Article Text

Abstract
Objectives The size and shape of a joint cavity are the key determinates for the mobility of the joint. The anatomy and configuration of the facet joint (FJ) recesses at different levels of the spine remain unclear and controversial. The aim of this study was to identify the configuration of the FJ recesses in the cervical, thoracic and lumbar spine using a combination of micro-CT and sheet plastination techniques.
Methods Of 19 cadavers (9 males, 10 females, age range of 54–89 years), the FJ cavities of 3 spines were injected with contrast filling and scanned with micro-CT, and 16 plastinated spines were prepared as the series of sagittal (9 sets), transverse (5 sets) or coronal (2 sets) sections with a thickness of 2.5 mm and examined under a stereoscopic microscope.
Results This study characterised the FJ spaces and recesses of the spine and found that (1) the configuration and extent of the FJ recesses varied along the spine. The optimal needle approach to the FJ cavity was via an anterolateral or posterolateral recess at the cervical level, along the tip of the inferior articular process at the thoracic level and via the posteromedial recess at the lumbar level. (2) The FJ cavity did not communicate with the retrodural space.
Conclusion The anatomical features of the FJ recesses at different levels of the spine confirm no direct communication between the FJ cavity and retrodural space.
- facet joint recess
- spine
- micro-CT
- anatomy
- epoxy sheet plastination
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Anatomy of the facet joint (FJ), or zygapophyseal joint, of the spine has been extensively studied but less attention is paid to the joint cavity,1–4 which is one of the key determinates for the mobility of a joint.5–7 Using arthrography to visualise a FJ cavity was explored at the lumbar spine and indicated that its small and irregular articular cavity posed a problem to directly insert the needle into the cavity.8–10
The FJ cavity can be divided into two portions: the FJ space between the articular cartilages of two opposing facets, and FJ recesses extending peripherally beyond the edges of the articular cartilage. It has been suggested to use the FJ recesses to maximise access to the FJ cavity.9 11–13 However, the anatomy and configuration of the FJ recesses at different levels of the spine remain unclear and controversial.14 15 At the lumbar spine, for example, the inferior FJ recess has been reported to have an opening to communicate with the extracapsular fat,16 whereas the superior FJ recess communicates with the intervertebral foramen via an opening along the lateral aspect of the recess.17 18 At the cervical spine, Okada stated that 80% of the FJs communicated with the interlaminar and interspinous regions and contralateral FJs via an extradural space dorsal to the ligamentum flavum.18 19 Anatomical evidence for the above reports is lacking. The aim of this study was to identify and localise three-dimensional (3D) configuration of the FJ recesses in the cervical, thoracic and lumbar spine using a combination of epoxy sheet plastination and micro-CT scanning technologies.
Material and methods
A total of 19 cadaveric spines were used in this study, 16 for epoxy sheet plastination and 3 for micro-CT scans. None of the cadavers had previous surgical intervention and physical abnormalities, but facet degeneration of the specimens was not excluded. The cadavers were bequeathed for medical education and research purposes under the Human Tissues Act. Individual FJs of the spine were abbreviated as C1/2, C2/3, …, L3/4 and L4/5, respectively, in this study.
Epoxy sheet plastination
Sixteen plastinated spines (seven males and nine females, age range of 54–89 years) were prepared as sagittal (nine sets), transverse (five sets) or coronal (two sets) sections. The plastination procedure was performed as previously described.20 In brief, the whole spine was frozen at −80°C for 5 days and cut with a band-saw into serial sections. The thickness of a section was 2.5 mm and the interval between two adjacent sections was 0.88 mm. To minimise tissue shrinkage, the sections were slowly dehydrated in cold acetone at −30°C for 3 weeks, followed by degreasing in acetone at 22°C–24°C for 2 weeks, then impregnated with an epoxy resin mixture of E12/E6/E600 (Biodur, Heidelberg, Germany) at 0°C for 2 days and cured at 45°C for 5 days.
The plastinated sections were examined under a Leica MZ8 stereoscopic microscope (Leica, Heerbrugg, Switzerland). In a plastinated section, the FJ spaces and recesses were real spaces, whereas other potential spaces, such as retrodural space and subsynovial area, were occupied by transparent adipose tissue which was identifiable under a microscope.
