Article Text

Abstract
Background Spinal manipulation is commonly used to treat back pain. The application of spinal manipulation has traditionally involved an element of targeting the technique to a level of the spine where the proposed movement dysfunction is sited. We evaluated the effects of a targeted manipulative thrust versus a thrust applied generally to the lumbar region.
Methods A randomised controlled clinical trial in patients with low back pain following CONSORT (Consolidated Standards of Reporting Trials) guidelines. Sixty subjects were randomly allocated to two groups: one group received a targeted manipulative thrust (n=29) and the other a general manipulation thrust (GT) (n=31) to the lumbar spine. Thrust was either localised to a clinician-defined symptomatic spinal level or an equal force was applied through the whole lumbosacral region. We measured pressure-pain thresholds (PPTs) using algometry and muscle activity (magnitude of stretch reflex) via surface electromyography. Numerical ratings of pain and Oswestry Disability Index scores were collected.
Results Repeated measures of analysis of covariance revealed no between-group differences in self-reported pain or PPT for any of the muscles studied.
Summary A GT procedure—applied without any specific targeting—was as effective in reducing participants’ pain scores as targeted approaches.
Trial registration number ISRCTN11994230.
- back injuries
- physiotherapy
- sports physiotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings?
A technically difficult targeted manipulation technique that requires specific training was no more effective in reducing back pain than a simple general thrust technique, which requires minimal training.
How might it impact on clinical practice in the future?
Our data challenge the time-consuming examination and treatment techniques that target a thrust technique to a specific region of the lumbar spine for back pain, when in our study the specific techniques proved no better than a simple, general thrust technique.
Introduction
Low back pain is extremely common, with at any point in time, approximately 12% of the global population suffering from significant levels of pain.1 Within the sporting population, low back pain is one of the more common musculoskeletal conditions affecting athletes.2 In a review of national and international guidelines, for the management of non-specific back pain in primary care, 12 out of 15 guidelines included manipulation as a recommendation for the management of non-specific low back pain.3 Spinal manipulation (SM) is defined as ‘the application of rapid movement to vertebral segments producing joint surface separation, transient sensory afferent input and reduction in perception of pain. Joint surface separation will commonly result in intra-articular cavitation, which in turn, is commonly accompanied with an audible pop. Postmanipulation reductions in pain perception are influenced by supraspinal mechanisms including expectation of benefit’.4
Manual therapists invest considerable time and effort developing psychomotor skills and clinical reasoning paradigms, based on the identification and targeting of specific passive movements to a symptomatic spinal level. However, some authors have shown clinically meaningful reductions in spinal pain, with SM techniques that move a large regions of the spine, with very little targeting of movement.5 Also, neck pain can be reduced with SM applied to the thoracic spine.6
Researchers have investigated the efficacy of the specificity of application that has also been considered with both high (mobilisation) and low velocity (manipulation) passive movements applied to the spine. Two studies7 8 compared the effects of specific manipulation and mobilisation with a clinician-determined ‘target’ spinal level, with manipulation/mobilisation applied at random levels or generally through the lumbar spine. Pain and disability were equally improved—further challenging the need for targeting passive movement. Those two studies7 8 had not examined the effects of SM on electromyography (EMG) parameters and had not standardised the amplitude of the SM movements used.
We believed there was a need to investigate the clinical utility of specific targeting thrust (TT) versus a general thrust (GT) movement SM (of equivocal acceleration). Therefore, this study examined the effect of targeting SM to symptomatic lumbar spinal level on (1) local nociceptive pain, (2) self-reported back pain and (3) local muscle stretch-reflex responses. The intervention was compared with a thrust movement of the same magnitude and acceleration that did not target a spinal level, instead generally moving the lumbar region. We noted that the magnitude of the local-muscle EMG stretch-reflex response to manipulative techniques may be correlated with the severity of pain and disability in patients with low back pain,9 and that the local stretch-reflex response contributes to postreflex relaxation of muscle,10 thereby contributing to the analgesic effect of SM. Therefore, our study included data that would allow us to compare this local muscle response, between the targeted thrust (TT) and GT groups.
Methods
Subjects were randomly allocated to either a TT or GT group, using a minimisation technique.11 The Minimisation strategy employed two factors: body mass index and gender to govern allocation, as these factors are known to influence EMG signal conduction velocity.12 Subjects were blind to treatment allocation.
