Article Text

Abstract
Background Sidestep cutting technique is essential in programmes to prevent anterior cruciate ligament (ACL) injury. A better understanding of how technique affects potentially harmful joint loading may improve prevention programmes. The purpose of this study was to investigate the effect of sidestep cutting technique on maximum knee abduction moments.
Methods Cross-sectional study. Whole-body kinematics and knee joint kinetics were calculated in 123 female handball players (mean±SD, 22.5±7.0 years, 171±7 cm, 67±7 kg) performing sidestep cutting. Three cuts from each side were analysed. Linear regression was applied between selected technique factors and maximum knee abduction moment during the first 100 ms of the contact phase. Furthermore, we investigated to what degree the abduction moment originated from the magnitude of the ground reaction force (GRF) or the knee abduction moment arm of the GRF.
Findings Technique factors explained 62% of the variance in knee abduction moments. Cut width, knee valgus, toe landing, approach speed and cutting angle were the most significant predictors. An increase in one of these factors of 1 SD increased the knee abduction moment from 12% to 19%. The effect of the moment arm of the GRF was more important than the force magnitude for maximum knee abduction moments.
Interpretation Lower knee abduction loads during sidestep cutting may be achieved if cuts are performed as narrow cuts with low knee valgus and toe landings. These factors may be targeted in ACL injury prevention programmes.
- Biomechanics
- Knee ACL
Statistics from Altmetric.com
Introduction
The majority of anterior cruciate ligament (ACL) injuries occur in cutting, jumping and single-leg landing manoeuvres.1–5 Knee valgus motion has been identified as an important component of the injury mechanism in recent three-dimensional kinematical analyses of injury situations (Koga 2010 og Koga 2011). It has also been reported that knee valgus angles and knee abduction moments measured in drop jumps can predict ACL injury.1 ,6–9
Prevention programmes focusing on avoiding knee valgus have proven effective, but unfortunately lack of compliance is a serious threat to their effectiveness.10 Further knowledge on how to improve these programmes may reduce the training time and increase the preventive effect, which again may increase the compliance of the athletes.11
Movement technique can affect maximal knee abduction moments, and predictors for high loading have been identified in analyses of simple change of direction tasks.12–14 Recently, Myer et al15 reported predictors for high knee abduction moments in drop jumps, and used these results to develop clinical screening tools for high-loading individuals, believed to be at increased risk of ACL injury. Another approach is to target identified predictors in preventive training. Dempsey et al16 ,17 were able to reduce knee abduction moments by instructing players to perform cuts with the stance foot closer to the midline and the trunk more erect. These results are promising; however, it remains to be seen whether such movement pattern changes are functional during match play. Sidestep cutting during active game play is a complex movement, usually performed to fake an opponent, which is different from a simple change of direction.18 Therefore, laboratory studies should strive to mimic the actual playing situation. In fact, it has been shown that just including a static defender (dummy) to the testing situation affects motion patterns substantially.19
In order to reduce maximum knee abduction moments, it is necessary to reduce either the magnitude of the ground reaction force (GRF) or its moment arm in the frontal plane. The relative importance of these two factors may have implications for prevention strategies. Soft landings are believed to reduce the maximum GRF, while avoiding valgus alignment is thought to reduce the moment arm of the GRF in the frontal plane.
As ACL injuries are likely to occur within the first 40 ms of the contact phase, technique training that reduces knee valgus motion and abduction loading during the early landing phase should be emphasised.8 The purpose of this study was to investigate the relationship between self-selected, sport-specific sidestep cutting technique and knee abduction moments during early stance phase. A second aim was to investigate which of the two factors, moment arm and magnitude of the GRF, that were mostly affected by the technique parameters. The technique factors selected were chosen from previous relevant studies.12 ,13 ,17
Methods
Subjects
Prior to the 2007–2008 season all Division I players in the Norwegian female handball league were invited to baseline testing for a cohort study initiated to investigate risk factors for ACL injuries, and 184 players were tested. We excluded 11 players who were not match fit because of injuries. Based on player lists from the team coaches, the 173 match fit athletes represent 84% of the eligible athletes. All back and wing players (N=125) were selected for analysis, regardless of their previous injury status. Back and wing players were selected as players in these positions normally perform sidestep cutting during match play. Two had to be excluded due to technical problems; thus, the final sample consisted of 123 players (22.5±7.0 years, 171±7 cm, 67±7 kg, mean±SD).
