Article Text

Abstract
Objective: To test the hypothesis that chronic salbutamol intake improves performance during supramaximal exercise and to estimate the effects of this treatment on body composition, bone mass, and metabolic indices in healthy women.
Methods: Fourteen female volunteers (seven sedentary and seven recreationally trained) performed a 30 second Wingate test with and without salbutamol ingestion (12 mg/day for four weeks) in a random, double blind, crossover design. Blood samples were collected at rest, at the end of the test, and during passive recovery for lactate measurement. Body composition and bone mass were determined by dual energy x ray absorptiometry.
Results: Peak power appeared significantly earlier and was significantly (p<0.05) increased after salbutamol intake in all subjects. There was no difference in total work performed and fatigue indices with salbutamol compared with placebo. No significant alterations in lean or fat body mass and bone variables were observed with salbutamol treatment in either trained or untrained subjects during the trial. In contrast, blood lactate was significantly (p<0.05) increased during the recovery period after salbutamol ingestion compared with placebo.
Conclusion: As in men, chronic administration of therapeutic concentrations of salbutamol did not induce an anabolic effect in women but increased maximal anaerobic power. Further studies are necessary to clarify the mechanisms involved.
- BMC, bone mineral content
- BMCL, bone mineral content at the lumbar vertebrae
- BMD, bone mineral density
- BMDL, bone mineral density at the lumbar vertebrae
- women
- albuterol
- chronic intake
- performance
- body composition
Statistics from Altmetric.com
- BMC, bone mineral content
- BMCL, bone mineral content at the lumbar vertebrae
- BMD, bone mineral density
- BMDL, bone mineral density at the lumbar vertebrae
Only a few studies have investigated the use of β2 agonists as ergogenic aids during maximal or supramaximal exercise. This class of drug, in particular salbutamol, has become extensively used in the treatment of bronchial asthma and preterm labour. Moreover, β2 agonists have received recent attention from the International Olympic Committee and the World Antidoping Agency as drugs for enhancing muscle mass. Indeed, whereas aerosol use of these drugs seems to have a relatively selective action on the receptors in bronchial muscle, anabolic properties have been demonstrated in several species after systemic use of some β2 agonists coupled with a significant decrease in fat mass after relatively short periods of administration.1–3 In humans, both Martineau et al4 and Caruso et al5,6 found that short term therapeutic salbutamol administration improved strength but did not significantly affect lean body mass in healthy men. In agreement with these studies, we tested in a previous study7 the effects of salbutamol (12 mg/day for three weeks) during a Wingate test in healthy male subjects and found a significant increase in peak power with salbutamol without any change in body composition. However, whether this drug increases performance or muscle mass in women has yet to be determined.
A few studies on animals have also focused on the effects of β2 agonists on bone mineral, with contradictory results. Indeed, both an increase8,9 in suspended and denervated hindlimbs and a decrease under normal conditions10–13 in bone density have been reported in animals after clenbuterol and salbutamol administration. Only one study has focused on humans14 to determine if salbutamol helps resistance exercise to reduce unloading induced bone loss. The authors concluded that a resistance exercise/albuterol regimen probably increased bone mineral content by maintaining the mechanical loading stimulus. However, to our knowledge, there is no literature on the eventual effects of therapeutic systemic salbutamol administration on bone in humans without previously induced bone loss.
Therefore the primary purpose of this study was to test the hypothesis that short term oral salbutamol administration would improve performance in sedentary and trained healthy female volunteers during supramaximal exercise. Secondly, to investigate the possible effects of this treatment on muscle, bone, and metabolism, body composition (lean and fat mass), bone mineral measurements (bone mineral content and density), and metabolic variables (blood lactate) were monitored.
METHODS
Subjects
Fourteen women volunteered for the study, the protocol of which was approved by the ethics committee of Tours Hospital. Seven (mean (SD) age 20.9 (1.1) years) had been actively involved in a training programme two to three times a week for at least two years, and the remainder (mean (SD) age 23 (2.4) years) were sedentary. They were informed of the purpose and methods of the study before giving written consent to participate. The subjects were required to have been taking a low dose oral contraceptive pill continuously for the preceding 12 months. A medical history and physical examination excluded volunteers with a history of bronchospasm or atopy.
