
Abstract
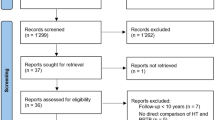
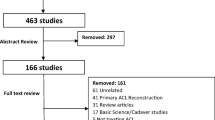
Following a bone-patellar tendon-bone autograft (BPTB) or four-stranded semitendinosus/gracilis tendons autograft (ST/G) anterior cruciate ligament (ACL) reconstruction, the speed and safety with which an athlete returns to sports (or regains the pre-injury level of function) depends on the rehabilitation protocol. Considering the large differences in clinical and outpatient protocols, there is no consensus regarding the content of such a rehabilitation program. Therefore, we conducted a systematic review to develop an optimal evidence-based rehabilitation protocol to enable unambiguous, practical and useful treatment after ACL reconstruction. The systematic literature search identified 1,096 citations published between January 1995 and December 2006. Thirty-two soundly based rehabilitation programs, randomized clinical trials (RCT’s) and reviews were included in which common physical therapy modalities (instruction, bracing, cryotherapy, joint mobility training, muscle-strength training, gait re-education, training of neuromuscular function/balance and proprioception) or rehabilitation programs were evaluated following ACL reconstruction with a BPTB or ST/G graft. Two reviews were excluded because of poor quality. Finally, the extracted data were combined with information from background literature to develop an optimal evidence-based rehabilitation protocol. The results clearly indicated that an accelerated protocol without postoperative bracing, in which reduction of pain, swelling and inflammation, regaining range of motion, strength and neuromuscular control are the most important aims, has important advantages and does not lead to stability problems. Preclinical sessions, clear starting times and control of the rehabilitation aims with objective and subjective tests facilitate an uncomplicated rehabilitation course. Consensus about this evidence-based accelerated protocol will not only enhance the speed and safety with which an athlete returns to sports, but a standardized method of outcome measurement and reporting will also increase the evidential value of future articles.
Similar content being viewed by others

References
Allum R (2003) Aspects of current management, complications of arthroscopic reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 85-B:12–16
Beynnon B, Benjamin S, Johnson R, Abate J, Nichols C, Fleming B et al (2005) Rehabilitation after anterior cruciate ligament reconstruction, a prospective, randomized, double-blind comparison of programs administered over 2 different time intervals. Am J Sports Med 33:347–359
Beynnon B, Johnson R, Abate J, Fleming B, Nichols C (2005) Treatment of anterior cruciate ligament injuries, Part I. Am J Sports Med 33:1579–1602
Beynnon B, Johnson R, Abate J, Fleming B, Nichols C (2005) Treatment of anterior cruciate ligament injuries, Part 2. Am J Sports Med 33:1751–1767
Beynnon B, Johnson R, Fleming B (2002) The science of anterior cruciate ligament rehabilitation. Clin Orthop 402:9–20
Cascio B, Culp L, Cosgarea A (2004) Return to play after anterior cruciate ligament reconstruction. Clin Sports Med 23:395–408
Cooper R, Taylor N, Feller J (2005) A randomised controlled trial of proprioceptive and balance training after surgical reconstruction of the anterior cruciate ligament. Res Sports Med 13:217–230
DeHaven K, Cosgarea A, Sebastianelli W (2003) Arthrofibrosis of the knee following ligament surgery. Instr Course Lect 52:369–381
Fleming B, Oksendahl H, Beynnon B (2005) Open- or closed kinetic chain exercises after anterior cruciate ligament reconstruction. Exerc Sport Sci Rev 33:134–140
Frosch KH, Habermann F, Fuchs M, Michel A, Schmidtmann U, Stürmer K (2001) Ist die erweiterte ambulante physiotherapie (EAP) nach vorderer kruezbandersatzplastik indiziert. Unfallchirurg 104:513–518
Gale T, Richmond J (2006) Bone patellar tendon bone anterior cruciate ligament reconstruction. Tech Knee Surg 5:72–79
Goldblatt J, Fitzsimmons S, Balk E, Richmond J (2005) Reconstruction of the anterior cruciate ligament, meta-analysis of patellar tendon versus hamstring tendon autograft. Arthroscopy 21:791–803
Harilainen A, Sandelin J (2006) Post-operative use of knee brace in bone-tendon-bone patellar tendon anterior cruciate ligament reconstruction, 5-year follow-up results of a randomized prospective study. Scand J Med Sci Sports 16:14–18