Procedures
The study was approved by the Regional Ethics Committee and informed consent was obtained from all players.
Testing
The players performed sidestep cutting in a biomechanics lab. Eight 240 Hz infrared cameras (ProReflex, Qualisys, Gothenburg, Sweden) recorded the movement of 35 reflective markers attached over anatomical landmarks.20 GRF and centre of pressure were recorded using a 960 Hz force platform (AMTI, Watertown, Massachusetts, USA).
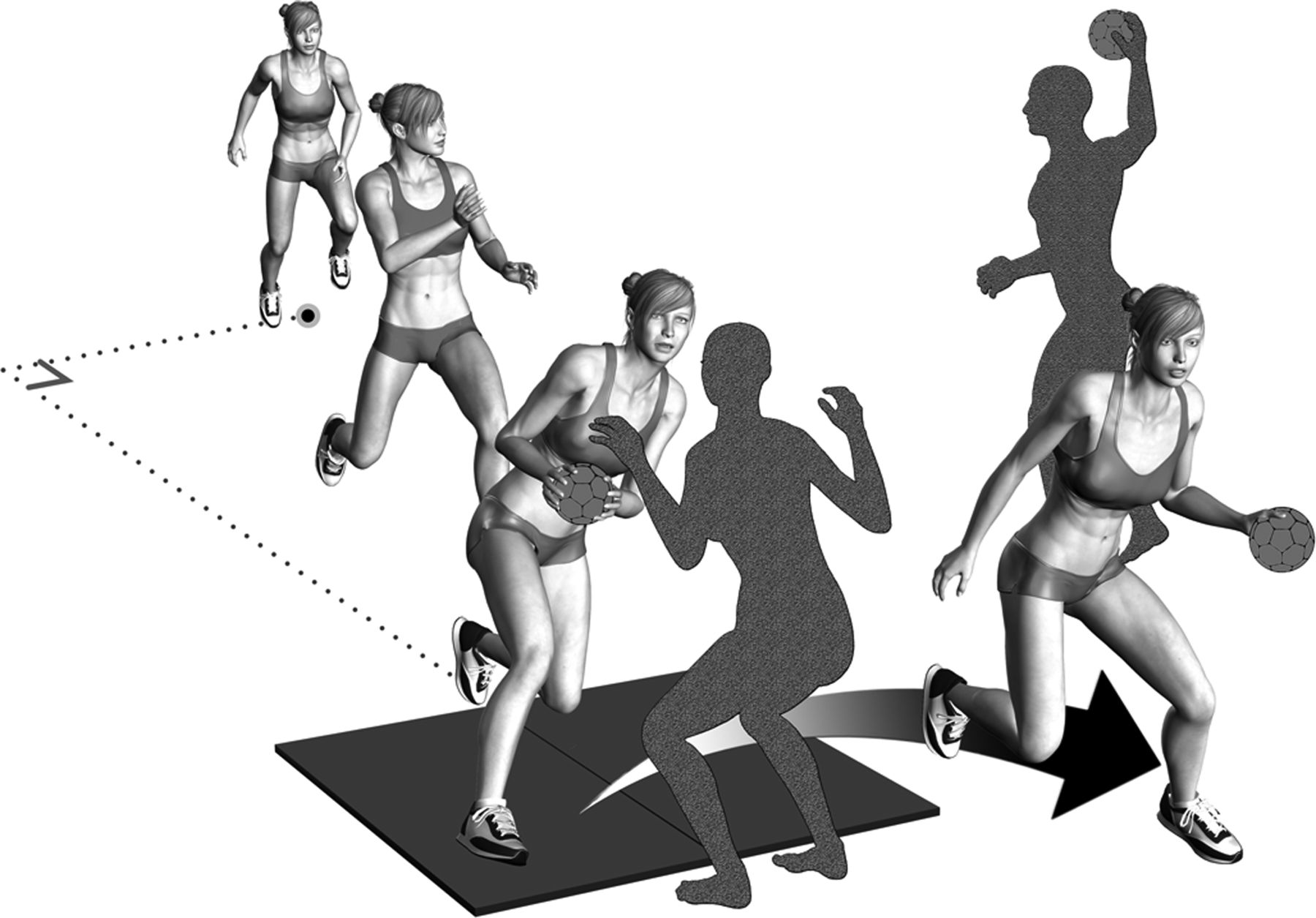
The players performed a side step cutting manoeuvre past a human static defender (170 cm). They accelerated for 6 m, received a pass from a team mate or an investigator in the final step before the cut, and arrived at an angle of approximately 30° to the long axis of the runway (figure 1). They were instructed to perform cuts similar to what they would do during active game play, focusing on faking the defender to go to one side and passing her on the other side. The defender was completely static during testing, but adjusted her position between trials to ensure that the ‘attacking’ player stepped onto the force platform with her stance foot. This ensured that the player focused on faking the defender rather than trying to hit the force platform.