Participants
Subjects, with low back pain, were recruited. On the initial visit, participants were screened for eligibility including: being between 20 and 60 years of age, having suffered pain for at least 3 weeks, having a Roland Morris Disability Questionnaire (RMDQ)13 score of 4 or above and not having any previous history of significant illness, bony pathology or any other contraindications to manipulation (ie, red flags). The study was approved by a local research ethics committee. Research carried out with human subjects in compliance with the Declaration of Helsinki. The study was approved by a local research ethics committee (North Manchester LREC 02/NM/406).
Patient involvement
The research was developed using the views of patients involved in an evaluation of back care services in a local hospital and reflected their desire to understand the need for such a long and detailed assessment process, prior to treatment. Results were fed back via the clinical department at which the service was being undertaken. Being involved in the study did not involve significantly more time or inconvenience than routine clinical care at the local service.
Intervention
Participants had been informed that they would receive one of two types of SM technique and were blind to which type they were receiving. The clinician, undertaking the SM technique, was not blind to allocation. The TT group received a single high-velocity low-amplitude thrust delivered to the subject positioned in a side lying position. The manipulation was delivered by an osteopath with 13 years of clinical experience. The joint targeted for manipulative thrust was the spinal location deemed to be most symptomatic during the clinical examination, using active movement observation, passive movement assessment of resistance to movement and pain provocation tests.14 The process of identifying the spinal level, considered clinically relevant, and thus the target for the manipulative thrust technique was investigated in a reliability study prior to the initiation of this work.14 This work established the intrarater reliability of this judgement to be Intraclass Correlation Coefficient (ICC)2,1=0.96 (95% CI 0.87 to 0.99).
The GT group received a high velocity movement with the subject in the same position as the targeted manipulation, but the force of the thrust was not directed toward a specific lumbar level. It was hypothesised that this would create a similar stimulation of the mechanoreceptors in the superficial soft tissues but that the kinetic force would be dispersed across a wider area causing less stimulation to specific, intersegmental joint and muscle mechanoreceptors. Subjects attended for three replicate sessions, with a minimum of 7 days and maximum of 9 days interval between visits. The intervention was undertaken in a clinical research facility, sited within a university teaching hospital.
Outcome assessment
Subjects attended for three sessions, where they received the intervention determined at allocation. At each testing session, subjects completed a RMDQ, in addition to the outcome measurements, detailed below.13
Pain measurements
Pretreatment and post-treatment pain were assessed by 15 16 Visual Analogue Scale and algometry. Algometry was used to assess pressure-pain threshold (PPT) at the centre of the muscle belly, for the same muscles evaluated by EMG (local multifidus and illiocostalis) (model PTH-AF 2; Pain Diagnostic and Treatment, USA). The reliability of this measure had been established as very good (ICC2,1=0.87; 95% CI 0.67 to 0.95), with low measurement error in a study undertaken prior to the trial.17
Electromyography
Surface EMG (sEMG; Biopac Systems, MP150 WSW, California, USA) was employed to assess peak EMG amplitude as a measure of muscular reflexogenic responses. Disposable pregelled, self-adhesive, surface electrodes (Ag/AgCl, Unilect), were attached bilaterally to prepared skin (impedance <10 kΩ), overlying two pairs of muscles: local multifidus and iliocostalis. Further electrodes were placed on bony prominences to act as ground electrodes.
Recorded signals were low and high bandpass filtered to exclude <8 Hz and >500 Hz, notch filtered (50 Hz) to remove ambient electric noise, and A to D converted at a sampling rate of 1000 Hz. AcqKnowledge software (Biopac Systems) was used for data extraction. Filtered raw EMG signals were normalised by subtracting the peak-to-peak EMG measurement at rest in side lying from the peak-to-peak recording of the reflex responses for each channel. Normalisation allowed for the comparison of the same muscle/different muscles on different days.18 An accelerometer (triaxial accelerometer TSD109F; Biopac Systems, California, USA), placed on the iliac crest, was used to evaluate the rate of acceleration and magnitude of the thrust for both groups.
Data analysis
We used an analgesic effect size of measures using self-reported pain (η2=0.25), a two-tailed null hypothesis and an alpha of 0.05 to generate a conservative estimate of power. Thirty participants per treatment group were determined to provide greater than 95% power to detect a group × time interaction in the proposed analysis of variance (ANOVA) model, based on pilot study point estimates of group difference and pooled SD.
All data were normally distributed and all assumptions for parametric testing were met. A repeated measure analysis of covariance (ANCOVA) (baseline scores as a covariate) was conducted to evaluate the differences in, change of pain and disability and differences between the magnitude of the EMG reflex response to TT and GT at the three different time points for the two groups. A priori, a decision was made to undertake per-protocol analysis and compare this with intention-to-treat analysis (using last value carried forward imputation of missing data) if loss to follow-up was >20%.