Haverkamp D, Sierevelt I, Breugem S, Lohuis K, Blankevoort L, Dijk CN (2006) Translation and validation of the Dutch version of the international knee documentation committee subjective knee form. Am J Sports Med 34:1680–1684
Heijne A, Werner S (2007) Early versus late start of open kinetic chain quadriceps exercises after ACL reconstruction with patellar tendon or hamstring grafts, a prospective randomized outcome study. Knee Surg Sports Traumatol Arthosc 15:402–421
Henriksson M, Rockborn P, Good L (2002) Range of motion training in brace versus plaster immobilization after anterior cruciate ligament reconstruction, a prospective randomized comparison with a 2-year follow up. Scand J Med Sci Sports 12:73–80
Hooper D, Morrissey M, Drechsler W, Morrissey D, King J (2001) Open and closed kinetic chain exercises in the early period after anterior cruciate ligament reconstruction. Am J Sports Med 29:167–174
Insall JN, Scott WN (2001) Surgery of the knee. 3rh edn. Volume 1. Churchill Livingstone, New York
Keating J, Matyas T (1996) The influence of subject and test design on dynamometric measurements of extremity muscles. Phys Ther 76:866–889
Lahav A, Burks R (2005) Evaluation of the failed ACL reconstruction. Sports Med Arthrosc Rev 13:8–16
Liu-Ambrose T, Taunton J, MacIntyre D, McConkey P, Khan K (2003) The effects of proprioceptive or strength training on the neuromuscular function of the ACL reconstructed knee, a randomized clinical trial. Scand J Med Sci Sports 13:115–123
Maddison R, Prapavessis H, Clatworthy M (2006) Modelling and rehabilitation following anterior cruciate ligament reconstruction. Ann Behav Med 31:89–98
Majima T, Yasuda K, Tago H, Tanabe Y, Minami A (2002) Rehabilitation after hamstring anterior cruciate ligament reconstruction. Clin Orthop 397:370–380
Mc Carty L, Bach B (2005) Rehabilitation after patellar tendon autograft anterior cruciate ligament reconstruction. Tech Orthop 20:439–451
Meyers M, Sterling J, Marley R (2002) Efficacy of stairclimber versus cycle ergometry in postoperative anterior cruciate ligament rehabilitation. Clin J Sport Med 12:85–94
Mikkelsen C, Cerulli G, Lorenzini M, Bergstrand G, Werner S (2003) Can a post-operative brace in slight hyperextension prevent extension deficit after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthosc 11:318–321
Mikkelsen C, Werner S, Eriksson E (2000) Closed kinetic chain alone compared to combined open and closed kinetic chain exercises for quadriceps strengthening after anterior cruciate ligament reconstruction with respect to return to sport, a prospective matched follow-up study. Knee Surg Sports Traumatol Arhrosc 8:337–342
Möller E, Forssblad M, Hansson L, Wange P, Weidenhielm L (2001) Bracing versus nonbracing in rehabilitation after anterior cruciate ligament reconstruction, a randomized prospective study with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 9:102–108
Morrissey M, Drechsler W, Morrissey D, Knight P, Armstrong P, McAuliffe T (2002) Effects of distally fixated versus nondistally fixated leg extensor resistance training on knee pain in the early period after anterior cruciate ligament reconstruction. Phys Ther 82:35–43
Morrissey M, Hudson Z, Drechsler W, Coutts F, Knight P, King J (2000) Effects of open versus closed kinetic chain training on knee laxity in the early period after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 8:343–348
O’Connor D, Laughlin M, Woods G (2005) Factors related to additional knee injuries after anterior cruciate ligament injury. Arthroscopy 21:431–438
Perry M, Morrissey M, King J, Morrissey D, Earnshaw P (2005) Effects of closed versus open kinetic chain knee extensor resistance training on knee laxity and leg function in patients during the 8- to 14-week post-operative period after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 13:357–369
Pförringer W, Kremer C (2005) Die nachbehandlung operativ versorgter frischer vordere kreuzbandrupturen, eine randomisierte prospective studie. Sportverletz Sportschaden 19:134–139
Pinczewski L, Lyman J, Salmon L, Russell V, Roe J, Linklater J (2007) A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft, a controlled, prospective trial. Am J Sports Med 35:564–574
Plas C, Dingjan R, Hamel A et al. (1998) Nederlands Huisartsen Genootschap standaard traumatische knieproblemen M66. Available via DIALOG. http://nhg.artsennet.nl/upload/104/standaarden/M66/std.htm. Accessed June 1998