Testing situation. Players started at an angle of approximately 33° on the long axis of the runway. They were instructed to try to fake the defender into going to one side while cutting to the other. The defender was completely static and adjusted her position between the trials so the players hit the force platforms with their normal sidestep cutting technique.
The players performed up to three practice cuts to familiarise themselves with the situation. Subsequently, three successful trials from each side (left-right and right-left) were selected for analyses. Qualified personnel ensured that the trials selected were performed with match-like intensity with the stance foot on the force platform and all markers attached to the player's skin. Prior to sidestep cutting, all players went through a static, standing calibration trial. The motion analysis system was calibrated according to guidelines from the manufacturer.
Data processing
Marker trajectories were calculated and tracked with the Qualisys Track Manager (Qualisys, Gothenburg, Sweden). Both force data and marker trajectories were filtered using a Woltring spline with a 15 Hz cut-off frequency to avoid impact artefacts.20 ,21 The kinetics and kinematics were calculated in custom Matlab scripts (MathWorks Inc, Natick, Massachusetts, USA) as described previously,20 with hip and knee kinematics calculated using the Joint Coordinate System (JCS) convention and joint moments calculated with inverse dynamics and expressed as external moments projected onto the JCS axes.
Description of sidestep cutting technique
Sidestep cutting technique was described using the following variables at initial contact (figure 2): knee flexion, knee valgus, hip abduction, hip internal rotation, torso lateral flexion relative to the pelvis, torso rotation relative to direction of movement, speed of torso rotation, foot rotation relative to direction of movement and toe landing, in