Article Text

Abstract
While there is a multitude of evidence supporting the efficacy of injury prevention training programmes, the literature investigating the implementation of these programmes is, in contrast, rather limited. This narrative review sought to describe the commonly reported barriers and facilitators of the implementation of injury prevention training programmes among athletes in organised sport. We also aimed to identify necessary steps to promote the uptake and sustainable use of these programmes in non-elite athletic communities. We identified 24 publications that discussed implementing evidence-based injury prevention training programmes. Frequently reported barriers to implementation include the perceived time and financial cost of the programme, coaches lacking confidence in their ability to implement it, and the programme including exercises that were difficult or confusing to follow. Frequently reported facilitators to implementation include the coach being aware of programme efficacy, shared motivation to complete the programme from both coaches and athletes, and the ability to easily integrate the programme into practice schedules. The current literature is focused on high-income, high-resource settings. We recommend that future studies focus on understanding the best practices of programme dissemination in culturally and economically diverse regions. Programmes ought to be of no financial burden to the user, be simply adaptable to different sports and individual athletes and be available for use in easily accessible forms, such as in a mobile smartphone application.
- prevention
- implementation
- exercises
- injury
- sports
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The previous literature has described the efficacy of evidence-based injury prevention training programmes.
Effective programmes are comprised of neuromuscular training, plyometric exercises, balance training and stretching.
Despite generally high efficacy, program implementation rates remain low.
WHAT THIS STUDY ADDS
Frequently reported barriers to injury prevention program implementation include the perceived time and financial burden, coaches lacking confidence in their knowledge to implement the program properly and the complexity of the programme’s exercises.
Commonly reported facilitators to injury prevention program implementation include the coach’s knowledge of the programme’s efficacy, motivation to complete the program from both the coach and the players, and the programme’s ease of integration into the usual practice schedule.
Current literature on this topic is focused in high-resource and high-income countries.
We provide specific recommendations for researchers, clinicians, and administators to encourage the wider and more sustained implementation injury prevention exercise programs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We suggest that future studies on injury prevention exercise programmes use implementation-specific frameworks to guide the assessment of implementation success, as well as qualitative methods to better understand the attitudes and beliefs of key stakeholder groups.
Future studies should also investigate the barriers and facilitators to injury prevention exercise program implementation in a wider range of athletic communities.
Parents of adolescent athletes are important stakeholders in this realm and seem to be currently underutilised. Parental buy-in could be an invaluable tool to encourage the broader use of injury prevention exercise programs in youth sports.
We suggest that injury prevention exercise programmes be made available in free mobile smartphone applications to increase ease of access and sustained use.
Introduction
Osteoarthritis (OA) is one of the most common chronic health conditions in the USA, substantially contributing to the burden of chronic pain and disability.1 The prevalence of knee OA has nearly doubled since the mid-20th century, even after adjusting for age and body mass index.2 Recent studies demonstrate that knee OA makes up roughly 80% of the total burden from all forms of OA.2 About 19% of Americans aged 45 years and older are affected by knee OA; however, increasing evidence shows that OA also should be of concern for certain young athletes, especially those with a history of knee injury.2 3
Lower-limb injuries account for over 65% of all sports injuries.4 Arguably of greatest concern, anterior cruciate ligament (ACL) injuries are associated with long-term economic and health burdens. Surgical reconstruction of the ACL and its long-term costs are estimated to be as high as US$38 000 per patient.4 There is a known association between ACL injury and the later development of OA.3 5–7 This is of particular concern for young athletes, who, after sustaining an ACL injury, are at significantly increased risk of developing OA as early as 5–15 years after an ACL injury.5 Working to prevent initial knee injury is thus necessary to reduce the additional burden of living over half their life with OA.
Numerous randomised controlled trials have demonstrated the efficacy of injury prevention training programmes in reducing ankle and knee injuries in athletes at youth, high school and elite levels.4 8–18 These programmes generally include neuromuscular training, plyometric exercises, balance training and stretching.4 Exercise regimens are recommended to be performed 2–3 times per week through the pre-competitive season, in-season and during out-of-season maintenance. However, they do not need to be overly time-intensive and can be integrated into a pre-existing warm-up or conditioning routine.4 Several injury and athletic organisations, including the National Athletic Trainers’ Association, the Academy of Orthopaedic Physical Therapy, the American Academy of Sports Physical Therapy, the Osteoarthritis Action Alliance, the American College of Sports Medicine and the International Olympic Committee, support and offer guidance on the use of injury prevention programmes to prevent knee injuries.4 19–22
While the literature investigating the implementation of these programmes is limited, some research indicates usage rates are as low as 20%–29% in the youth soccer community, despite the multitude of evidence supporting their effectiveness.23 24 Further information about the current state of implementation of injury prevention programmes is critical to promote widespread dissemination and adoption. This paper aims to describe the frequently reported barriers and facilitators of injury prevention training programme implementation among athletes in organised sports. We aim to identify steps needed to promote the uptake and continued use of these programmes in community-level sports environments.