Potter N (2006) Complications and treatment during rehabilitation after anterior cruciate ligament reconstruction. Oper Tech Sports Med 14:50–58
Raynor M, Pietrobon R, Guller U, Higgins L (2005) Cryotherapy after ACL reconstruction. J Knee Surg 18:123–129
Rebel M (2000) Koordinatives training nach VKB-operationen. Sportverletz Sportschaden 14:12–19
Risberg M, Holm I, Steen H, Eriksson J, Ekeland A (1999) The effect of knee bracing after anterior cruciate ligament reconstruction, a prospective, randomized study with two years follow up. Am J Sports Med 27:76–83
Risberg M, Lewek M, Snyder-Mackler L (2004) A systematic review of evidence for anterior cruciate ligament rehabilitation, how much and what type. Phys Ther Sport 5:125–145
Risberg M, Mork M, Jenssen H, Holm I (2001) Design and implementation of a neuromuscular training program following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 31:620–631
Ross M, Denegar C, Winzenried J (2001) Implementation of open and closed kinetic chain quadriceps strengthening exercises after anterior cruciate ligament reconstruction. J Strength Cond Res 15:466–473
Shaw T (2002) Accelerated rehabilitation following anterior cruciate ligament reconstruction. Phys Ther Sport 3:19–26
Shaw T, Chipchase L, Williams M (2004) A users guide to outcome measurement following reconstruction. Phys Ther Sport 5:57–67
Shaw T, Williams M, Chipchase L (2005) Early quadriceps exercises affect the outcome of ACL reconstruction, a randomised controlled trial. Aust J Physiother 51:9–17
Shelbourne K, Patel D (1999) Treatment of limited motion after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthosc 7:85–92
Strehl A, Eggli S (2007) The value of conservative treatment in ruptures of the anterior cruciate ligament (ACL). J Trauma 62:1159–1162
Tandogan R, Taser O, Kayaalp A et al (2004) Analysis of meniscal and chondral lesions accompanying anterior cruciate ligament tears, relationship with age, time from injury, and level of sport. Knee Surg Sports Traumatol Arthrosc 12:262–270
Trees A, Howe T, Dixon J, White L (2005) Exercise for treating isolated anterior cruciate ligament injuries in adults (review). Cochrane Database Syst Rev 4:1–41
Tsaklis P, Abatzides G (2002) ACL rehabilitation program using a combined isokinetic and isotonic strengthening protocol. Isokinet Exerc Sci 10:211–219
Wilk K, Reinold M, Hooks T (2003) Recent advances in the rehabilitation of isolated and combined anterior cruciate ligament injuries. Orthop Clin North Am 34:107–137
Wu G, Ng G, Mak A (2001) Effects of knee bracing on the sensorimotor function of subjects with anterior cruciate ligament reconstruction. Am J Sports Med 29:641–645
Acknowledgments
We thank Anne Benjaminse, PT, MSc for her translation efforts.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendices
Appendix 1: Rehabilitation protocol following ACL reconstruction (BPTB and ST/G method)
Presurgery
Preferably patients will be seen by the physical therapist at least three times presurgically. In these sessions, the following will be considered:
-
Information about the rehabilitation (discuss mutual expectations). Emphasize that knee rehabilitation is more than strength-training of the upper-leg muscles alone. The (neuromuscular) rehabilitation addresses the whole lower extremity, core stability and training of the kinetic chain.
-
Decrease of pain, swelling and inflammation.
-
Achieve/maintain normal range of motion (ROM) with a focus on good patellar mobility.
-
Achieve/maintain normal gait pattern.
-
Maintain muscle strength, prevent atrophy.
-
Training of the first-days postoperative exercises (i.e., heel slides, straight-leg raising (SLR), squads, leg elevation with a pillow under the heel). Emphasize the importance of full extension.
-
Practice alternate walking with crutches for the first days postoperatively.
-
Tests: VAS-score pain; ROM; measurement of knee swelling; IKDC questionnaire; hop tests and optional isokinetic tests for strength and endurance of the knee flexors and extensors.
Phase 1 (week 1)
-
Control of pain and inflammation (i.e., through cryotherapy and exercises).
-
Obtain ROM of 0º–90º, emphasizing achievement of full extension (i.e., through CPM and exercises: patellar mobilization in all directions, heel slides and leg elevation with a pillow under the heel).
-
Regain muscle control, with safe isometric and isotonic OC (ROM 90º–40º) and CC (ROM 0º–60º) strength exercises without additional weight. (i.e., SLR, mini squads, shifting body weight).
