scanning seem less reliable for diagnosis than medial tenderness.
Introduction
Insertional Achilles tendinopathy is known to be difficult to treat as multiple different tissues can be involved in the pathogenesis.1 2 The subcutaneous and retrocalcaneal bursae, the bone insertion and the distal Achilles tendon, can alone or in combination be responsible for pain.3 4 This can make the diagnosis challenging, likely affecting the outcome of treatment. There is paucity of evidence-based treatment for this condition which makes it difficult to support currently used treatment recommendations.5 Further studies on pain mechanisms and randomised studies comparing treatment approaches are warranted to develop effective pathology-based treatment methods.
Recently, coexisting plantaris tendinopathy has been demonstrated in a subgroup of patients suffering from chronic painful mid-portion Achilles tendinopathy not responding to conservative treatments.6–10 Anatomical observations have shown that between individuals, there is a large variation in the course and insertion site of the plantaris tendon.11 The position of the plantaris in relation to the Achilles is of importance and can during certain movements lead to interference with compression and shearing between the Achilles and plantaris tendons.12 13 Surgical removal of the plantaris tendon has shown good short-term and longer-term clinical results,6 14–16 and also improved Achilles tendon structure.17 18 Furthermore, there is evidence that in some cases, only the plantaris tendon is abnormal suggesting that the plantaris tendon itself can be a driver of medial Achilles tendon pain.14 Therefore, a proper diagnosis including evaluation of plantaris tendon involvement is essential for choosing the correct treatment. Studies comparing clinical, surgical and imaging findings in patients with mid-portion Achilles tendinopathy have shown that plantaris tendon involvement is mostly characterised by medial tenderness, localised high blood flow between the plantaris and Achilles, and tendinopathic structural changes in the medial side of the Achilles.7
For chronic painful insertional Achilles tendinopathy there is, to the best of our knowledge, no study that has evaluated the position and impact of the plantaris tendon. In the region of the Achilles mid-portion, the plantaris tendon most often can be found using ultrasound (US) examination.7 However, in the Achilles insertion, the plantaris tendon is located very close to the medial Achilles and is often difficult to differentiate from the Achilles using conventional imaging such as US or MRI. This makes plantaris involvement difficult to diagnose, reinforcing the importance of distinct tenderness on the medial side of the Achilles insertion as the prime diagnostic finding. This observational case series aimed to evaluate plantaris tendon involvement in consecutive patients with chronic painful insertional Achilles tendinopathy. Medial side tenderness and preoperative US findings were compared with the surgical findings.
Methods
Patients
Ninety-nine consecutive patients (74 males and 25 females), mean age 40 years (range 24–64), who were surgically treated for chronic painful insertional Achilles tendinopathy by the same surgeon (HA) between 2013 and 2018, were included. All patients had prolonged pain symptoms (>6 months) from the Achilles tendon insertion. Participants were athletes in varied sports and activity levels: long-distance running (n=38), triathlon (n=3), football (n=3), rugby (n=2), basketball (n=2), recreational joggers (n=38) and walkers (n=13). None of the patients had an underlying inflammatory arthropathy or were on medication to control a chronic systemic inflammatory disease.
Clinical examination and US imaging
Clinical examination showed thickening of the Achilles tendon insertion with tenderness in the regions at the subcutaneous and retrocalcaneal bursa, and in some cases, distinct tenderness on the medial side of the Achilles insertion.
US+Doppler (DP) examination using a linear multifrequency probe (8–13 MHz, Siemens P500) showed a combination of pathology in the subcutaneous and retro-calcaneal bursa (thickening and high blood flow), bone (prominent bone edge-Haglund like deformity) and distal Achilles tendinopathy with high blood flow from the ventral side. In a subgroup of patients, a thick and wide plantaris tendon surrounded by high blood flow was visualised on the medial side of the Achilles tendon insertion.