Methods
An electronic database search of the literature was conducted between February and March 2021 by two authors (MCM and LH). We did not restrict the search to publication date, but the results were limited to articles printed in English. The search took place in PubMed, Google Scholar, the Cochrane Library and the Cumulative Index of Nursing and Allied Health Literature. A combination of the following terms was used during this search: ‘implementation’, ‘exercise programme’, ‘injury prevention’, and ‘sports’. We conducted a comprehensive narrative review rather than a traditional systematic review because our focus was to gain a more general, larger-scale view of the current literature investigating injury prevention training programme implementation barriers and facilitators within a broad range of youth and adult non-elite athletic communities. Thus, data extraction and synthesis were not feasible for all eligible articles because of the variability in the types of articles, study designs and research areas (eg, effectiveness of implementing a specific injury prevention training programme, barriers/facilitators to injury prevention training programmes, implementation science) on this topic. We did not use strict criteria to exclude articles found through our search to preserve our goal of gaining a broader scope on this topic. Titles and abstracts were reviewed by two authors (MCM and YMG), and the full text was obtained for articles that included the implementation of injury prevention training programmes. We performed quality assessments of the retrieved articles. The two authors reviewed the identified articles using a spreadsheet that included quality assessment items from Walsh et al25 for qualitative studies and Shea et al for systematic reviews.26
Results
Overview of the current implementation literature
We identified 23 publications that discussed topics related to the implementation of evidence-based injury prevention training programmes: 16 analysed barriers and facilitators regarding specific injury prevention training programmes, while 7 discussed more generally how to approach implementation science research on this topic. Of the 16 studies that investigated specific barriers and facilitators, 4 were based in Australia,27 28 2 were based in Scandinavia,29 30 3 in the USA,23 24 31 32 2 in Canada,33 34 1 in Switzerland35 and 4 were systematic reviews studying injury prevention training programmes based in various regions.31 36–38 A representative sample of these studies is described in detail in online supplemental table 1.
Supplemental material
Summary of the current literature
We found that the majority of the studies included in this review met all identified quality assessment measures. Tables summarising these results are included in online supplemental tables 2 and 3. We found that a qualitative study by McGlashan et al did not fully describe the methods used to conduct semistructured interviews and a systematic review by O’Brien and Finch did not discuss the likelihood of publication bias from the articles they described.27 39
Supplemental material
Supplemental material
While synthesising the results from the current literature, we found common themes in the reported barriers and facilitators to implementing injury prevention training programmes (figure 1). Many studies reported that the extra time, ranging from 5 to 20 min required to complete the programme, was the biggest barrier noted by coaches.28 30 31 33 40–42 Even coaches who reported they had not used an injury prevention training programme indicated that the perceived time burden of the programme was too high. Data on coaches’ knowledge about injuries and injury prevention techniques varied greatly. Little knowledge in this area and viewing injury prevention as a low priority were common barriers to implementation.24 27 28 30 35 37 42 On the other hand, knowledge surrounding the burden of injury did not always facilitate the adoption and implementation of an injury prevention training programme.43

Summary of perceived barriers and facilitators of injury prevention exercise program implementation.