-
Improve gait pattern. If pain is tolerated, aim at walking without crutches from day 4. Sufficient neuromuscular control and a non-limping gait pattern are criteria for walking without crutches.
Criteria to start with phase 2
-
Pain knee is equal to previous week or less (VAS-score pain).
-
Minimal swelling (measurement with measuring tape).
-
Full extension and 90º flexion are possible (ROM-goniometer).
-
Good patellar mobility compared with contralateral side.
-
Sufficient quadriceps control to perform a mini squad 0º–30º and SLR in multiple directions.
-
Ability to walk independently with or without crutches.
Phase 2 (week 2 to week 9)
-
Apply cryotherapy in case of pain or swelling (if necessary after each therapy session).
-
Work toward full ROM (maintain full extension, 120º flexion from week 2 and 130º flexion from week 5) with remaining attention for good patellar mobility.
-
Walking without crutches from day 4 to 10. Normalize gait pattern with walking exercises (treadmill from week 3 and jogging in a straight line from week 8).
-
Isometric and isotonic strength training increasing in intensity (quadriceps, hamstring, gastrocnemius and soleus), with increasing ROM for OC and CC exercises without extra weight. For OC exercises: weeks 2, 3 and 4 from 90° to 40°, afterward 10° toward extension to be added every week. For CC exercises: weeks 2–7 from 0° to 60° and from week 8 from 0° to 90°.
-
Start neuromuscular training by slowly increasing from static stability to dynamic stability. Work toward confidence on the vestibular and somatosensory system for balance, with increasing surface instability and decreasing visual input.
-
Start from week 3 with cycling on an ergometer and swimming.
-
Start from week 4 with stepping on a stair-stepping machine.
-
Start from week 8 with outdoor cycling.
Caution: act adequately in case of persisting pain, inflammation or limited ROM → there is a risk of developing arthrofibrosis (in case of doubt consult the orthopedic surgeon)!
Criteria to start with phase 3
-
Minimal pain and swelling (VAS-score pain, measurement of knee swelling with measuring tape).
-
Full extension and at least 130º flexion possible (ROM-goniometer).
-
Normal gait pattern.
-
Exercises of previous week are carried out properly.
-
Administer the IKDC questionnaire.
Phase 3 (week 9 to week 16)
-
Obtaining and maintaining full ROM.
-
Optimizing muscle strength and endurance. Add increasing weights from week 9 both for OC and CC exercises.
-
Neuromuscular training with increasing emphasis on dynamic stability and plyometric exercises, slowly increasing duration and speed. Start with two-legged jumping and work slowly toward one-legged jumping. Normalize running with outdoor jogging from week 13.
Criteria to start with phase 4
-
No pain or swelling in the knee (VAS-score pain, measuring knee swelling with measuring tape).
-
Full flexion and extension of the knee (ROM-goniometer).
-
Administer the IKDC questionnaire again.
-
Quadriceps and hamstring strength >75% compared to the contralateral side. Difference in hamstring/quadriceps strength ratio is ≤15% compared to the contralateral side (optional isokinetic strength testing of knee flexors and extensors at 180º per second).
-
Hop tests >75% compared to the contralateral side.
-
Exercises of previous week are carried out properly.
Phase 4 (week 16 to week 22)
-
Maximizing muscle endurance and strength.
-
Maximizing neuromuscular control with emphasis on jumping, agility training and sport-specific tasks. Variations in running, turning and cutting maneuvers are allowed. Duration and speed to be increased and maximized.
Criteria for returning to sports
-
No pain or swelling (VAS-score pain, measuring knee swelling with measurement tape).
-
Full flexion and extension of the knee is possible (ROM-goniometer).
-
Quadriceps and hamstring strength >85% compared to the contralateral side. Difference in hamstring/quadriceps strength ratio is <15% compared to the contralateral side (optional isokinetic strength testing of knee flexors and extensors at 60°, 180° and 300° per second and an endurance test at 180° per second).
-
Hop tests > 85% compared to the contralateral side.
-
Exercises of previous week are carried out properly, and the patient tolerates sport-specific activities and agility training with maximal duration and speed.
-
Administer the IKDC questionnaire again.
Appendix 2: overview of tests




Rights and permissions
About this article
Cite this article
van Grinsven, S., van Cingel, R.E.H., Holla, C.J.M. et al. Evidence-based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 18, 1128–1144 (2010). https://doi.org/10.1007/s00167-009-1027-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-009-1027-2