Article Text

Abstract
Objective This study explored the perceived effect of the menstrual cycle (MC) on the performance of Australian female athletes, preparing for the Tokyo Olympic and/or Paralympic Games.
Methods 195 female athletes, nominated by 24 National Sporting Organisations as preparing for the Tokyo Olympic and/or Paralympic Games, completed an online questionnaire (‘MCq perceptions’). The MCq perceptions investigated menstrual symptoms, hormonal contraceptive (HC) use and a preferred competition window within the MC.
Results Two-thirds (65.6%) athletes reported that their MC affected their performance; in training (65.6%) compared with competition (58.0%).
Aesthetic-sport athletes were most likely to perceive their performance to be affected by their MC (RR=1.40) compared with endurance (RR=0.88) and strength-sport (RR=1.04) athletes. Athletes experiencing three or more symptoms were twice as likely to identify as affected. Athletes who reported pain (RR=1.89) or the use of analgesia (RR=1.45) were more likely to identify as affected by their MC.
A preferred competition window was identified by athletes as ‘just after your period’ (41.5%). For athletes not using HC, this window was identified by 53.7%.
Conclusion In Australia, elite-female athletes perceive their MC to affect their performance, and many have a preferred performance window. Performance-focused strategies should be created for ‘affected’ athletes, aiming to provide these athletes with education, and where appropriate, control over predictability, timing and symptoms of their MC.
- female
- athlete
- performance
- endocrine
- olympics
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available on request (dralicemcnamara@gmail.com).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Menstrual symptoms in the general and athletic population are common.
It is not yet clear if exercise performance in elite-female athletes is affected by menstrual cycle phase, except it maybe trivially reduced during the early follicular phase.
What this study adds
Two-thirds of elite-female athletes, preparing for Olympic and Paralympic Games perceive their menstrual cycle affects their performance.
Most elite-female athletes can identify a menstrual cycle phase for perceived optimal performance.
How this study might affect research, practice and/or policy?
Further quality research is needed into clear physiological or psychological mechanisms.
The impact of menstrual cycle and performance is an important conversation between athletes and support teams (coaching, medical, performance psychology).
Screening for menstrual-linked pain should be undertaken, as well as accurate diagnoses and treatment.
Introduction
Athletic performance is influenced by numerous factors, including the art of timing physiological and psychological readiness.1 The menstrual cycle (MC) is one sign of normal endocrinological and gynaecological function, and its ability to produce physiological2 3 and psychological4 5 symptoms in women of reproductive age is well described. Despite this, it is unknown how the MC and associated fluctuations in female sex-steroids (oestrogen and progesterone) affect athletic performance. A review of 51 published studies investigating effects of MC on performance concluded that, ‘exercise performance might be trivially reduced during the early follicular phase of the MC’.6
‘Trivial’ is non-congruent with the perception of women logging data on the exercise-tracking network (Strava), where 80% report at least one menstrual symptom ‘often’, associated with training/competition disruption and/or changing/ missing daily activities (eg, work/education).7 Over half of all Australian mixed-level athletes (athletics, rowing, soccer, water-polo n=1248;) and highly trained UK athletes (runners and rowers n=909;) reported that symptoms contributed to perceived reductions in performance in training and/or competition. Detailed interviews with 15 female national-representative rugby athletes revealed that almost all perceived symptoms impact negatively on performance.10 These findings suggest perceived effect of MC on performance despite the absence of a strong mechanistic physiological and/or psychological explanation.
Athletes training for Olympic/Paralympic Games have inflexible competition schedules and high pressure to perform. To date, examination of perceived effects of MC on athletic performance has been conducted in mixed-level athlete groups, or small groups of highly trained athletes in specific sports. If elite-female athletes perceive their MC to affect performance, then further research into physiological or psychological mechanisms relating symptoms or specific phases of MC to performance is warranted.
This study sought to understand factors influencing an elite-athlete to self-report being affected by their MC. We posed two main questions: (1) Does your menstrual cycle affect your performance and (2) When in your MC would you like to race/compete in your Olympic/Paralympic final? We explored several factors that may impact athlete responses including: chronological age, experience, sport-specific characteristics, severity of MC symptoms, MC modification and control, useful conversations and education.