addition to approach speed at initial contact, cutting angle, total time of contact phase (‘cut time’) and cutting width. Toe landing was defined as the angle between the long axis of the foot and its projection on the ground. Cutting angle was defined as the angle between the velocity vector of the body centre of mass 10 frames (42 ms) before initial contact and 10 frames after toe off. Cutting width was defined as the angle between a line from centre of pressure to the centre of mass and the vertical in a plane perpendicular to the direction of movement 20 ms after initial contact. Approach speed was calculated from the absolute speed of the centre of mass at initial contact.
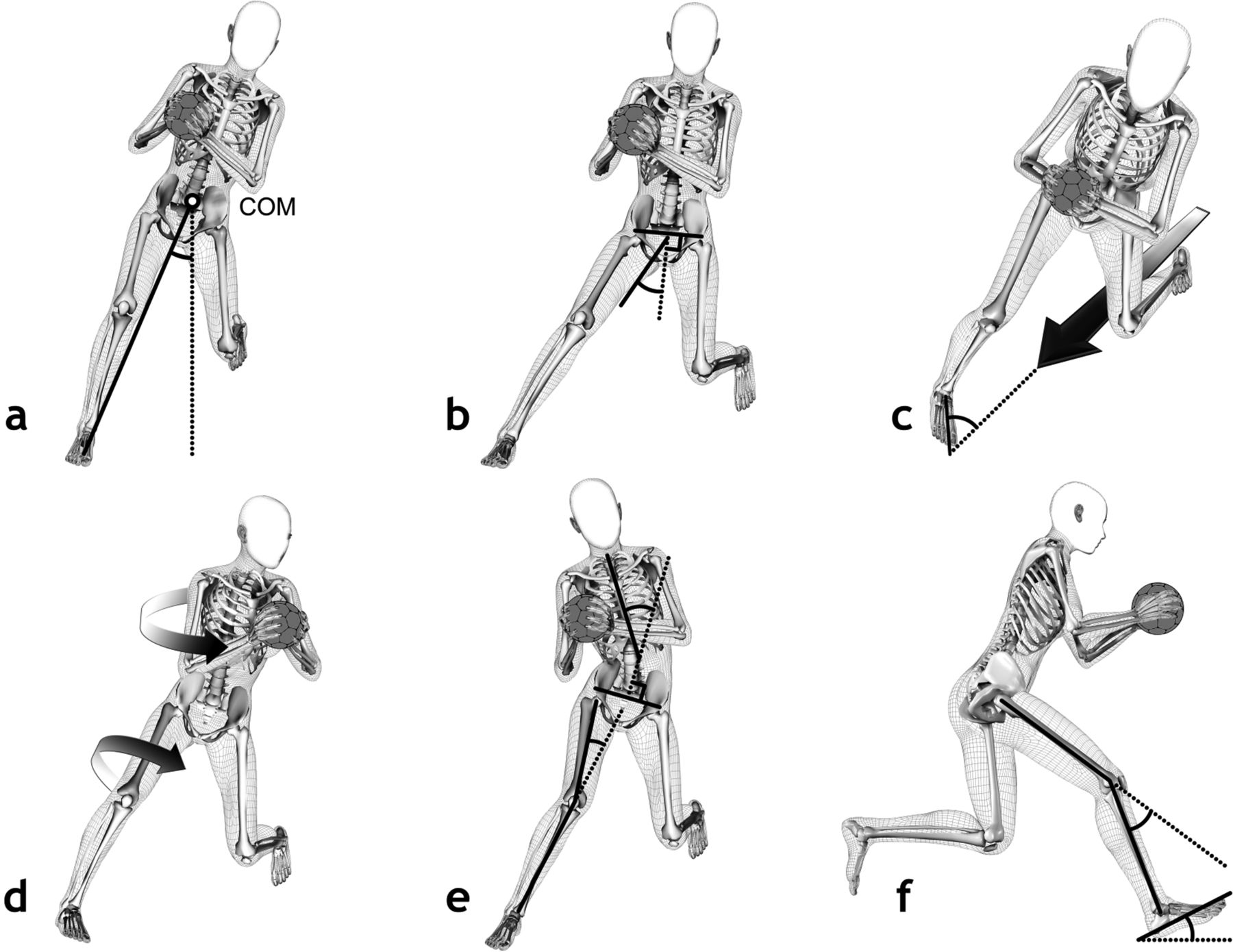
Technique factors described at initial contact. (A) Width of cut; (B) hip abduction; (C) foot rotation; (D) torso rotation and hip internal rotation; (E) torso lateral flexion and knee valgus and (F) knee flexion. Additional technique factors were approach speed, cutting angle, cut time and speed of torso rotation.
Calculation of simplified knee abduction moment
An estimated knee abduction moment ignoring the inertia of the segments was found using the equations 1 through 3. The moment arm of the GRF was found by equation 4.
An estimated resultant knee joint moment is calculated by
 where r is the vector from centre of pressure (COP) to knee joint centre; JCknee the coordinates of knee joint centre and COP the coordinates of COP.
where r is the vector from centre of pressure (COP) to knee joint centre; JCknee the coordinates of knee joint centre and COP the coordinates of COP.
According to the JCS convention,22 the abduction axis was defined as:
 Where ythigh is the medio-lateral axis of thigh; zshank the proximal-distal axis of shank and rabd the rotation axis of valgus.
Where ythigh is the medio-lateral axis of thigh; zshank the proximal-distal axis of shank and rabd the rotation axis of valgus.
