Article Text

Abstract
Background Studded footwear can cause severe lacerations in rugby union; the prevalence of these injuries is currently unknown.
Objective To summarise the skin and laceration injury prevalence in published epidemiological studies and to investigate any differences in skin injury risk between amateur and professional players.
Design Systematic literature review and meta-analysis of epidemiological studies.
Data sources PubMed, Web of Science, Scopus and Ovid.
Eligibility criteria for selecting studies Prospective, epidemiological studies published in English after 1995, measuring a minimum of 400 match or 900 training exposure hours. Participants should be adult rugby union players (amateur or professional). The study should report a separate skin or laceration injury category and provide sufficient detail to calculate injury prevalence within this category.
Results Twelve studies were included. Mean skin injury prevalence during matches was 2.4 injuries per 1000 exposure hours; during training sessions, the prevalence was 0.06 injuries per 1000 exposure hours. Skin injuries accounted for 5.3% of match injuries and 1.7% of training injuries. Skin injury risk was similar for amateur compared with professional players during matches (OR: 0.63, p=0.46.), but higher during training sessions (OR: 9.24, p=0.02).
Conclusions The skin injury prevalence of 2.4 injuries per 1000 exposure hours is equivalent to one time-loss injury sustained during matches per team, per season. Amateur players are more likely to sustain skin injuries during training sessions than professional players. There is a need for more studies observing injuries among amateur players.
Trial registration number PROSPERO CRD42015024027.
- Epidemiology
- Injury
- Rugby
- Dermatology
- Review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What are the new findings
Skin injuries account for 5.1% of match injuries and 1.5% of training injuries in rugby union.
Amateur players are more likely to sustain a laceration injury during training sessions than professional players.
Current injury definitions can lead to underestimation of skin and laceration injury prevalence.
Future studies should focus on investigating amateur and female rugby skin injuries.
What is already known?
Injury prevalence in professional rugby union is 81 injuries per 1000 match exposure hours.
Laceration and skin injury prevalence in professional rugby union is 1–3 injuries per 1000 match exposure hours.
Injury definitions influence the reporting of overall injury prevalence; this makes it difficult to compare different studies.
Introduction
Rugby union is a popular sport with approximately 7.23 million players worldwide.1 Rugby union has a high injury incidence with a self-reported injury rate of 96 injuries per 1000 occasions of participation. This is higher than other popular team sports such as association football (64 injuries per 1000 occasions) and field hockey (62 injuries per 1000 occasions).2 The full-contact nature of rugby union has previously been identified as a major risk factor for injury; an estimated 72% of match injuries resulted from player-to-player contact.3
Studded footwear is worn in rugby union and other field sports played on grass, as a means to increase the traction between the shoe and the playing surface. Studs have been shown to cause severe laceration injuries to players.4 In 2008, a studded footwear manufacturer was sued by a player who sustained a laceration to the head.5 Since the introduction of the bladed stud in 1994, manufacturers have made innovations in the design and material of studded footwear. Traditionally, rugby boots have been equipped with screw-in studs with a round profile, made out of aluminium. Bladed studs are moulded out of plastic, and their elongated profile gives rise to their name. Nowadays, rugby players wear both shoes with moulded studs and with aluminium rounded studs.6 World Rugby, the international governing body of rugby, has specified a test method for assessing the laceration injury risk of studded footwear; however, these regulations currently lack validation and are optional for manufacturers to follow. Identifying the proportion and prevalence of skin injuries in rugby union will aid the understanding of skin injuries and is the first step in injury prevention models such as van Mechelen et al.7 Previously, there have been no specific published data available on the skin injury prevalence caused by stud–skin interactions in rugby union.
In rugby union, a survey study6 investigating the cause of stud laceration injuries during the game identified that 97% of respondents had experienced minor (ie, did not hinder the player from continuing to play) skin injuries caused by studs and 71% of respondents had experienced major (ie, lost playing time) skin injuries caused by studs at least once during their rugby career. No stud laceration injury incidence (ie, injuries per 1000 exposure hours (ITEH)) was reported in this study.
The injury definition used in sports injury epidemiological studies influences their results and has been a topic of debate.8–10 Five commonly used injury definitions are:
Time-loss (1 day): any physical complaint sustained by a player during a match or training session that prevents the player from taking full part in a match or training session 1 day after the injury.10
Time-loss (immediate): any physical complaint sustained by a player during a match or training session that forces the player to retire and/or prevents the player from taking full part in a training session or match the following day.