Micro-CT scans
Three cadaveric spines (two males, one female, age range of 74–81 years) were used for micro-CT scanning. The FJs with the intact capsule were carefully dissected and fully visualised. After the FJ space was palpated, a 25G needle was placed into the space at the posteroinferior aspect of the joint. A mix of barium sulfate suspension (E-Z-EM Canada, New York, USA) and blue-coloured latex (1:1 parts by weight) was injected into the FJ cavity. Amount of the contrast filling varied in different FJs, for example, more in the cervical FJs and lesser in the thoracic FJs. Post-micro-CT scanning dissection was performed to verify the distribution of the contrast filling in the FJ cavity and to correlate with the micro-CT 3D renderings.
Results
The FJ recesses of the cervical FJ
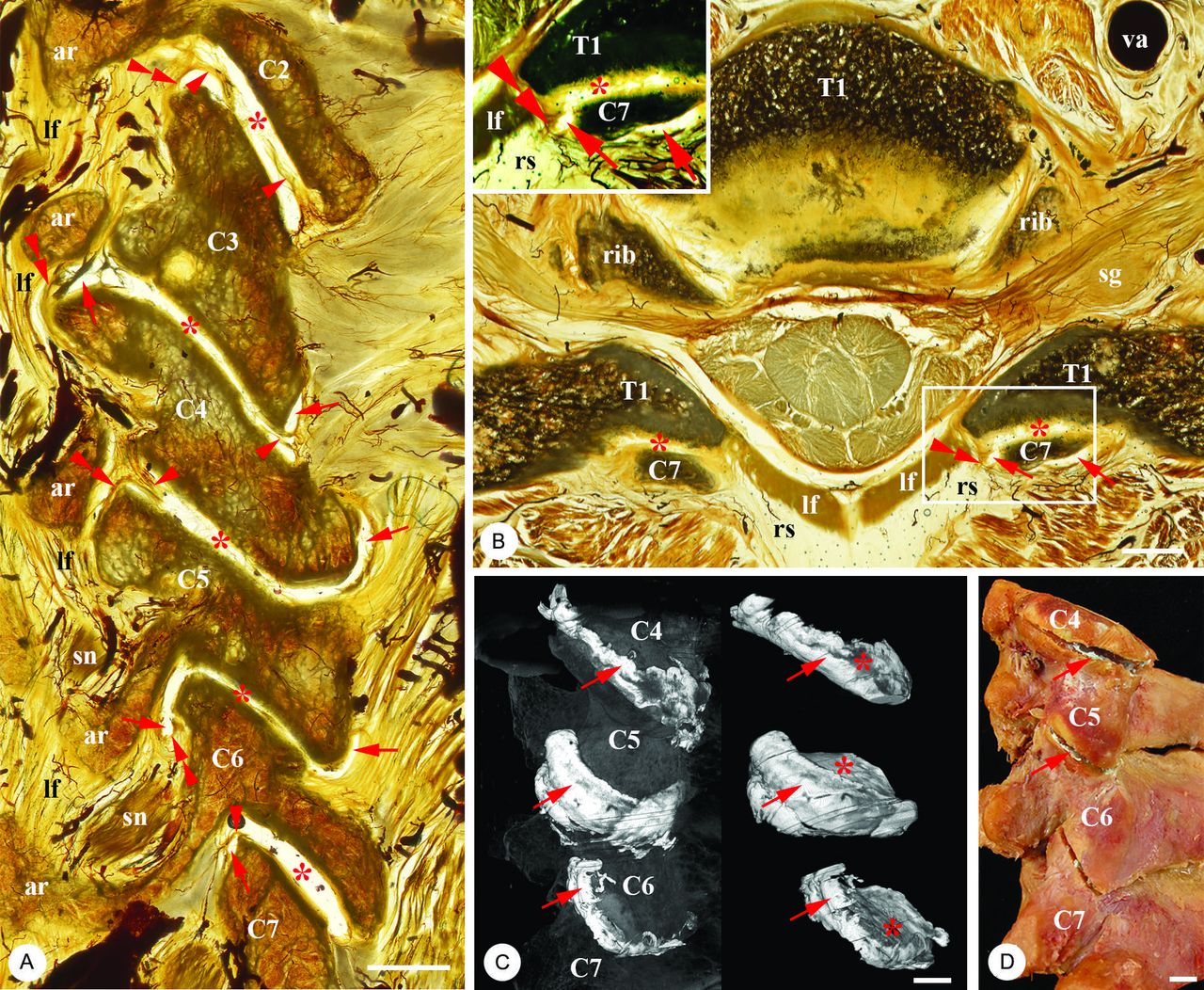
The FJ recesses of the cervical FJ lipped almost fully around the FJ space, with larger recesses on the anterolateral and posterolateral edges of the facet (figure 1A–D). The anterolateral recess extended inferiorly and was bordered by a layer of the joint capsule neighboured by the retrodural space which was a potential space and contained adipose tissue, spinal nerve and vessels, posterior to the ligamentum flavum (figure 1A,B and inset). The posterolateral recess extended superiorly (figure 1A) and its capsule wall was enhanced by the tendinous fibres from the deep cervical muscles (figure 1A,B). The synovial folds from the anterior or posterior capsule protruded into the cavity (figure 1A).