The estimated knee abduction moment can then be found by
 The moment arm was then found by
The moment arm was then found by

Statistical analyses
Statistical analyses were performed in SPSS V.18 (SPSS Inc, Chicago, Illinosis, USA). A total of 738 cuts (2 sides×3 cuts×123 players) were included in the analyses. Knee abduction moments and GRF were normalised to body weight. The correlation between the estimated knee abduction moment and the knee abduction moment calculated using inverse dynamics was described with Pearson's correlation coefficient. Backward stepwise linear regression with probability of F to remove of 0.10 was used to investigate the associations between independent and dependent variables. The selected cutting technique variables were included in separate regression models on maximum knee abduction moment during the first 100 ms of the contact phase as well as the magnitude of GRF and the moment arm of the GRF in the frontal plane at the time of maximum knee abduction moment. The relative importance of each of the independent factors in the regression analysis is obtained by calculating the effect of changing each technique factor 1 SD and keeping the others constant. We did this by multiplying the regression coefficients with the SD of the corresponding factor, and expressed it as a percentage of the mean maximum knee abduction moment during the first 100 ms. Error bars are calculated from the SE of regression coefficients and the SD of the technique factors. One SD is considered a measure of the normal variation between subjects, and shows the potential for variation and change in the technique parameters. Regression analyses were also used to see how well the moment arm and the magnitude of the GRF could predict the maximum knee abduction moment calculated using inverse dynamics during the first 100 ms.
Results
The regression of technique variables and maximum knee abduction moment during the first 100 ms of the stance phase had an R2 of 0.62 with p<0.001. Speed of torso rotation, knee flexion and cut time were excluded from the final regression model due to low correlation with the outcome measure. The mean and SD of technique factors used to describe sidestep cutting technique are presented in table 1.
Mean, SD and range for technique variables and outcome measures
The mean (SD) maximal knee abduction moment during the first 100 ms of contact phase was 1.6 (0.66) Nm/kg (figure 3). We observed an excellent correlation (r=0.95) between the estimated knee abduction moment and this knee abduction moment calculated using inverse dynamics. Knee abduction moment showed a better correlation with the moment arm of the GRF compared with the magnitude of the GRF (table 2).
Regression of moment arm and magnitude of the ground reaction force at the time of maximum knee abduction moment on magnitude of maximum knee abduction moment

Mean (±SD) knee abduction moment during the first 150 ms of contact phase. N=738 sidestep cuts.
The regression of technique variables with the moment arm of the GRF in the frontal plane showed an R2 of 0.45 with p<0.001 (figure 5). Approach speed, cutting angle and rotation of foot were excluded from the final regression model. The regression of technique variables and magnitude of the GRF had an R2 of 0.37 with p<0.001. Lateral flexion of torso, toe landing, cut width, foot rotation and hip abduction were excluded from the final regression model.
The effect of different technique factors on the maximum knee abduction moment the first 100 ms are presented in figures 4 and 5. The regression equations are available in the online supplementary appendix.

Effect (% increase) on maximum knee abduction moment of increasing each factor 1 SD and keeping the others constant. N=738 sidestep cuts.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect (% increase) on ground reaction force and knee abduction moment arm of the ground reaction force at the time of maximum knee abduction moment of increasing each factor 1 SD while keeping the others constant. N=738 sidestep cuts.
Discussion
Knee valgus angle, toe landing and cut width were the technique variables where a 1 SD change produced the greatest effect on maximum knee abduction moment during the first 100 ms of the stance phase. A substantial effect was also seen of cutting angle and approach speed. The effect on maximum knee abduction moments of changing these factors 1 SD was 12–19%. For example, a decrease of 4.4° in knee valgus angle corresponds to a 19% decrease in knee abduction moment, and feet pointing 16° more downward corresponds to a 13% decrease. In total the selected technique factors accounted for 62% of the variance in maximum knee abduction moment.
We found that knee abduction moments increase with knee valgus, hip abduction, hip internal rotation, torso lateral flexion and toe landing, in line with what have been reported previously.12 ,13 ,17 In addition, we found significantly higher knee abduction moments in ‘wide cuts’. However, we did not find the relation between foot rotation and knee abduction moments reported by Sigward et al.13 This difference may originate from possible artefacts in their knee joint moments due to different cut-off frequencies for the filtering of force and marker data, as was recently demonstrated.20
An increase in knee loading is expected with increased performance. During match play, the need for speed and direction changes is dictated by the playing situation, including factors such as position of the ball, opponents, team mates and type of play. The impulse needed to perform the movement will be lower with a lower approach speed and a smaller cutting angle, and we demonstrate how approach speed and cutting angle are correlated with maximum knee abduction moments. This is also reflected in the analysis of cutting technique and GRF, where higher GRF was associated with higher approach speed, smaller cutting angle and a shorter cut time. These factors are not relevant to change in preventive training, as it may compromise the performance of the athletes.