Results
Participants
Seventy-six subjects attended for assessment. Fourteen of these volunteers were excluded (these participants had a RMDQ score that was too low (<4) for inclusion) and one declined to participate. Sixty-one were allocated and one withdrew after randomisation. Thus, from a sample of 60, 31 subjects were allocated to the TT group and 29 to the GT group. Loss to follow-up after visit 3 was 15% (see figure 1).
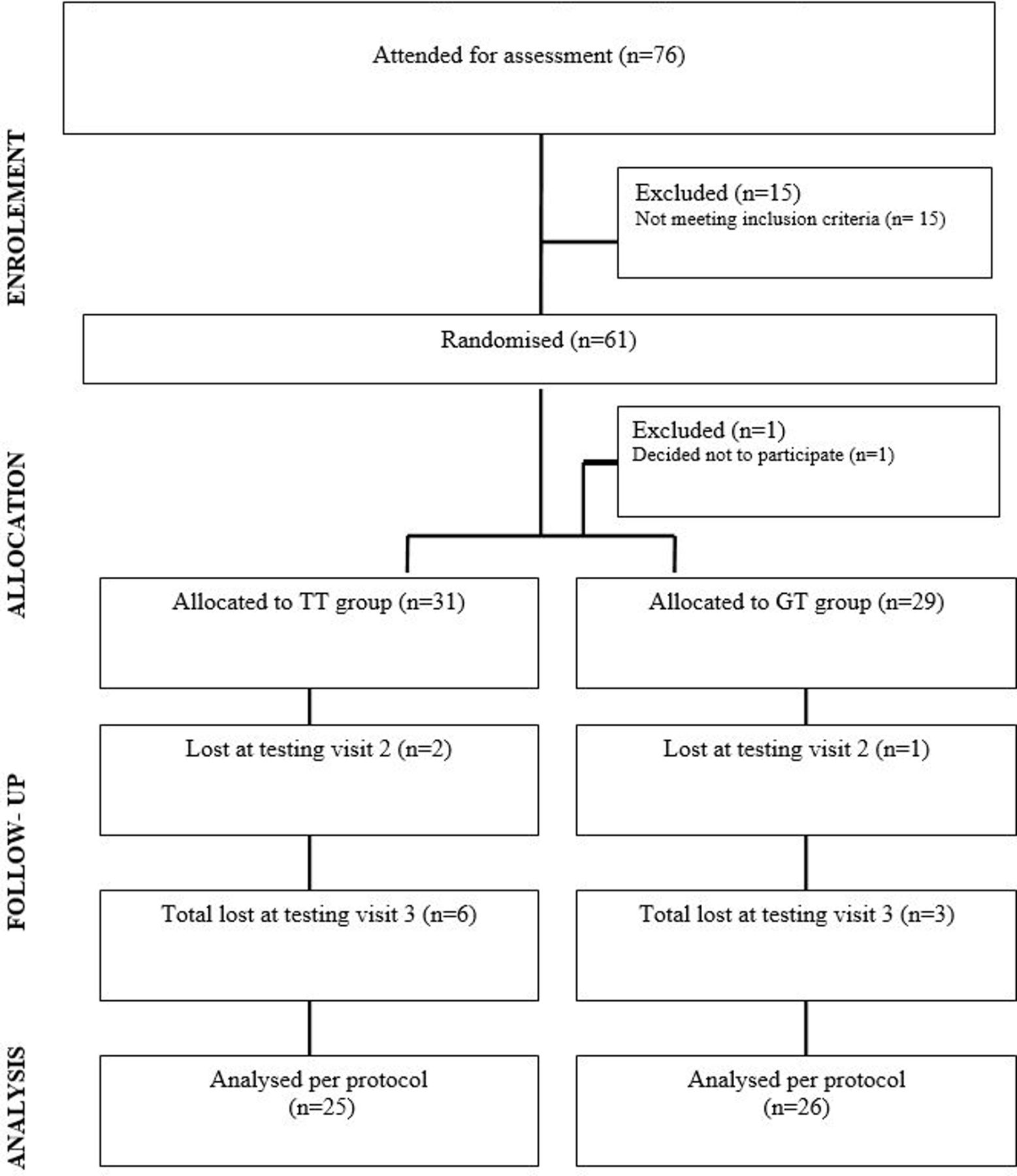
{kind=link}
The CONSORT statement diagram, detailing the participant flow through the trial. CONSORT, Consolidated Standards of Reporting Trials; GT, general thrust; TT, targeted thrust.