Surgical procedure
Operations were performed with local anaesthesia (5–10 mL of Xylocaine 10 mg/mL with epinephrine 5 µg/mL). Via an open procedure, both bursae and the prominent upper calcaneus were removed together with scraping of the ventral side of the distal Achilles. The medial side of the insertion was then inspected. If a plantaris tendon was found (figure 1), it was released and the distal part (5–7 cm) of the plantaris tendon excised. The skin was sutured with non-resorbable sutures. Further details of this procedure and post-operative rehabilitation are described in a previous publication.19 Clinical examination, US examination and surgical procedures were performed by the same experienced surgeon (HA). The thickened plantaris tendon found at surgery was the surgeon’s subjective view.

Surgical removal of a thickened and widened plantaris tendon on the medial side of the Achilles insertion. The plantaris is identified proximally, released and followed all the way down to the insertion, where the tendon is divided.
All patients gave permission to be included in this study.
Results
In 48/99 patients (32 men, mean age 41 years, range 27–62; 16 women, mean age 38 years, range 27–59), there was distinct tenderness on the medial distal part of the Achilles tendon insertion on clinical examination.
In 32 patients, US+DP examination showed a plantaris tendon together with localised high blood flow on the medial side of the Achilles insertion.
Findings during surgical treatment showed a thick and wide plantaris tendon together with a richly vascularised fatty infiltration in 48/99 patients, in all patients with clinically diagnosed distinct medial tenderness.
Discussion
In this prospective observational study on patients surgically treated for chronic painful insertional Achilles tendinopathy, we found that the plantaris tendon appeared to be involved in almost half (48%) of the examined cases. This was indicated by the finding of a thick plantaris tendon together with richly vascularised fatty infiltration on the medial edge of the Achilles tendon insertion. These findings are likely of importance and should be considered for diagnosis and treatment especially when there is distinct medial tenderness during clinical examination.
It could be argued whether this finding is of clinical relevance. However, given the results of recent studies demonstrating comparably high neural innervation of the plantaris tendon and its surrounding tissues,9 it is likely that some cases of insertional Achilles pain will have plantaris tendon involvement as a component of pain generation. The plantaris tendon has been demonstrated to be stiffer and stronger than the Achilles tendon,20 and to have three different movement planes,12 all possibly predisposing to interference with the Achilles through compressive and shearing forces.13 Furthermore, a recent study has discovered that in some patients with mid-portion Achilles tendon pain, there is tendinopathy in the plantaris but not in the Achilles. This highlights the possibility that the plantaris and its surrounding tissues may indeed be a pain driver in patients with medial Achilles tenderness.14 The results of the current study show that for proper decision making on suitable treatments, the potential involvement of the plantaris tendon should be examined.