The facet joint (FJ) recesses at C2–C7 levels. (A) Sagittal view of the FJ spaces (asterisks) and recesses (arrows) of the C2–C7 FJ cavities. Arrowheads point to the synovial folds. Double arrowheads point to the synovial capsule dorsal to the lf which attaches to the vertebral ar. (B) Transverse view of the spaces (asterisks) and recesses (arrows) of the inferior part of the C7/T1 FJ cavity. The inset is a phase-contrast view of the line box in (B), showing that the FJ capsule (double arrowheads) separates the FJ recess (arrows; a real space) from the rs (an adipose potential space) which lies dorsal to the lf. (C) Lateral views of the three-dimensional reconstruction model of the recesses (arrows) and spaces (asterisks) of the C4–C7 FJ cavities with and without vertebrae. (D) Lateral view of a cadaveric specimen showing the partially opened C4–C7 FJ cavities (arrows) with the contrast filling after micro-CT scanning (C). ar, arch; C2–T1, the order of the vertebrae; lf, ligamentum flavum; rs, retrodural space; sg, spinal ganglion; sn, spinal nerve; va, vertebral artery. Bars, 5 mm.
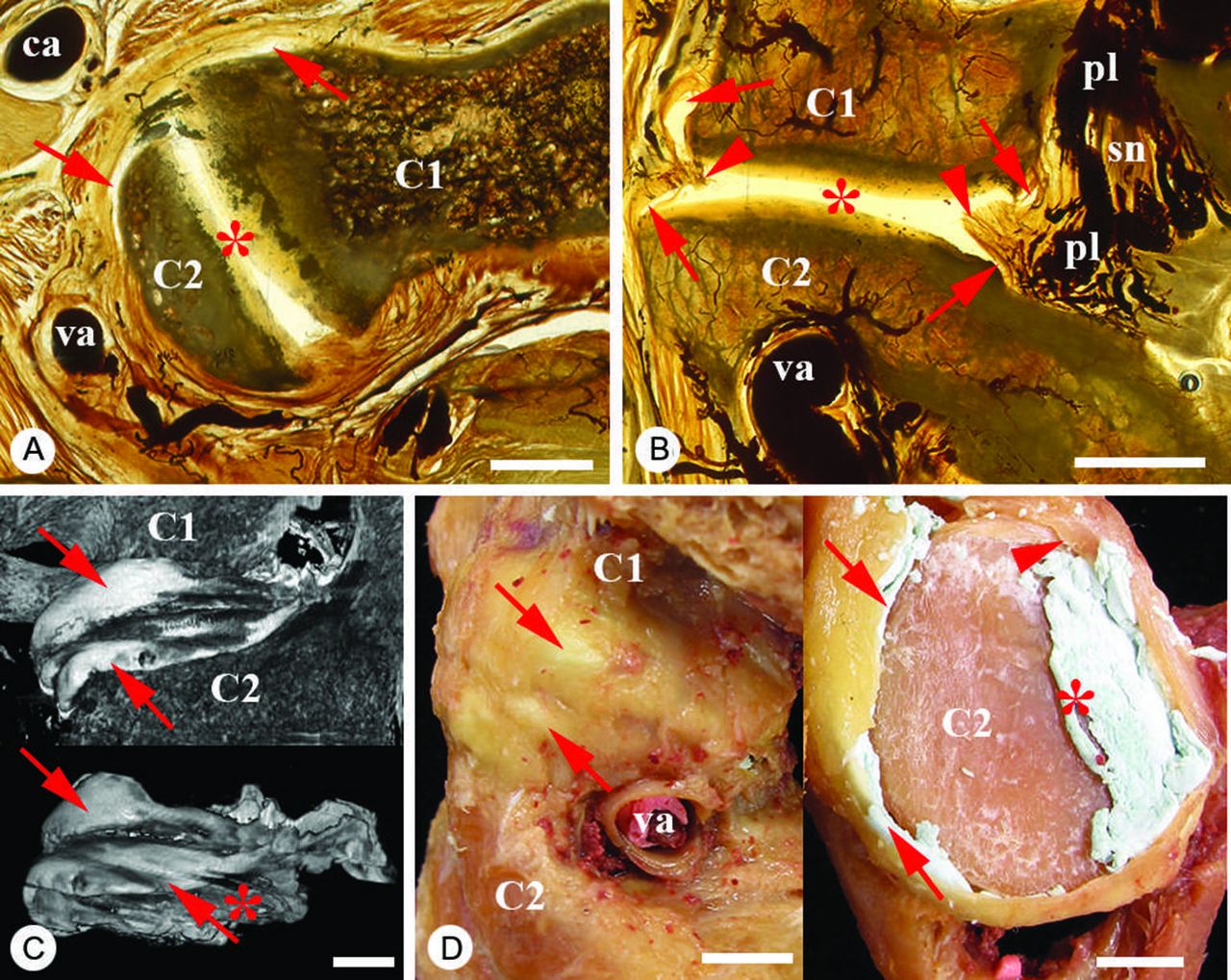
Of the cervical FJs, the C1–C2 joint was unique (figure 2A–D) and had a relatively horizontal FJ space (figure 2C) and an abundance of FJ recesses (figure 2A–D). The recesses wrapped superiorly or inferiorly around the edges of the superior and inferior facets, with particularly large anterosuperior and anteroinferior recesses (figure 2B,C). The capsule wall of the recesses was supported by fibrous tissue (figure 2A,B), and posteriorly neighboured by a very rich venous plexus and the spinal nerve (figure 2B). Synovial folds protruded into the cavity (figure 2B).