Medical attention: the player receives medical treatment for his/her injury.
Player reported: the player reports his/her physical complaint as an injury.
Trainer reported: the coach or (head) trainer reports a player injured.
A consensus statement on injury definitions and data collection procedures for epidemiological studies in rugby union was published in 2007.10 This document recommends using the 1-day time-loss injury definition and laceration injuries are recommended to have their own injury type category. If a time-loss injury definition is used, minor injuries and injuries which fall under the blood injury rule11 could be treated on the side of the field (stitched or glued) and therefore be ignored in the injury count, leading to a likely underestimation of the skin injury prevalence.12 13 An example of such a situation is given in the consensus statement,10 p330:
‘A loose-head prop forward sustained a laceration to his head during a match; the player left the field of play to enable the team doctor to suture and protect the injury. The player returned to the field of play. The player continued to train and play with his head bandaged for the next three weeks. This episode should not be recorded as an injury’.
In a review on skin injuries in football, van den Eijnde et al 12 warned that skin injuries were under-reported in the current literature and suggested that this resulted from restrictive injury definitions. The use of a medical attention injury definition rather than a time-loss injury definition led to a twofold to fourfold increase in the injury prevalence of abrasions and lacerations compared with the use of a time-loss injury definition.12
Level of play has previously been identified as a risk factor for injury.14 In a meta-analysis of professional rugby union injuries by Williams et al, 15 international match injury risk was found to be higher than levels 1 and 2 clubs match injury risk, suggesting that more elite players sustain a higher risk of injury during matches. This effect was not found for training injuries. Overall, mean match injury prevalence during senior men’s professional rugby was 81 ITEH and mean training injury prevalence was 3 ITEH.15 This same review also investigated injury patterns in professional rugby union; they found a laceration and skin injury prevalence during match play of 1 ITEH (95% CI 1 to 3 ITEH).15 The review did not report on the proportion of laceration and skin injuries, the laceration injury prevalence during training sessions, and solely focused on injuries sustained by professional players. Therefore, no comparisons could be made between injury risks for amateur versus professional players. Differences between professional and amateur rugby could influence the skin and laceration injury prevalence between playing levels.
These differences include playing styles, the quality and potential wear of the footwear worn, intensity of movements and impact forces. This study systematically reviews published epidemiological literature reporting on laceration or skin injury prevalence in rugby union during match play and training sessions and identifies potential differences in skin injury risk for amateur and professional players.
Methods
This review was registered in the PROSPERO International Prospective Register of Systematic Reviews (registration number CRD42015024027). The 2009 Preferred Reporting Items for Systematic review and Meta-Analysis Protocols guidelines for preferred reporting items for review and meta-analysis protocols16 were implemented in preparing and conducting this review.
Literature search strategy
The literature search was conducted in July 2016 using the search engines PubMed, Ovid, Scopus and Web of Science. The search strategy was designed with the purpose of finding epidemiological studies on rugby union injuries. Search terms for all search engines were:
(rugby) AND (epidemiology OR epidemiological OR epidemiologic OR injury OR injured OR injuries).
Search engine limits were set to find only articles published after January 1995, due to an innovative change in stud design in the previous year (1994) and the introduction of professional rugby union in 1995. The title, author, date of publication and abstract of each record were imported to a Reference Manager (RefWorks, ProQuest LLC, 2016).
Selection criteria
After removing duplicates, the title and abstract of the remaining records were screened for eligibility by the first author. From resulting records, the full-text article was obtained and again screened for eligibility. The following inclusion criteria were used throughout:
The study must report on prospective, epidemiological findings in a rugby union cohort of players.
The study must observe injuries in players >18 years of age.
The study must not report only a subcategory of injuries, for example, tackling injuries or head injuries.
The study must report a skin or laceration injury category and provide enough information to calculate injury prevalence within this category.
The athlete exposure in the study should be >400 match hours and/or 900 training hours.
The full-text article must be written in English and published in a peer-reviewed journal after 1995.