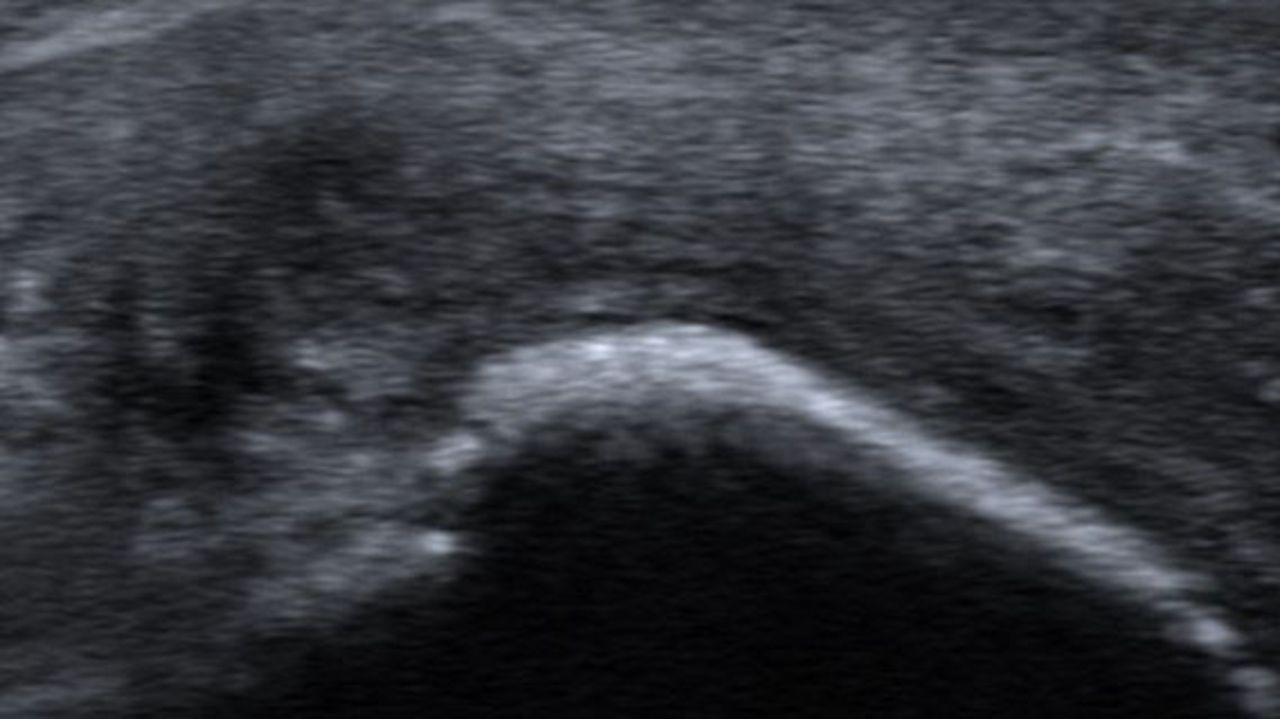
It is interesting that all 48/99 patients who had distinct tenderness on the medial side of the Achilles insertion on clinical examination, also had macroscopical findings of a thick plantaris tendon together with a richly vascularised fatty infiltration indicative of plantaris-related pathology. The preoperative US+DP scanning seems less reliable, as only 32/48 tendons with macroscopical findings were identified (figure 2.).
{kind=link}
{kind=link}
Ultrasound image showing a widened plantaris tendon (arrow) is seen on the medial side of the Achilles insertion.
A weakness in this study is that we have no histopathological evidence of plantaris tendon pathology. However, it seems likely that the pathological changes seen in the plantaris tendon at the level of the Achilles mid-portion would also occur at the Achilles insertion. Another weakness in this study is our inability to present the clinical results in all patients, as the majority of patients were sourced from other countries. Nevertheless, among the 48 tendons where the plantaris tendon was tender to palpation and subsequently removed during surgery, we had postoperative data on elite athletes. In this group, 23/23 were satisfied and had returned to previous sport activity, indicating that at least in this subgroup, it is likely that the plantaris tendon was involved in the painful condition. Finally, it is also a weakness that we can only subjectively evaluate the plantaris tendon as being thick and wide. This evaluation is based on the normal appearance of the plantaris tendon, as being thin like a ‘piano string’ and slightly flat in the insertion.
The results of this case series suggest that surgical excision of the distal part of the plantaris tendon represents a possible treatment strategy in patients with insertional Achilles tendinopathy and distinct medial tenderness. However, randomised studies on larger patient material, with and without plantaris removal, are needed to clarify the role of the plantaris tendon in chronic painful insertional Achilles tendinopathy.
In conclusion, in patients with chronic painful insertional Achilles tendinopathy with distinct tenderness on the medial side of the insertion, the plantaris tendon should be considered as a possible source for pain.
References
Footnotes
Twitter @lorenzo_masci
Contributors HA performed all the surgeries and clinical examinations. CS was involved in the data processing. LM was involved in clinical examination and ultrasound imaging. All authors were involved in the design of the study, the data collection and manuscript writing. The manuscript was finally approved by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Studies on surgical treatment of Achilles tendinopathy were approved by a local ethics committee (Umea University, Sweden).
Provenance and peer review Not commissioned; externally peer reviewed.