Subjects were asked to maintain similar exercise patterns and normal food intake and were required to continue taking the oral contraceptive pill at the same time each day, as specified for oral contraceptive usage, throughout the duration of the experiments. They were also instructed to abstain from intense exercise and ingestion of caffeine and alcohol for 24 hours before each trial, which was always performed during the second part of the menstrual cycle.
Exercise
The 30 second Wingate test was performed on a Monark pan loaded, bicycle ergometer with a resistance of 0.075 kg/kg body mass as recommended. During the test, the revolutions were determined using a magnetic switch and magnets mounted on the wheel of the ergometer. Revolutions were recorded by a computer and used in the calculation of the power variables. At the end of the Wingate test, rpm and resistance were used to calculate peak power as maximal anaerobic power, mean power as anaerobic capacity, time to peak power, and the fatigue index.
To familiarise themselves with the protocol and to increase the reproducibility of the test, subjects returned for an additional supramaximal anaerobic Wingate test trial ride in the two weeks before the actual experiment.
Drug
The double blind, randomised, crossover study consisted of two four week treatments (placebo and salbutamol) for each subject separated by a four week drug-free washout period. Placebo (gelatine) and salbutamol (trade name Salbumol, 2 mg, tablet; Glaxo-Wellcome Laboratory, Paris, France) were packaged in identical capsules. During the experimental periods, the subjects received three capsules daily of either placebo or salbutamol (4 mg—that is, two tablets per capsule), one capsule at 8 am, one at 12 pm, and one at 5 pm.
Trials to exhaustion were performed on the last day of each treatment after a final ingestion of either placebo or salbutamol.
Body composition and bone mineral indices
Body weight, body composition, and bone mineral indices were assessed four times, before and at the end of each treatment.
Body composition (fat and lean mass) was determined by dual energy x ray absorptiometry (Hologic QDR 1000/W; Hologic, Waltham, Massachusetts, USA) using a standardised procedure. The in vivo coefficient of variation was less than 2%.
Bone mineral content (BMC; g) and bone mineral density (BMD; g/cm2) were measured for the whole body and at the lumbar vertebrae (L2–L4; BMCL and BMDL). Measurements were performed with the dual energy x ray absorptiometry apparatus described above. The in vivo coefficient of variation using this technique was less than 1% at the specific regional site and up to 2.5% at the whole body level.
Experimental protocol
The protocol for each trial was identical. Trials were held at the same time of day (9 30–10 30 am) for each subject to prevent diurnal variations in hormonal responses. On the day of the experiment, subjects reported to the laboratory at 8 30–9 30 am, two hours after ingesting a capsule containing either placebo or salbutamol (4 mg) and one hour after ingesting a small meal, which was identical for each trial. Dietary consistency (about 500 kcal) was confirmed through self reported diet records and questioning before each trial. After insertion of a catheter into a superficial forearm vein (9–10 am), subjects warmed up with light cycling exercise. An accurate record was kept of the duration intensity of the warm up on the first trial (about two minutes), which was identical for all trials and not considered part of the total exercise time. The subjects then rested, and, at 9 30–10 30 am performed a 30 second Wingate anaerobic power test. Blood samples were taken at rest, at the end of the Wingate test, and after 5, 10, and 15 minutes of recovery.
Blood lactate analysis
Blood samples (1 ml) were promptly centrifuged, transferred in a chilled EDTA tube, and stored at −72°C until assayed for lactate. Analysis was by an electro-enzymatic method (Microzym; Biosentec, Toulouse, France). All assays were performed in duplicate. The coefficient of variation was <10%.
Statistical analysis
Data are presented as mean (SEM). An independent t test was used to evaluate the differences in subject characteristics between groups at the start of the study. A specific test for crossover trials was used to determine whether there were any significant differences between placebo and salbutamol performance variables. Differences in body composition, bone variables, and blood lactate between the trials were analysed by two way analysis of variance with repeated measurements. A post hoc Newman-Keuls test was performed to determine the location of the differences in the event of an analysis of variance revealing a significant main effect. The null hypothesis was rejected at p<0.05.