Only studies observing injuries in an adult cohort were included in this review since in junior (<18 years) age categories, the rules of rugby union are different. The minimum athlete exposure criteria was defined such that at least one team (15 players) was followed for a full season (defined as 20 matches and/or 20 weeks of 2 training sessions a week), which results in a minimum of 400 match exposure hours or 900 training exposure hours. Studies published after 1995 were included because a change in stud designs was introduced in 1994 and professionalism was introduced in rugby union in 1995. No restriction was placed on the level of play (amateur or professional), sex or injury definition used. Athletes were defined as ‘professional’ if they were receiving monetary reimbursement for their participation in the team to the degree that maintaining full-time employment elsewhere was not necessary. Review papers, conference abstracts and studies using data that were already published in a different study were excluded. A study was also excluded if it did not report injury frequency and exposure hours for match and training sessions separately.
Quality and bias assessment
A four-item checklist was used to assess the risk of bias of each of the included studies. The checklist was adapted from Waldén et al 17 and based on the ‘Strengthening the reporting of observational studies in epidemiology’ (STROBE) statement.18 Studies were assessed on each item for low risk (0) or high risk (1) of bias. A cumulative score for each study was calculated. Studies with a cumulative score of 0 were defined as at low risk of bias, studies with a score of 1 or 2 as at medium risk of bias and studies with a score >3 as at high risk of bias. Only studies with a low or medium risk of bias were included in the meta-analysis. The full checklist can be found in online supplementary material 1.
Supplementary Material
Supplementary material 1Data extraction
For each study that met the inclusion criteria, the injury definition, skin injury category and athlete level—professional or amateur—were recorded. Where available, the observed number of total injuries, the observed number of skin or laceration injuries, and their corresponding match and training exposure hours were extracted from each study. Injury prevalence was defined as the number of observed ITEH. For each study, separate injury prevalence (±95% CI) was calculated for injuries sustained during match play and during training sessions. The percentage of skin injuries in proportion to total injuries observed in a study was also calculated for both matches and training sessions. If stated in a separate category, abrasion injuries were not included when calculating skin injury prevalence. A weighting factor based on study size (defined as exposure hours) was implemented when calculating the mean of each group of studies.