Some studies found that coaches felt they lacked the necessary physical equipment and support staff resources to properly implement injury prevention training programmes.41 42 It is important to note, however, that additional physical equipment is not a requirement of many injury prevention programmes, thus this barrier can be easily overcome with certain programmes. Unsurprisingly, support from key stakeholders, including coaches, administrators, athletic trainers and injury prevention training programme experts, was found to be an important facilitator in injury prevention training programme implementation.27 Additionally, the complexity and difficulty of the exercises included in injury prevention training programmes were reported as barriers to implementation.34 44 Conversely, studies reported that programmes easily adaptable to individual teams, sports and athletes were more likely to be implemented.34 42 45 This result could relate to the finding that players’ lack of motivation also affected whether or not a programme was implemented.28 31 40 41
Looking specifically at the US-based literature, some studies have investigated barriers and facilitators in injury prevention training programme implementation in high school and collegiate sports teams. A 2015 study of soccer and basketball coaches in Oregon high schools found that the coaches believed there was little need for an injury prevention training programme given low injury rates. The perception that injury prevention training programmes were complex and difficult to administer prevented the initial adoption of programmes.24 In a 2020 study by Dix et al, NCAA Women’s soccer coaches in the NCAA East Region reported that the perceived need to hire additional coaching staff who could administer an injury prevention training programme was the biggest barrier to implementing a programme with their teams.32 A study focusing on club-level soccer coaches indicated that even high levels of intent to incorporate an injury prevention training programme into team practices did not necessarily translate to high levels of implementation.43 Even an educational workshop intervention aimed to increase the adoption of injury prevention training programmes in this population did not drastically increase adherence rates.43 Implementation success with these types of educational workshops has been found in another study, however.46
Discussion
Directions for researchers
Many of the studies found through this review were set within randomised clinical trials. While testing the efficacy of new injury prevention training programmes cannot be disputed as essential, it is also necessary to use pragmatic or hybrid designs to better understand the implementation of injury prevention training programmes in real-world settings outside of randomised clinical trials.47–49 True effectiveness trials are limited.50 The current literature is set on the qualities that make an effective injury prevention training programme when implemented appropriately. Still, the evidence is lacking on the optimal strategies to best disseminate these programmes to ensure widespread uptake, adoption and long-term use. Similar to suggestions made previously by Finch,51 we support future studies’ use of the seven-step Translating Research into Injury Prevention Practice (TRIPP) Framework as well as Padua’s seven steps for developing and implementing a preventive programme as roadmaps to drive intervention planning, and the use of both the Reach, Effectiveness, Adoption, Implementation, and Maintenance Framework and the TRIPP Framework to direct the evaluation of programme implementation and adoption.39 52 53 Long-term studies are also needed to examine how injury prevention training programmes endure over time.
Furthermore, we believe that the inclusion of qualitative interviews with key stakeholders will be a valuable addition to the current body of the literature and provide essential feedback on how to improve their involvement in injury prevention training programme implementation, dissemination and maintenance. The use of qualitative methods in sports medicine is growing. Understanding stakeholder motivation and their knowledge, attitudes and beliefs surrounding the implementation of injury prevention training programmes will help identify education initiatives and improve implementation techniques. Researchers in the area of concussion prevention and management have successfully used qualitative methods to identify gaps in knowledge and factors related to the attitudes and beliefs of athletes, parents and coaches.54–56 Valuable insights have been gained using qualitative methodology to examine the implementation and use of an injury prevention training programme through research in Europe.57–59 Applying similar techniques in other geographic regions will improve injury prevention training programme implementation strategies.
Currently, the literature on injury prevention training programme efficacy, implementation and adoption are primarily set in homogenous, high-resource communities in high-income countries, such as Australia, Canada the USA and European nations. There is a significant gap in the literature investigating the use of injury prevention training programmes in culturally and economically diverse settings globally. Conducting this type of research in underserved areas requires careful attention to address an array of ethical concerns. For example, investigators should ensure communities can sustain the tested injury prevention training programme after the study. We suggest targeting implementation strategies to middle and high school sports programmes in underrepresented areas as an initial step in expanding the use of these programmes within these communities. Many evidence-based injury prevention training programmes benefit from not requiring additional equipment resources. We see this factor as a facilitator to implementation and a way to ensure programme accessibility no matter the user’s socioeconomic status. It will, however, be important to study how well current injury prevention training programmes and new programmes integrate into diverse settings where sports culture and injury needs may differ. Drawing from key ideas within the implementation and dissemination science realm, the use of systematic evaluation of the social, cultural and environmental context is necessary to encourage the spread, scalability and sustained use of evidence-based injury prevention programmes.60
Directions for clinicians and administrators
The current literature provides a good base to describe the principles of effective and implementable injury prevention training programmes. We found that injury prevention training programmes that are flexible and easily incorporated into the existing practice schedule for a team are more likely to be adopted. We also found evidence supporting the importance of involving key stakeholders, including coaches and players. Studies show that buy-in from coaches and players is a necessary first step to injury prevention training programme implementation.53 61 62 Education on the importance of injury prevention and the efficacy of injury prevention training programmes can help coaches feel adequately equipped to administer the injury prevention training programme. However, buy-in from coaches alone is not enough—players also need to be involved and feel motivated to participate in the injury prevention training programme.63 64 To achieve this goal, it may be beneficial to promote the positive effects injury prevention exercise programmes can have on overall biomechanics and athletic performance. Some studies have found evidence associating injury prevention training programme completion with increased lower extremity strength and flexibility,65 66 vertical jump height,66 67 balance ability67 and maximum aerobic power,66 all of which can, in turn, advance athletic performance.65–67
Additionally, it would be beneficial to encourage buy-in for these programmes from the parents of adolescent athletes. While the literature on this particular aspect of stakeholder involvement is lacking, we suggest that educational efforts on the importance of these programmes be expanded to include parents. Parent involvement—and influence—in youth sports continues to increase, highlighting the invaluable need to include this previously untapped group in efforts to expand the implementation of injury prevention programmes in community athletics.68 69 Parents’ investments in terms of time and money into their children’s sports teams can be powerful tools that assist in changing the overall culture around injury prevention in these types of community settings.