RESULTS
Performance
Whatever the treatment administered, peak power and mean power appeared to be significantly higher in the trained than the untrained subjects (p<0.05) (table 1). No significant differences in fatigue index, time to peak power, or peak power/kg were noted. With salbutamol treatment, there was a significant increase in peak power compared with placebo for both trained and untrained subjects (p<0.05). Moreover, time to peak power was significantly decreased for trained and untrained subjects with salbutamol treatment compared with placebo (p<0.05). No significant differences in mean power or fatigue index were found.
Performance in the Wingate test after placebo and salbutamol treatment in trained and untrained subjects
Body composition
At the beginning, there were no differences between the trained and untrained groups in fat mass (kg) and fat mass related to body weight (%) (fig 1). In contrast, both body mass and lean mass were significantly higher in the trained than the untrained subjects (p<0.05). No differences in any of the variables investigated were found after salbutamol or placebo treatment.
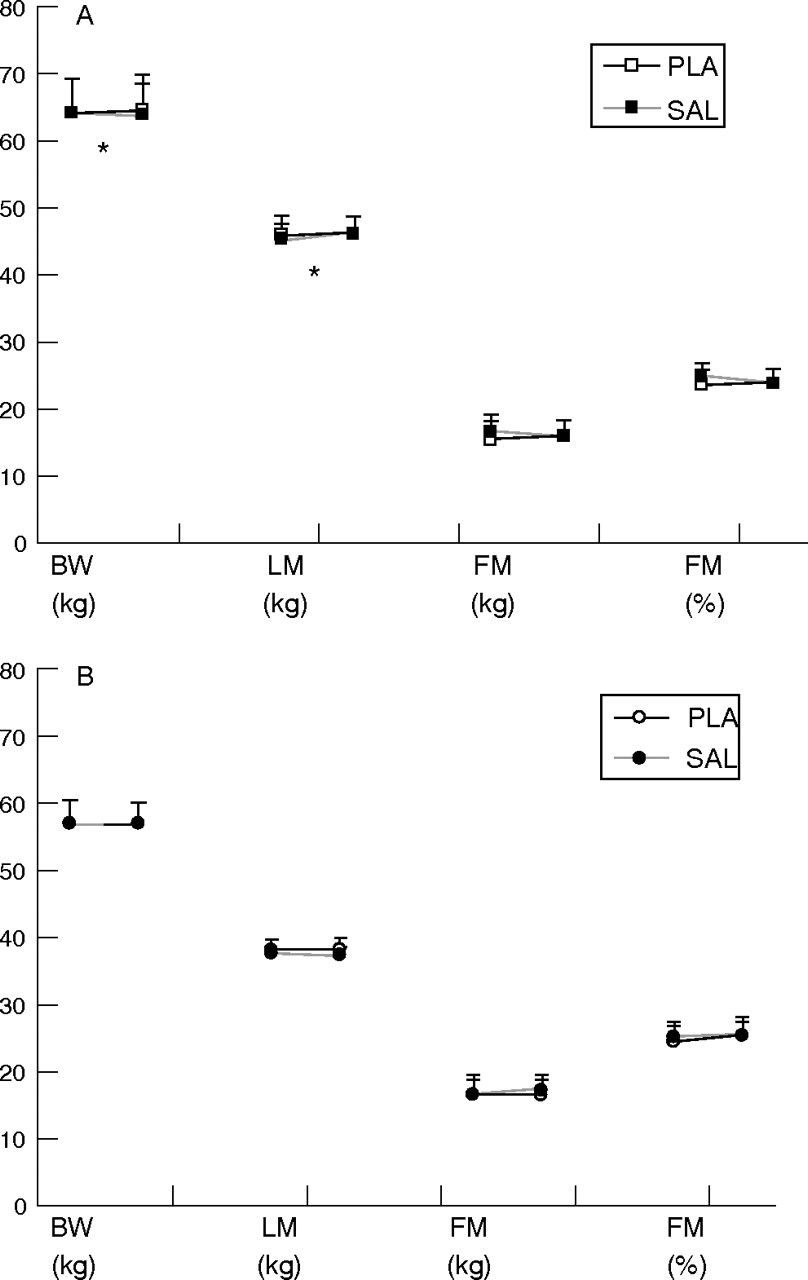
Body weight (BW, kg), lean mass (LM, kg), and fat mass (FM, kg and %) for trained (A) and untrained (B) subjects before and after placebo (PLA) and salbutamol (SAL) treatment. *Significant difference between trained and untrained subjects (p<0.05).