Statistical analysis
In this meta-analysis, the influence of playing level (amateur or professional) on skin injury prevalence during match and training sessions was of interest. Influence of sex on injury risk could not be investigated due to a shortage of studies publishing female injury numbers. Skin injury prevalence data was modelled using a negative bionomial regression with log link. This generalised linear model is similar to the Poisson regression model previously described by Lystad et al,19 but also accounts for overdispersion in the dataset. In our model, the response variable was the number of observed skin injuries offset by the log of the exposure hours. A weight scaling variable was assigned to each study depending on its relative size. The OR (and 95% CI) that an amateur player sustains a skin injury—as compared with a professional player—was calculated. Separate ORs were determined for training sessions and during match play. Alpha was set at 0.05.
Results
A total of 1351 records were identified through the online search engines (stage 1, figure 1). After duplicates were removed, the titles and abstracts of 464 remaining records were screened (stage 2). The screening excluded 424 articles; therefore, 40 full-text articles were reviewed for eligibility (stage 3). Twenty-eight articles were excluded based on the selection criteria, leaving 12 studies which were included in this review3 20–30 (stage 4). Out of these selected studies, 10 studies measured professional athletes3 20 22–28 30 and 2 studies observed injuries in an amateur cohort.21 29 Eleven out of 12 studies included a completely male cohort3 20 22–30; 1 study observed injuries of both males and female rugby players.21
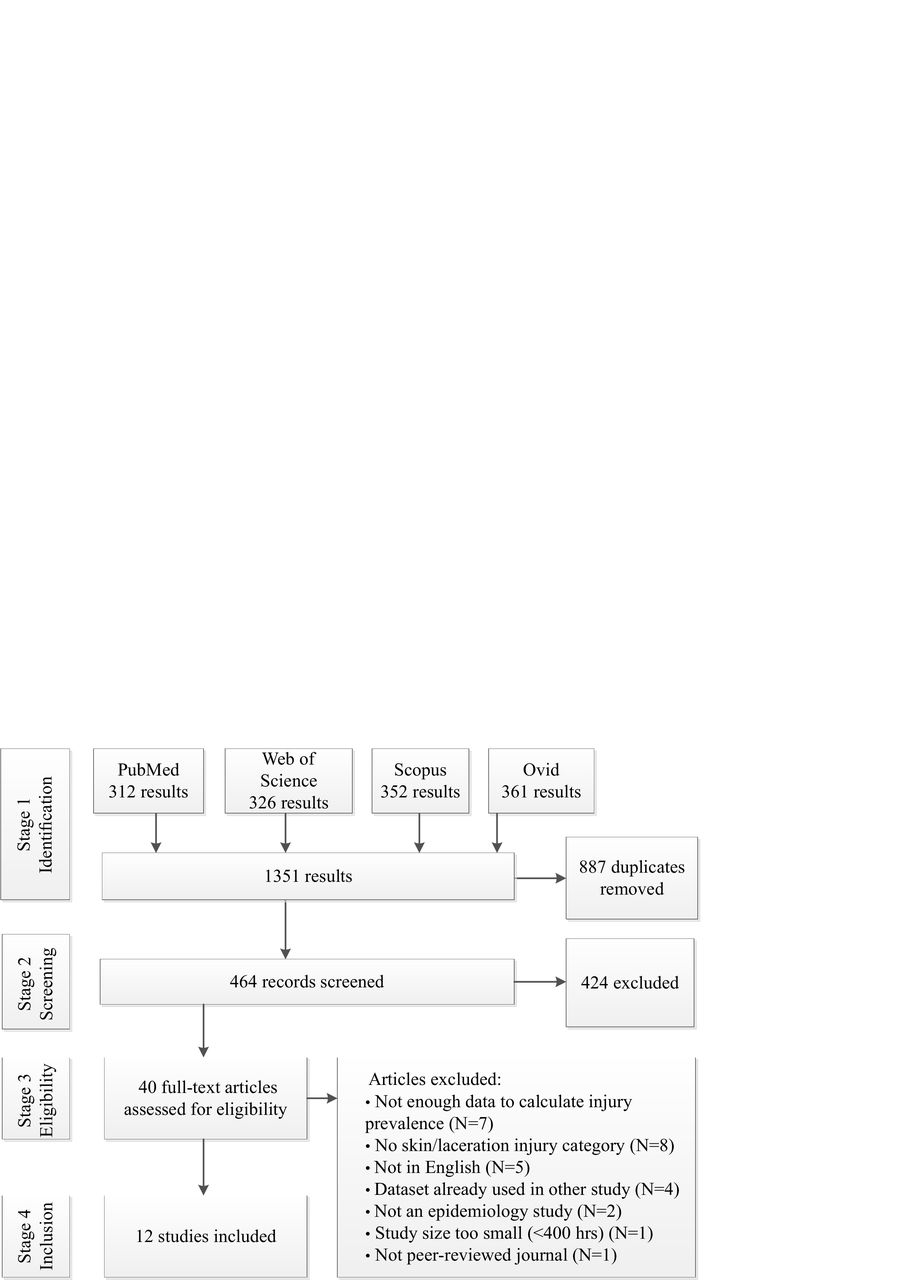
Flow chart of the literature search and selection process. Chart design adapted from Moher et al.16
Quality and bias assessment
In the risk of bias assessment, seven articles were categorised as a low risk of bias and five articles were categorised as a medium risk of bias (online supplementary material 1). No articles were excluded from the meta-analysis based on the bias assessment.
Match injuries
Eleven out of 12 studies included in this review monitored and reported the match injuries of their athletes3 20 21 23–30 (table 1). The majority of the studies3 22–27 29 30 used a time-loss 1 day injury definition. The other studies used time-loss immediate, sometimes in combination with medical attention. 20 21 28 No included study used a player or coach reported definition. Mean overall match injury prevalence in professional and amateur players combined was 53 ITEH (95% CI 51 to 54).