Both groups of subjects had similar demographic, anthropometric and pain characteristics at the start of the trial (see table 1).
Baseline characteristics of the two groups following randomisation
Changes in pain
Table 2 summarises differences in pain assessment for both treatment groups at each time point of assessment. A repeated measures of ANCOVA, including baseline scores as a covariate, revealed no between-group differences in self-reported pain, disability or PPTs for the muscles studied (see table 3).
Descriptive statistics for the pain measurements
Repeated measure ANCOVA: pain by time × group
Change in sEMG stretch-reflex responses
There was a statistically significant change in the differences in the magnitudes of the sEMG reflex response to TT and GT, over three successive treatment visits, in the multifidus muscles (see table 4). There was a trend, in the TT group, toward a larger sEMG reflex response at test 3, than at test 1. There was no significant difference in the magnitude or acceleration of the SM thrust in between groups (ANOVA time × group, F=0.01, significance=0.97). The consistency of the magnitude of acceleration during thrusts (in both GT and TT groups) (intrarater reliability of the pooled data) was excellent (ICC2,1 =0.96; 95% CI 0.92 to 1.00).
Descriptive statistics: sEMG responses for TT and GT groups at each visit
Discussion
This trial took two similar groups of subjects with low back pain and compared the effect of a manipulative TT technique aimed toward a clinician-defined target versus a similar magnitude thrust technique that was not targeted toward a specific level of the lumbar spine. There were no differences in disability or pain reductions between the groups. Pain was measured as self-reported pain levels or in pressure-pain perception in the lumbar muscles. There was an increase in the stretch-reflex sEMG response in the lumbar multifidus muscles of the TT group, across the three visits.
Our data suggest that targeting a manipulative thrust technique to a clinician-defined, specific level of the lumbar spine does not improve self-reported pain or disability levels. This extends previous reports that compared methods of joint mobilisation and manipulation.7 8 19 All these data (our study and related studies) suggest, it may be necessary for manual therapy scientists to re-evaluate the paradigms traditionally used to explain the therapeutic mechanisms of applied passive movement to the spine. We report that specifically targeted manipulation amplified the local stretch-reflex response, though it did not reduce pain (compared with the control group), over the course of three visits. One could speculate that as subjects attended for repeated visits, they anticipated that they were to going to receive a thrust to a specific locality resulting in a ‘protective’ muscular excitability to stretch, via an increase in alpha motor neuro pool activity, a phenomenon that has been observed with lumbar manipulation previously.10 20 21
Limitation
The study had some limitations. A post hoc power calculation, using the observed between group difference and variance, showed that actually a sample size of 34 in each group would have led to the β value of 20% and an α value of 5%, with regards to pain. This study’s α and β values were 0.05% and 32%, respectively, and thus the study was slightly underpowered, raising the chance (by 12%) of a false negative. The study was single blind, as the experimenter had to know which group the subject was in to deliver the correct SM thrust. This may have impacted on the relationship between experimenter and subjects, providing an element of bias.
The impact of selecting and targeting a manipulative thrust technique, to a clinician-defined ‘symptomatic’ level on pain and disability was no greater than that achieved by a GT of the lumbar spine. These data are similar to findings from a study undertaken with a younger, military sample,8 showing no significant difference in pain response to a general versus specific rotation, manipulation technique. Similar evidence demonstrating equivocal pain reductions following mobilisation (slow oscillatory movements) applied to either clinician-defined ‘target’ spinal levels or when randomly applied mobilisation to any level in a region of the spine7 adds to the need to question the benefit of the process of targeting passive movement to clinician-defined symptomatic levels.
In summary, if ‘targeted’ manipulation proves to be no better than ‘general’ manipulation (when there has been further research, more studies), it would challenge the need for some current training courses that involve comprehensive manual skill training and teaching of specific techniques. If simple SM interventions could be delivered with less training, than the targeted approach currently requires, it would mean a greater proportion of the population who have back pain could access those general manipulation techniques. We conclude that this treatment approach—general manipulation—needs to be considered with an open mind and researched further.
References
Footnotes
Contributors LP was the lead investigator and undertook experiments. CJM was supervisor of the work and lead author on this paper. JAO was supervisor of the work and reviewer of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval A favourable ethical opinioin was obtained from North Manchester Local Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.