Bone densitometry
Table 2 shows BMD, BMDL, BMC, and BMCL values in the trained and untrained subjects. At the start of the study, the trained subjects had significantly higher BMD, BMC, and BMCL than the untrained subjects. There were no significant changes in any of these variables after either salbutamol or placebo treatment in the trained or untrained subjects.
Whole body and lumbar spine bone mineral density (BMD, BMDL) and content (BMC, BMCL) in trained and untrained subjects before and after placebo and salbutamol treatment
Blood lactate analysis
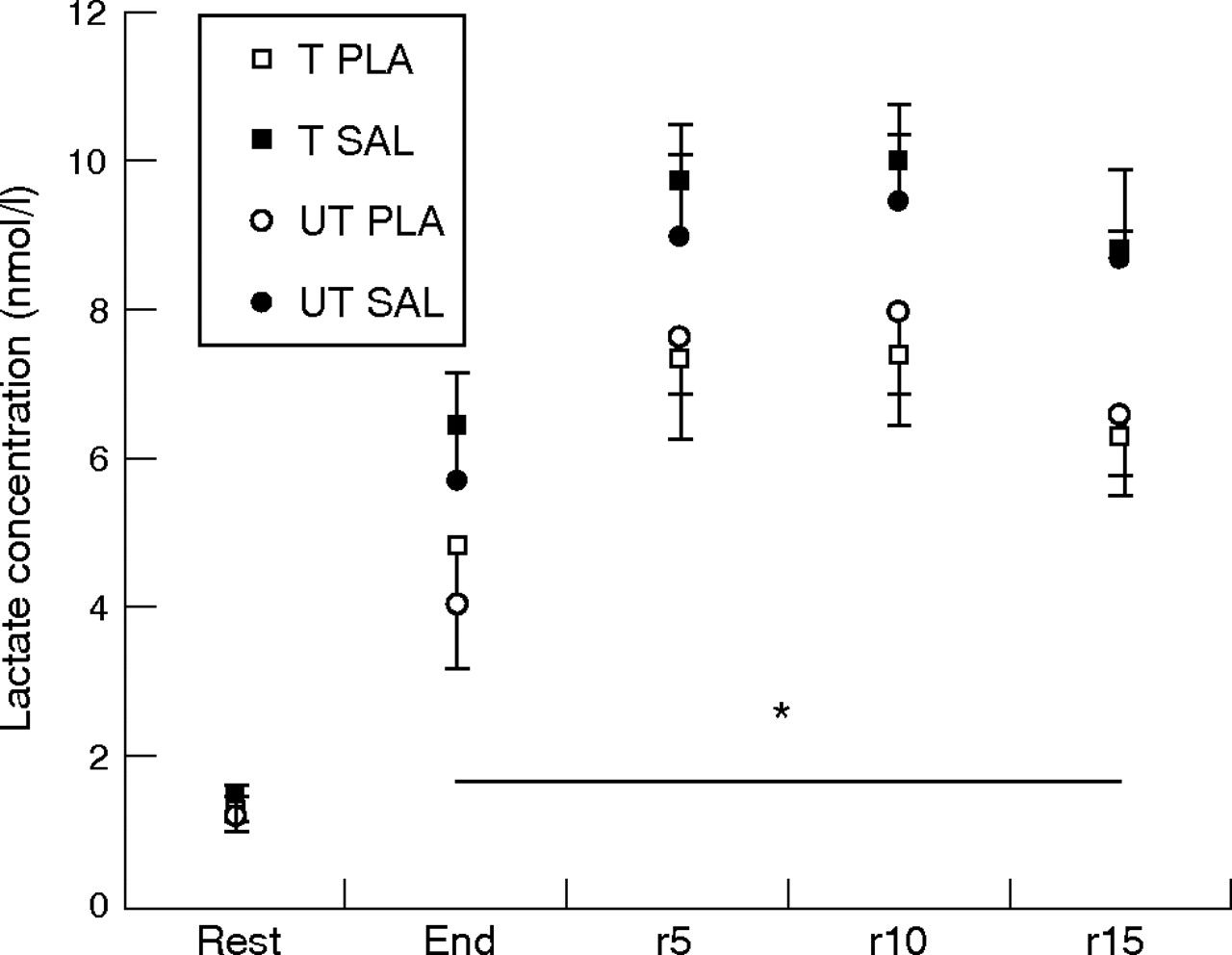
At the end of exercise and during recovery, blood lactate concentrations were significantly higher than the basal values (p<0.05) (fig 2). Salbutamol significantly increased blood lactate concentrations during recovery in all subjects (p<0.05).