Total and skin injury prevalence of rugby union players during matches
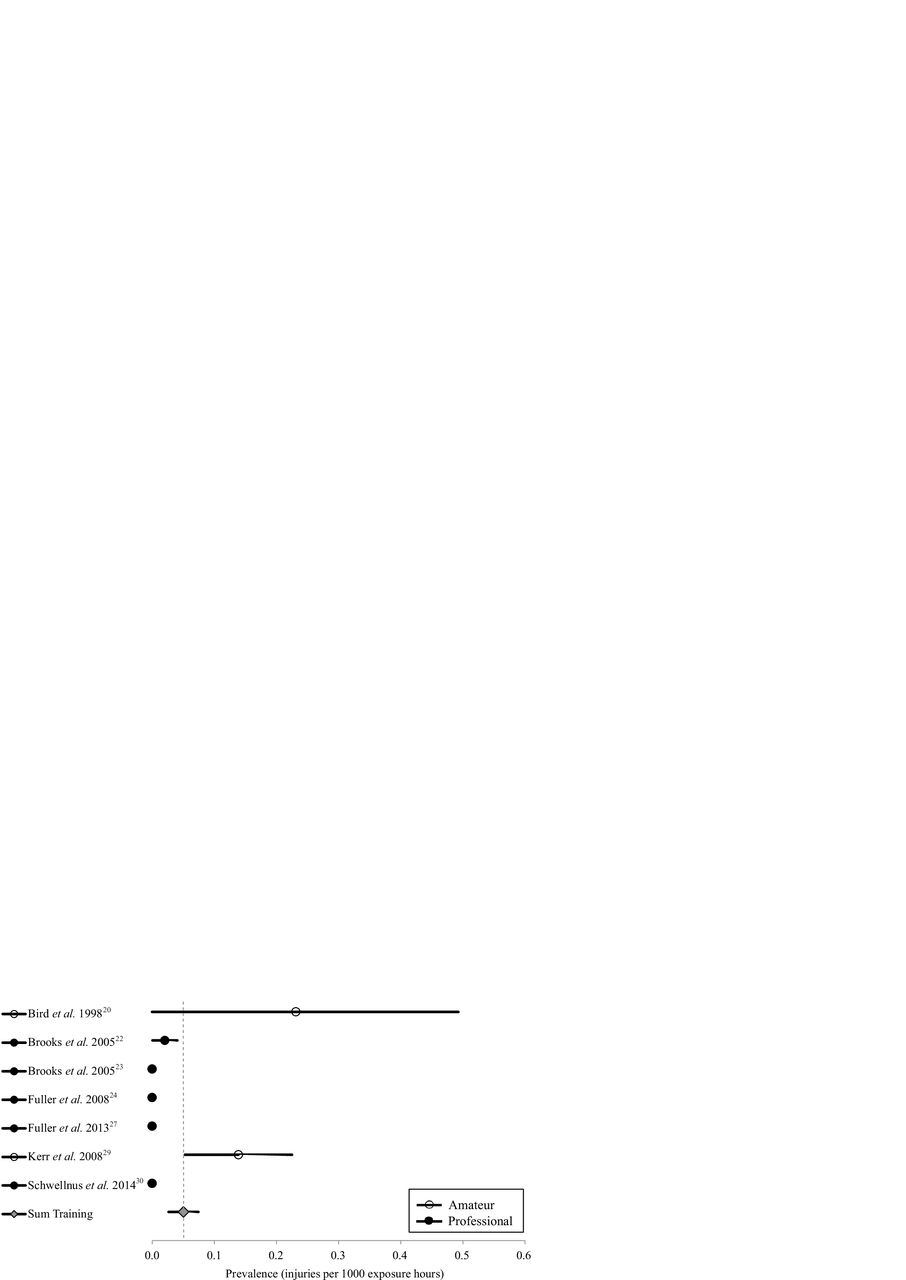
The skin injury prevalence during match play in amateur and professional players combined was 2.4 ITEH (95% CI 2.0 to 2.7) (figure 2). Mean skin injury prevalence during professional match play was 3.0 ITEH (95% CI 2.5 to 3.6) and during amateur match play was 1.8 ITEH (95% CI 1.4 to 2.2). The skin injury risk for amateur players compared with professional players during matches was not significantly different (OR: 0.60; 95% CI 0.17 to 2.08; p=0.42). The lowest skin injury prevalence observed was 0 laceration injuries after 19:20 hours of match exposure.24 The highest skin injury prevalence was 21.2 ITEH, where 41 injuries occurred during 19:30 hours of match play.20 The proportion of skin and laceration injuries in the included studies during match play ranged from 0% to 27%, with a weighted mean of 5.1%.

Forest plot of skin injury prevalence during match play in studies observing amateur and professional injuries.
Training injuries
Seven out of 12 studies included in this review monitored and reported the injury data of their athletes during training sessions.21–24 27 29 30 Five studies monitored a professional population,22–24 27 30 and two studies an amateur population.21 29 One study used the time-loss immediate in combination with medical attention injury definition,21while the other six studies used the time-loss 1 day injury definition23 24 27 29–31 (table 2). The mean overall training injury prevalence for amateur and professional players combined was 2.8 ITEH (95% CI 2.6 to 2.9).