We also note that it will be important to encourage injury prevention training programmes in school settings and recreational non-elite athletic environments. Previous studies have investigated the efficacy of injury prevention training programmes in school physical education classes.70 71 While results from these studies indicate that these programmes can successfully reduce injury occurrence, further research is needed to understand the specific barriers and facilitators to implementation in adolescent physical education classes as they likely differ from those associated with outside-of-school non-elite athletic settings.
As previously detailed, the current literature describes the time required to complete an injury prevention programme as a key barrier to implementation. A number of the studies found through this review are limited by the detail of information around the comprehensive time burden of the studied injury prevention training programmes—in other words, questions remain around the number of times per week a programme was performed, the number of weeks during in-season competition the programme was performed, the number of weeks during out-of-season competition the programme was completed, and whether the programme was completed all at once or separated throughout practice. These are all important factors to consider in terms of how they contribute to programme implementation and long-term compliance.37 72 The current best practice guidelines from the National Association of Athletic Trainers indicate that evidence-based injury prevention programmes can be performed in as little as 10–15 min, 2–3 times per week to be effective.4 Future research will benefit from ensuring that data on the amount of time required to complete a programme is reported. This type of information is necessary to understand the optimal balance of programme time that will ensure high levels of efficacy while limiting the overall time burden in different non-elite athletic settings. As noted in Padua’s seven-step guidelines for programme implementation, a ‘one-size-fits-all’ approach to injury prevention training programmes does not seem feasible.53 Instead, programmes must be flexible to accommodate the setting-specific barriers and facilitators to implementation.
To increase ease of access to and the sustained use of injury prevention training programmes, we suggest that programmes include a free smartphone mobile application version. An estimated 80% of the world’s population has a mobile phone, suggesting that mobile applications would greatly expand access to evidence-based injury prevention exercises to communities that previously may have been excluded from this content due to geographic and monetary factors.73 A literature review conducted in 2014 found that only four evidence-based injury prevention applications were available for mobile download.73 A free mobile application could address a number of the perceived barriers in implementation found through this comprehensive review, including barriers related to cost, coaches lacking educational materials on injury prevention, a need to individualise the programme for different athletes and a lack of explanation for confusing or difficult exercises.