The C1/C2 facet joint (FJ) recesses. (A) Transverse view of the space (asterisk) and recesses (arrows) of a left C1/C2 FJ cavity. (B) Sagittal view of the space (asterisk) and recesses (arrows) of the C1/C2 FJ cavity. Arrowheads point to the synovial folds. Note the pl and sn posterior to the FJ cavity. (C) Lateral views of the three-dimensional reconstruction model of the recesses (arrows) and space (asterisk) of a C1/C2 FJ cavity with and without the vertebrae after micro-CT scanning. (D) The intact and opened C1/C2 FJ specimen after a contrast filling injection and micro-CT scanning (C). Arrows point to the FJ recesses and asterisk indicates the FJ space. C1–C2, the first and second cervical vertebrae; ca, carotid artery; pl, vascular plexus; sn, spinal nerve; va, vertebral artery. Bars, 5 mm.
The FJ recesses of the lumbar FJ
The lumbar FJ had a vertical ovoid FJ space and large anteromedial and posteromedial FJ recesses (figure 3A–D). The anteromedial recess extended superiorly slightly beyond the upper edge of the superior articular process of the lower vertebra (figure 3A), whereas the posteromedial recess wrapped around the lower lip of the inferior articular process of the upper vertebra (figure 3A,B). The capsule wall of the anteromedial recess was strongly supported by the ligamentum flavum (figure 3B). Posterior to the ligamentum flavum but exterior to the synovial membrane was the retrodural space which was occupied by adipose tissue. The fibrous capsule of the posteromedial recess attached to the articular processes, and synovial folds deeply protruded into the FJ space (figure 3A,B).