{kind=link}
{kind=link}
Blood lactate concentration (mean (SEM)) at rest, at the end of exercise, and during passive recovery (after 5 (r5), 10 (r10), and 15 (r15) minutes) after placebo (PLA) and salbutamol (SAL) treatment in trained (T) and untrained (UT) subjects. *Significant difference between placebo and salbutamol (p<0.05).
DISCUSSION
Our results show that short term, therapeutic, systemic administration of salbutamol—that is, 12 mg/day for four weeks—improves peak power during supramaximal exercise in healthy sedentary and moderately trained female volunteers. No significant alterations in body composition or bone indices were observed with salbutamol treatment in either group during the trial.
The effects of resistance training on skeletal muscle has been studied previously.15 In agreement with the literature, we found a higher lean mass in the trained subjects than in the sedentary group. We found a parallel significantly higher body weight in the trained subjects without any significant difference in fat mass (total or %) between trained and untrained subjects. Four weeks of salbutamol intake at a therapeutic dose did not change any variables of body composition in the healthy women. Although clenbuterol, another β2 agonist, is known to stimulate muscle hypertrophy and reduce body fat,2,3,10 the anabolic effects of salbutamol and other β2 agonists remain equivocal. The different treatment effects may be due to different experimental conditions, such as species, dose, mode of administration, age, and sex.16,17 Hence, in animal studies, the anabolic effect of salbutamol on skeletal muscle was only found after intravenous administration with implanted minipumps,18 but never after oral administration in either animals or humans.2,19 Martineau et al4 found that salbutamol (16 mg/day for three weeks) did not affect lean body mass in healthy men. Another study examined the effect of a six week 16 mg daily salbutamol dose during a 9 week resistance training programme in healthy male subjects and also found that the drug did not modify muscle mass.5 In a recent study, the same authors6 investigated a 12 mg/day dose of salbutamol for two weeks. After 10 weeks of resistance training, similar results were obtained, but with a trend to a higher lean body mass with salbutamol. Finally, we tested in a previous study,7 the effects of salbutamol (12 mg/day for three weeks) on body composition in healthy male subjects and were unable to find any change in body composition, irrespective of the training status. In agreement with these previous studies on men, the present results also rule out any anabolic effect of oral salbutamol in healthy trained or untrained women.
Mechanical loading plays a major role in the development and maintenance of bone mass. Clinical and experimental studies have shown that moderate and repeated physical activity results in increased bone mass in both animals and humans.10 Mechanical loading influences bone mass through the strain it creates in bone tissue as a result of the strain itself, because of changes in streaming potentials, intralacunar pressure, and fluid flow, or through deformations in the extracellular matrix.10 Therefore it is logical that our trained subjects had significantly higher BMD, BMC, and BMCL than the untrained subjects. In this study, short term salbutamol administration did not have any effect on any of these variables in either group of subjects. These results initially appeared to contradict the few previous studies conducted with animals and humans. Indeed, some animal experiments showed that administration of β2 agonist, especially clenbuterol and salbutamol, leads to lower BMD, BMC, and mechanical resistance10–13. In contrast, in rats, β2 agonist administration attenuated bone loss resulting from hindlimb suspension.8,9 Only one study has investigated the effects of salbutamol on bone variables in humans. Caruso et al14 examined whether it could help resistance exercise to reduce unloading induced bone loss. Human subjects had their left legs suspended for 40 days, preventing normal ambulatory activity. While performing left leg strength training three days a week, the subjects concurrently received placebo or salbutamol (16 mg a day for 40 days). After 40 days, the resistance exercise/salbutamol assignment had induced significant gains in left leg BMC, whereas in the resistance exercise/placebo group, the mechanical loading data had significantly declined during the final unloading days compared with initial values. The authors concluded that the exercise/salbutamol assignment had probably increased BMC by maintaining the mechanical loading stimulus.