The relation of the knee abduction moment to the moment arm of the GRF is stronger than the relation to its magnitude (table 2), indicating that alignment was more important than was the magnitude of forces. The force magnitude is directly related to acceleration through Newton's second law. This implies that alignment is more important for maximum knee abduction moments than are factors related the acceleration of the athlete, like the performance factors presented previously. Thus, changing alignment may provide an opportunity to reduce knee abduction moments without sacrificing performance.
Cut width, knee and hip frontal plane kinematics, as well as hip internal rotation, affected the moment arm of the GRF in the frontal plane, as seen from the regression analysis. These factors act to position the knee medially relative to the stance foot, which may increase the knee abduction moment arm and joint moment. Torso lateral flexion and rotation produce similar effects on the moment arm of the knee abduction moment. A simulation study of sidestep cutting has demonstrated how the knee abduction moment is sensitive to the centre of mass position,23 and this may explain the effect of the torso kinematics.
We expected that players using a toe landing would display lower GRFs due to energy absorption at the ankle joint, but this was not the case. In fact, toe landing was not even found to be a significant predictor for GRF at the time of maximum knee abduction moment. Surprisingly, the effect of toe landing on maximum knee abduction moment was mediated through an effect on the moment arm of the GRF. Toe landing appears to help players align their lower extremity to reduce the moment arm. A video analysis study demonstrated less toe landing in ACL injury situations compared with controls,3 and this may be explained by the more beneficial alignment with toe landings.
There are some limitations to this study. Skin movement artefacts are one of the most challenging problems of motion analysis, and the problems increase with higher speed and impact.24 Nevertheless, Besier et al25 have reported good correlation of results between two test sessions of sidestep cutting, and good test–retest reliability has been reported for drop jumps.26 The high number of participants in this study reduces the effect of random errors on the results. We found a consistent pattern of knee abduction moments across players, with a peak occurring at approximately 30 ms for most players (figure 3).
Knee abduction moments are but one risk factor for ACL injuries, and it is still not known to what degree the factors that predict increased knee abduction loading will also predict an increased risk of future ACL injuries. The strength of the present study is that we investigated separate components of the cutting technique and their immediate effect on knee biomechanics. This increases the understanding of how prevention exercises may work, and shows their potential effects.
There is some variation in the cutting techniques used in this study, but we believe that the validity is increased by letting the players perform their self-selected sidestep cutting technique. Injuries are sustained during this kind of movement; thus, it is a goal of injury prevention to change the knee biomechanics in the playing situation. Although cuts where performed with a somewhat lower approach speed than previous studies,27 all cuts were executed with a high intensity close to a match situation. The handball sidestep cuts are more demanding than simple direction changes, with the mediolateral movement to fake the static defender. This can be demonstrated by the magnitude of knee abduction moments, which were at least as high as those reported in previous studies.12 ,13 ,16 ,17 We added a ball to the testing situation to make it more sport specific, which may also have affected motion patterns.28
Sidestep cutting technique can be changed with training, and this study adds to the knowledge of which components to emphasise.16 ,29 ,30 By reducing dynamic valgus, placing the foot closer to the centre of mass and landing on their toes, athletes are likely to reduce knee abduction moment substantially. Some of the relevant factors are already targeted in effective prevention programmes, but more work is needed on how low-loading techniques can be implemented most efficiently.
Implications
Toe landings, narrow cuts and low knee valgus during sidestep cutting should be targeted in future ACL injury prevention programme to reduce maximum knee abduction moments and likely reduce ACL injury risk. The knowledge of the relation between technique variables and knee abduction moments can help inform the development of training protocols and training goals to promote safer sidestep cutting technique.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Correction notice This article has been corrected since it was published Online First. Errors in the third equation on page 2 have been corrected.
-
Funding The research of Eirik Kristianslund has been partly funded by the Medical Student Research Program at the University of Oslo. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport and Norsk Tipping AS.
-
Contributors EK and TK contributed to project planning, data acquisition, data processing, data analysis and writing of the manuscript. OF contributed to data acquisition, data processing, data analysis and writing of the manuscript. RB and GM contributed to project planning, data analysis and writing of the manuscript.
-
Competing interests None.
-
Ethics approval REK Sør (Regional Norwegian ethical committee).
-
Provenance and peer review Not commissioned; externally peer reviewed.