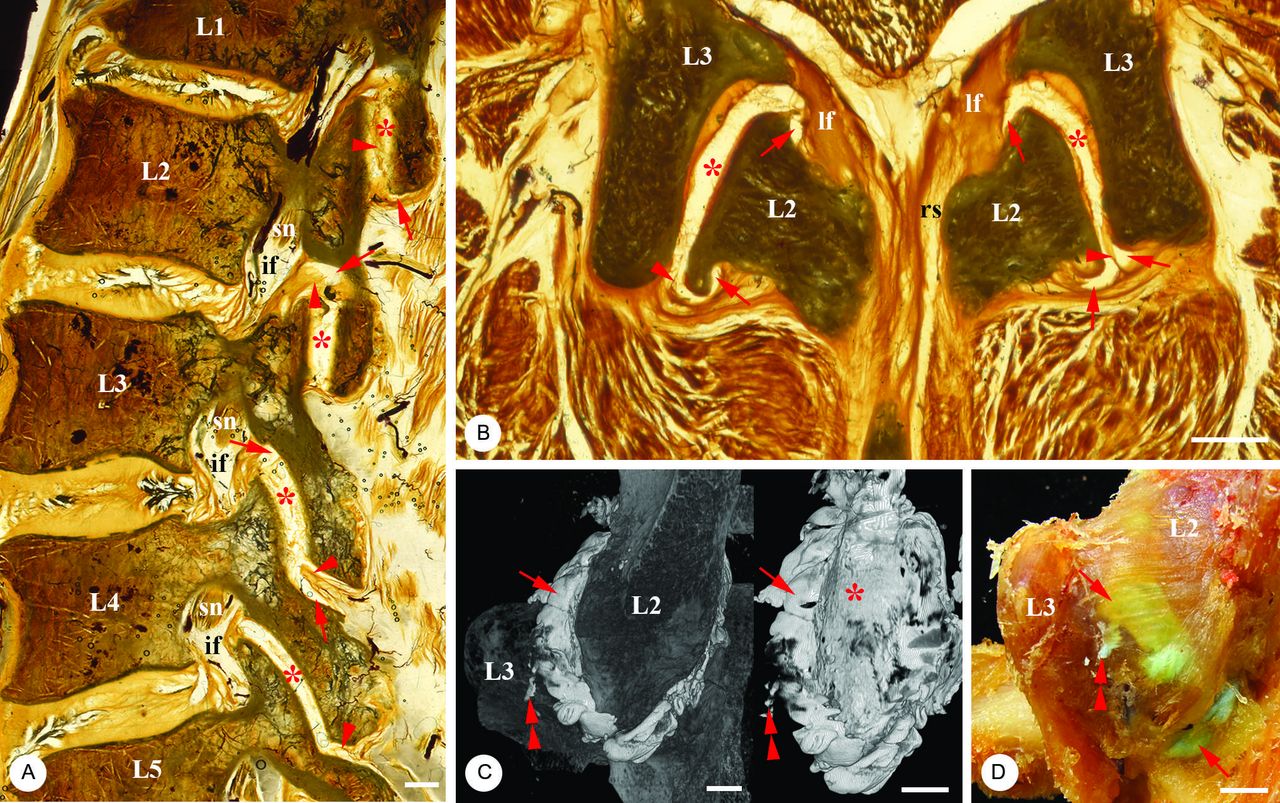
The facet joint (FJ) recesses at L1–L5 levels. (A) Sagittal view of the spaces (asterisks) and recesses (arrows) of the L1–L5 FJ cavities. Arrowheads point to the synovial folds. The spinal nerve (sn) is anterior and superior to the FJ and in the intervertebral foramen (if). (B) Transverse view of the spaces (asterisks) and recesses (arrows) of the L2/L3 FJ cavity. Arrowheads point to the synovial folds. Retrodural space (rs) is posterior to the ligamentum flavum (lf). (C) Posterior views of the three-dimensional reconstruction model of the space (asterisk) and recesses (arrows) of the L2/L3 FJ cavity in D with and without the vertebrae. Double arrowheads point to the contrast filling injection site. (D) Posterior view of the L2/L3 FJ specimen after contrast filling injection (double arrowheads). Arrows point to the recesses. L1–L5, the order of the vertebrae. Bars, 5 mm.
The FJ recesses of the thoracic FJ
The thoracic FJ had an anteromedial and an inferior FJ recess (figure 4A–D). The recesses were small and extended superiorly or inferiorly slightly beyond the tip of the articular process (figure 4A). The shape of the recesses at the upper and lower thoracic levels was similar to that at the lower cervical (figure 1) and upper lumbar levels (figure 3), respectively. The ligamentum flavum and fibrous capsule provided strong support for the capsular wall of the recesses (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The facet joint (FJ) recesses at T11–L1 levels. (A) Sagittal view of the spaces (asterisks) and recesses (arrows) of the T11–L1 FJ cavities. (B) Transverse view of the spaces (asterisks) and recesses (arrows) of the T12/L1 FJ cavities. Arrowhead points to the synovial fold. Retrodural space (rs) is posterior to the ligamentum flavum (lf). Double arrowheads point to the saw dust. (C) Posterior views of the three-dimensional reconstruction model of the space (asterisk) and recesses (arrows) of the T12/L1 FJ cavity with and without the vertebrae. Double arrowheads point to the injection site. (D) Posterior view of the space (asterisk) and recess (arrow) of the opened T12/L1 FJ (C) after contrast filling injection (double arrowheads) and micro-CT scanning. T11–L1, the order of the vertebrae; Bars, 5 mm.