Total and skin injury prevalence of rugby union players during training sessions
Mean skin injury prevalence during training sessions of amateur and professional players combined was 0.05 ITEH (95% CI 0.02 to 0.07) (figure 3). Skin injury prevalence during training sessions in professional players was 0.02 ITEH (95% CI 0.00 to 0.03) and in amateur players 0.15 ITEH (95% CI 0.07 to 0.24). There was a significantly higher risk of skin injuries for amateur players compared with professional players during training sessions (OR: 7.92; 95% CI 1.19 to 52.78; p=0.03). Four out of seven studies23 24 27 30 reported that no laceration injuries were observed during training sessions. The proportion of skin and laceration injuries during training sessions ranged from 0% to 4.5%, with a weighted mean of 1.5%.

{kind=link}
{kind=link}
{kind=link}
Forest plot of skin injury prevalence during training sessions in studies observing amateur and professional injuries.
Discussion
The objective of this review was to identify the prevalence of skin injuries in rugby union during match play and training sessions and to investigate if the risk of injury differs between amateur and professional players. The skin injury prevalence during match play from the combined data of 11 studies observing rugby union players was 2.4 ITEH, accounting for 5.1% of all match injuries. This number could be interpreted as one time-loss or medical attention laceration injury per team (15 players) per year (20 matches, 80 min/match). Seven of the included studies in this review provided sufficient information to calculate skin and laceration injury prevalence during training sessions. Mean skin injury prevalence during training sessions was 0.05 ITEH, accounting for 1.5% of all training injuries. Injury prevalence has previously been found to be lower during training sessions than in match play,3 22 27 and in this review a similar trend is observed when measuring skin injury prevalence (training: 0.05 ITEH; matches: 2.4 ITEH). In comparison, the incidence of abrasion and laceration injuries in association football matches—systematically summarised by van den Eijnde et al 12—varied from 0.8 to 6.1 ITEH.
Ten out of 12 studies included in this review reported on professional rugby union injuries. No difference was found in skin injury risk during match play for amateur players compared with professional players (OR: 0.60; 95% CI 0.17 to 2.08; p=0.42). During training sessions, the risk of skin injuries was higher for amateur players than for professional players (OR: 7.9; 95% CI 1.2 to 52.8; p=0.03). Only two studies included in this review reported on amateur injuries,21 29 from which one used a time-loss immediate in combination with a medical attention injury definition.21 The injury definition could therefore have influenced this result. Williams et al 15 found no clear influence of playing level on injury risk during training sessions, though more elite levels of play were associated with a higher injury likelihood during matches (87%–100% likelihood). The conclusions of Williams et al 15 were based on various levels of professional rugby (club level 2 to international), which makes it is unclear if this trend could be extrapolated to injuries sustained in amateur rugby as well. The impact of professionalism on injuries has previously been investigated by Garraway et al 14 who concluded that professionalisation in rugby union had increased the prevalence of injuries in both amateur and professional cohorts. Financial rewards were suggested to raise the overall injury rate and increase the pressure on athletes to return to play as soon as possible, making recurrent injuries more likely. The lower risk of skin injuries found in professional players could indicate that this type of injury is frequently ignored in professional rugby injury counts, therefore underestimating the extent of the injury problem.12 13 Approximately one-third of amateur rugby union players have found their own studs sharpened due to wear.6 In professional rugby union, players are more likely to have thorough stud checks and are more likely to renew their footwear or studs frequently, therefore minimising the usage of damaged studs resulting from wear.