Different hypotheses can be proposed to explain the lack of effect of salbutamol on bone variables in our trained and untrained subjects. Firstly, human bone typically remodels in four to six month cycles. It is therefore doubtful that a four week treatment at a therapeutic dose would induce significant alteration in bone variables without an unloading induced bone loss. Indeed, our subjects did not suffer from any bone deficit, and Caruso et al14 estimate that salbutamol prescription combined with resistance exercise may mitigate the prevalence of osteoporosis and osteopenia. Secondly, as mentioned above, salbutamol did not seem to have any effect on body composition or leptin concentration,7,13 and it has been suggested that a leptin mediated effect on bone tissue seems likely. Anyway, it appears that a month of salbutamol treatment at a therapeutic dose in healthy women did not have any effect on bone tissue, irrespective of the training status. Further studies on humans are necessary to evaluate the potential beneficial and/or pathophysiological effects of a longer, chronic, systemic salbutamol treatment combined with exercise training.
The finding of an improvement in performance in our trained and untrained female subjects agrees with the results of Caruso et al5,6 and Martineau et al.4 Those authors showed an increase in voluntary muscle strength in humans after a comparable daily salbutamol dose, combined or not with a resistance training programme. In the same way, we found a significant improvement in peak power (about 10%) during a 30 second Wingate test in healthy male subjects after three weeks of salbutamol intake, irrespective of their training status. In agreement with this previous study, we found in female subjects a higher peak power after salbutamol compared with placebo during the Wingate test. Similarly, in view of the lack of change in body composition, the improvement in performance cannot result from an anabolic effect. Moreover, because we found the same increase in peak power in our two groups of subjects (about 9%), it seems that, as in men, the training status did not interact with the improvement in performance induced by salbutamol. Therefore it can be assumed that salbutamol has the same ergogenic effects in both sexes. However, further studies are necessary to clarify the mechanisms involved. Both peripheral and central effects may be suggested. Indeed, it has been postulated that β2 agonist administration results in greater calcium efflux5 from the sarcoplasmic reticulum in skeletal muscle, causing the formation of greater numbers of cross bridges and leading to glycogenolytic stimulation during this type of exercise. In agreement with this hypothesis, we found in the present study significantly higher recovery blood lactate concentrations after salbutamol in all subjects, which may reflect greater glycogenolysis.7 However, a central effect of salbutamol in this improvement in performance cannot be eliminated.20
What is already known on this topic
-
The effects of short term, systemic administration of salbutamol as an ergogenic aid during maximal or supramaximal exercise have been investigated, and also the effects of chronic salbutamol use on body composition and bone mineral, the latter with contradictory results
-
Whether this drug increases performance or muscle mass in women has yet to be determined
What this study adds
-
Short term, oral administration of salbutamol improved performance in sedentary and trained healthy female volunteers during supramaximal exercise
-
Short term, oral administration of salbutamol had no effect on body composition (lean and fat mass) or bone mineral measurements (bone mineral content and density), but increased blood lactate concentration in the period of recovery after supramaximal exercise in both trained and untrained subjects
In conclusion, the results of this study indicate that short term administration of salbutamol at therapeutic doses does not alter either body composition or bone variables but increases maximal anaerobic power in healthy female volunteers. The precise mechanisms of action remain to be elucidated.
Acknowledgments
This project was carried out with the support of CPLD. We express our gratitude to the subjects for their dedicated performance. We also thank the Hôpital de la Madeleine, Professor D Courteix, Mrs Corinne, Dr L Benhamou, and Dr M Ferry for their assistance. We gratefully acknowledge the expert technical assistance provided by Mr Régis Bonnefoy.
REFERENCES
Footnotes
-
Published Online First 10 May 2006
-
Competing interests: none declared