Discussion
This study characterises the FJ spaces and recesses of the whole cadaveric spine and reveals anatomical features and 3D configurations of the FJ recesses at the cervical, thoracic and lumbar levels of the spine. The main findings of this study include that the configuration and extent of the FJ recesses varied at different levels of the spine, and the FJ cavity did not communicate with the retrodural space.
Features of the FJ recesses
This study demonstrated that although the orientation and shape of the FJ spaces were dictated by facet articular surfaces, the anatomical features of the FJ recesses varied significantly at different levels of the spine. The FJ recesses were not always redundancies along the superior and inferior-most aspects of the FJs as stated in the literature.3 12 For example, at the cervical level, the majority of the FJ cavities (C2–C7) can be accessed via a posterolateral recess just above the tip of the inferior articular process, whereas the C1–C2 FJ cavity is best accessed via an anterolateral approach as the posterior aspect of the FJ is heavily overlapped by neurovascular structures, particularly a rich venous plexus. At the thoracic level, small superior and inferior FJ recesses were seen. The needle placement to the inferior recess may be better along the tip of the inferior articular process. At the lumbar level, the posteromedial recesses and anteromedial recesses were equally large, but the posteromedial recess may provide an optimal approach to the FJ cavity. The needle placement is better just above the inferior and lateral edge of the inferior articular process because the extent of the superior and inferior recesses was limited. Care should be taken with the synovial fold as it may impede the spread of injectates.
Retrodural space and the FJ recesses
The direct communication between the FJ cavity and the retrodural space has been reported before.16 18 19 In some literature, in fact, the FJ recesses were referred to as the extracapsular fatty space.16 For example, McCormick et al defined that the FJ superior recess was within the joint cavity, whereas the inferior recess was an extracapsular fat-filled recess which extended into the FJ cavity, forming the synovium-lined ‘intracapsular’ fat pad. The authors named the fat-filled connection between the extracapsule inferior recess and ‘intracapsular’ fat pad as a normal opening through which the FJ inferior recess communicated with an ‘intracapsular’, fat-filled synovial fold.16 Taking the advantage of the newly developed anatomic technology, epoxy sheet plastination, which not only preserves in situ positions of the hard (eg, bones and cartilages) and soft (eg, adipose tissue, vessels and nerves) tissues without decalcification but also allows these structures to be examined at both the macroscopic (gross anatomical) and microscopic levels, this study revealed different configurations of the FJ access (a real space) and the retrodural space (an adipose potential space) in a plastinated section (see the inset of figure 1B). The results of this study showed that at both cervical and lumbar levels, the anterior FJ recess was bordered by a thin layer of the articular capsule and neighboured by a rich adipose area which was part of or extended to the retrodural space. Thus, the clinical evidence of communication between the FJ cavity and the retrodural space in contrast injections into the FJ cavity may be a result of an injection into the ‘intracapsular’ fat pad,16 or leakage from microtears, disruptions or defects of the capsule wall of the FJ recess.9 18 21–23 The factors that are disruptive to FJ capsules, leading to a leakage into surrounding adipose tissues through FJ recesses or isthmic defects, may include articular defects, damaging the tissues of the spinal motion segment such as the vertebral discs,23 24 and the associated FJs that undergo degeneration and effusion.25 26
Limitations
We note at least two limitations. First, a small number of the specimens were examined. Interindividual anatomical variations often exist. Second, the specimens were collected from elderly cadavers. Configuration of the FJ spaces and recesses may be altered due to degeneration of vertebrae and articular cartilages during ageing. Thus, further quantitative studies in the subjects with various ages may be warranted.
Conclusions
We confirm there is no direct communication between the FJ cavity and the retrodural space. The clinical implications of this study may be twofold. (1) The locations, sizes and orientations of the FJ recesses are essential for a better understanding of FJ mobility at different levels of the spine and for targeting the FJ recesses to maximise access to the FJ cavity. (2) Awareness of the relationship between the FJ recess and retrodural space is important during diagnostic imaging interpretation and interventional spine injection procedures.
Acknowledgements
The authors thank Marlene Black (plastination technician) and Andrew McNaughton (micro-CT technician) from the Department of Anatomy, University of Otago, for their technical support.
References
Footnotes
Contributors CGTL and ZX: acquisition, analysis and interpretation of data, and drafting the manuscript. MZ: conception and design of the study, drafting and finalising the manuscript.
Provenance and peer review Not commissioned; internally peer reviewed.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.