Conclusions
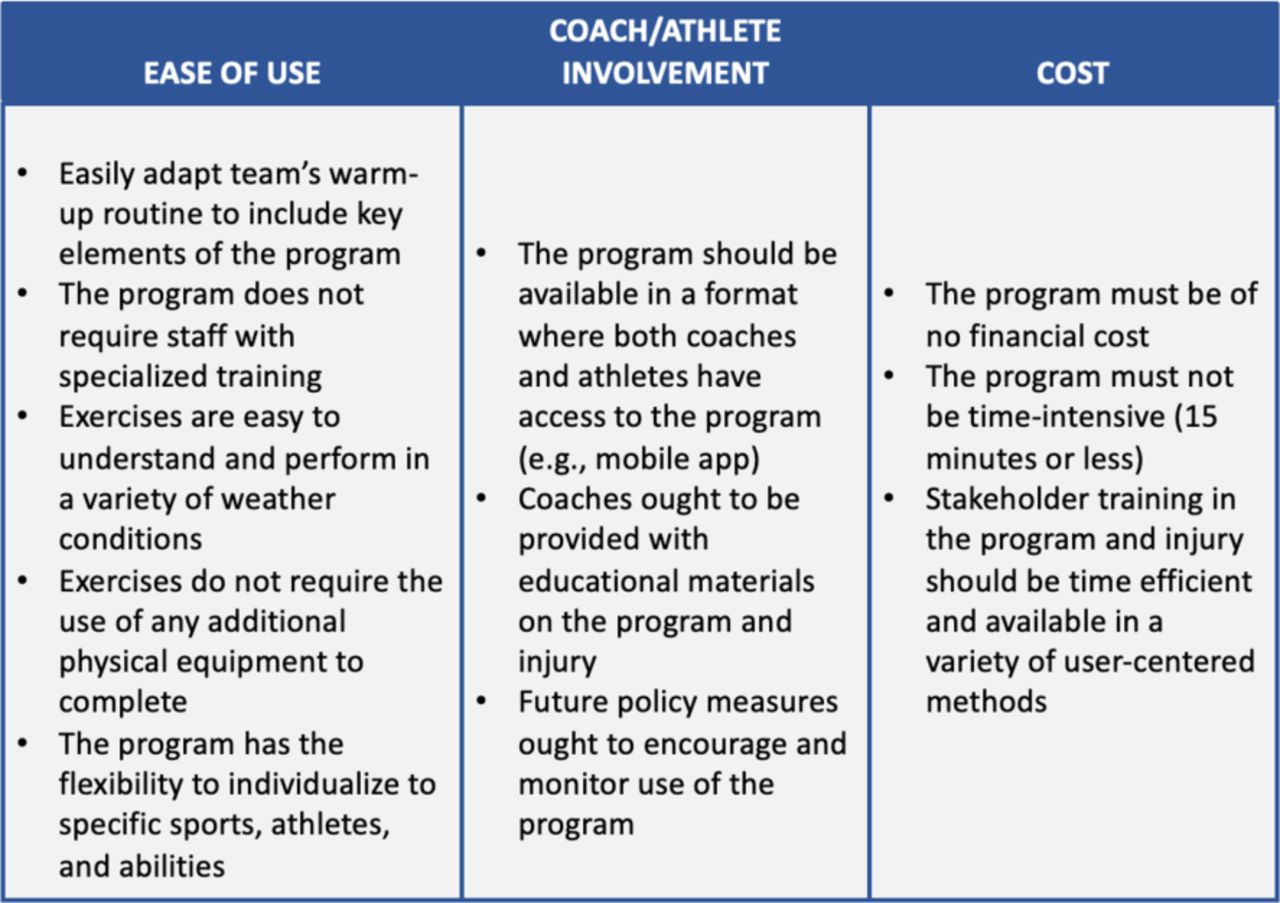
Recent literature agree on the qualities that make an injury prevention training programme effective at preventing injuries. Despite the known positive benefits of these programmes, uptake and adoption rates are still quite low. Even more surprising, there is a major gap in the literature investigating strategies aimed at improving implementation rates across a wide range of athletic communities. Based on the findings of this review, we propose recommendations to facilitate the implementation of future injury prevention training programmes (figure 2). Additionally, we recommend engaging professional sport and coaches’ associations to promote the use of and disseminate educational information on evidence-based injury prevention programmes. Perhaps most novel, we recommend that injury prevention training programmes be available in free smartphone mobile applications. We see the convenience and ease of access of a mobile application as key factors that will facilitate the initial uptake and long-term use of injury prevention training programmes.

{kind=link}
{kind=link}
Recommendations to increase injury prevention exercise program implementation.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JTS and YMG are joint senior authors.
Contributors Substantial contributions to study conception and design: MCM, JTS and YMG. Substantial contributions to acquisition of data: MCM, LH, HJR, JD, LJD and YMG. Substantial contributions to analysis and interpretation of data: MCM, LH, HJR, JD, LC, KRA, JTS and YMG. Manuscript preparation: MCM and YMG. Critical revisions to the manuscript for intellectual content: MCM, LH, HJR, JD, LJD, LC, KRA, JTS and YMG. Final approval of the submitted manuscript: MCM, LH, HJR, JD, LJD, LC, KRA, JTS and YMG.
Funding This study was funded by Centers for Disease Control and Prevention (Grant number: #NU58DP006980).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.