All studies included in this review used a ‘time-loss’ injury definition. Four studies used the ‘time-loss immediate’ definition and these studies had the highest percentage of laceration injuries of the 12 studies, suggesting that this type of injury often forces a player off the field, but not necessarily prevents them from playing subsequent matches. A consensus statement on the injury definitions used in epidemiological studies for rugby union recommends the use of time-loss 1 day injury definitions.10 Before the publication of this consensus statement, Ekstrand et al 32 warned that the use of time-loss injury definitions can lead to underestimation of the true prevalence of skin injuries. An example is given by Gibbs13 who observed 62 lacerations which needed suturing during three rugby league seasons. One of these lacerations was officially marked as an injury because the wound became infected which resulted in missed training sessions and/or matches for the injured player. This situation reiterates the importance of appropriate injury definitions when estimating the skin injury risk of players; the medical attention injury definition is less likely to underestimate skin injury prevalence compared with 1 day time-loss definition.12
Limitations
The results of this study should be interpreted in the light of its limitations. As skin and laceration injuries are rarely the focus of epidemiological studies of sports injuries, a more accurate estimate of skin injury prevalence could have been obtained if more studies were included; specifically, eight studies were excluded from this review because no separate skin or laceration injury category was available in the published article. Excluding articles that did not state a separate skin or laceration injury category could have biased the results if authors decided not to report this injury category because the injury frequency was too low. Any observed skin injuries would therefore be masked in the ‘other’ injury category. However, Fuller et al 24 still included a laceration injury category even though no lacerations were observed in the study. Four out of the seven studies reporting on training injuries also found no lacerations or skin injuries during training sessions in the observed time period, but still included the injury type as a separate category.23 24 27 30 According to the consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union,10 it is recommended that studies should report both separate laceration and abrasion injury categories. This is reiterated by van den Eijnde et al 12 who recommends reporting of contusions, lacerations and abrasions as separate injury categories as the causes of the injuries and the consequences for the athlete differ between these categories. The consensus statement on the collecting and reporting of epidemiological data had not been adopted by all studies in this review, often because studies were carried out before the statement was published. If future studies adopt these guidelines on reporting of injury categories, comparability between studies should improve. This increased standard in reporting can aid the validity of collated injury information across a number of studies and should encourage the reporting of ‘null-results’, where no injury in a specific category was observed.
A generalised linear model with negative binomial distribution with log link was used for the statistical analysis. As the data showed overdispersion, it was not possible to apply a Poisson distribution as previously described.15 19 Using a negative binomial distribution has lowered the statistical power, therefore making a conservative estimate of the effect of the predictor on the outcome variable. For that reason, it could be that there is an effect of playing level on skin injury risk during matches (figure 2) but more studies are needed to confirm or negate this.
Future research
There are a disproportionally small number of studies observing injuries in amateur cohorts. With <1% of all rugby union players receiving enough monetary reimbursement to focus on rugby full-time, professional players are over-represented in published epidemiological studies. As injury trends are not necessarily transferable between playing levels, an increase in studies observing amateur injury trends is needed. Furthermore, in this meta-analysis, the risk of bias in the two studies observing injuries in an amateur cohort21 29 was also higher than in the studies observing professional players3 20 22–28 30 (supplementary material 1). Therefore, future research should focus on establishing relevant skin injury frequencies in amateur cohorts, through equally robust methods as those applied to professional cohorts.
The female rugby population was under-represented in this review. One previous study found differences in injury patterns between male and female intercollegiate rugby players,33 but skin injuries were not investigated. The studies identified in this meta-analysis did not include enough female participants to determine whether gender had an influence on skin injury risk. Due to increasing women’s participation in the game,34 focus should be given to document female rugby injuries.
In future, incidence and severity of laceration injuries could be assessed with a modified version of the Skin Damage and Severity index which was originally developed for assessing abrasive injuries in football.35 This would allow for a more accurate estimation of the laceration injury prevalence in rugby union, minimising the non-reporting of these injuries caused by current injury definitions.
Conclusion
This systematic review summarised the published epidemiological literature on laceration or skin injury prevalence in rugby union. Following the inclusion criteria, 12 studies were selected for meta-analysis. Overall, skin and laceration injuries accounted for 5.1% of match injuries and 1.5% of training injuries in rugby union. A mean injury prevalence of 2.4 skin or laceration injuries per 1000 match exposure hours was found in this study, which could be interpreted as one time-loss injury per team, per season. During match play, no difference in skin and laceration injury risk was found between amateur and professional players. In training sessions, amateur players had a higher risk of sustaining skin and laceration injuries than professional players. Future research should focus on high-quality studies observing amateur players, female athletes and potentially developing a tool for assessing acute skin injury damage in rugby union.
References
Footnotes
Contributors BYO designed the study, collected the data, organised the data, performed the statistical analysis and drafted and revised the paper. She is guarantor. HFD and DJ monitored the data collection and data analysis and revised the draft paper. KK selected the statistical methods and revised the draft paper. MD revised the draft paper.
Funding This project was internally funded.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.