Methods
Study overview and ethics
Athletes aged 16 and over, selected or preparing for selection, for the Tokyo Olympic and Paralympic Games were invited by their National Sporting Organisation (Sports) to complete a questionnaire (MCq perceptions) interrogating their perceptions regarding MC and performance. The MCq perceptions were distributed via hyperlink, participants provided informed consent prior to commencing the questionnaire and data were collected between June and October 2020.
Chief Medical Officers of the Australian Institute of Sport, the Australian Olympic Committee and Paralympics Australia endorsed the conduct of this study. Individual athletes were not identifiable at any stage of the research.
Questionnaire survey and distribution
The MCq perception is an online quasi-structured questionnaire hosted by a cloud-based data storage platform (SurveyMonkey, Australia) consisting of three main sections: (1) Baseline demographics; (2) MC and performance experience, divided into two streams: athletes (A) naturally cycling (AthletesNC) and (B) using hormonal contraceptive (HC) (AthletesHC), asked different questions and (3) relevant performance supports.
Demographics collected included age, sport and event(s), targeted international competition, years of experience on senior national teams and participation in international major events (eg, Olympic Games, Paralympic Games and World Championships). The MC was explored in depth, including the athlete experience of symptoms, analgesia and HC use (and non-use). Athletes reporting amenorrhoea were included in the analyses. Perceived performance and training impacts of the MC were investigated, as was the preferred phase of the MC for their Olympic-/-Paralympic final. The third section used multiple choice questions to identify athlete resources within their performance support teams as well as free-text answers to questions focused on helpful or unhelpful conversations and learnt management strategies.
At the end of the collection period, both study mean and sport-specific mean data were distributed back to the Sports. Sports with less than five respondents received study-mean data only to preserve anonymity.
Data analysis
Descriptive statistics are presented as frequencies (proportion) for AthletesNC and AthletesHC, and where entire cohort data was important, the two groups were combined. A key binary variable was created; a yes/no answer to the research question, ‘Does your menstrual cycle affect your performance?’. Here, athletes affected by their MC were treated as one group compared with the non-affected athletes, and analysed across the domains of; experience, sport-specific and environmental characteristics, symptoms and hormonal modification. ORs with 95% CI were calculated for factors in relation to an athlete identifying as affected. Other data are displayed in table or graphical format. Representative comments are presented verbatim in quotation marks.
Patient and public involvement
Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Results
Demographics
Responses were received from 195 athletes (table 1) across 24 sports; 144 preparing for the 2020 Olympic and 52 preparing for the 2020 Paralympic Games, which due to the COVID-19 pandemic had been rescheduled for July and August 2021, respectively. One athlete was excluded due to incomplete survey completion; and incidentally, they were the sole reporter of primary amenorrhoea. One athlete was preparing for both Olympic and Paralympic Games and was included in both group analyses. Three-quarters of athletes were between 18 and 29 years and 94% had been a senior National team member for at least 1 year. The average training duration was 20.1 hours/week, and 44% had a female coach in their sport-specific coaching team.
Demographic data
MC characteristics and symptoms
Table 2 presents the characteristics of the athletes’ MC characteristics separately for AthletesNC (82; 42%) and AthletesHC (113;58%). Sixty-six per cent of AthletesNC and 60% of AthletesHC having an MC length of 25–35 days while 66% of AthletesNC and 51% of AthletesHC had a period duration of 4–7 days. Half of all athletes described their flow as ‘moderate’, 26% as ‘light’ and 11% as ‘heavy’.
Menstrual Cycle characteristics
Of the 17 menstrual symptoms interrogated, 81% of AthletesNC and 74% of AthletesHC experienced more than three menstrual symptoms, and a further 12% of AthletesNC and 20% of AthletesHC experienced 1–3 menstrual symptoms. Almost half (46%) of all athletes reported using analgesia in relation to their MC.
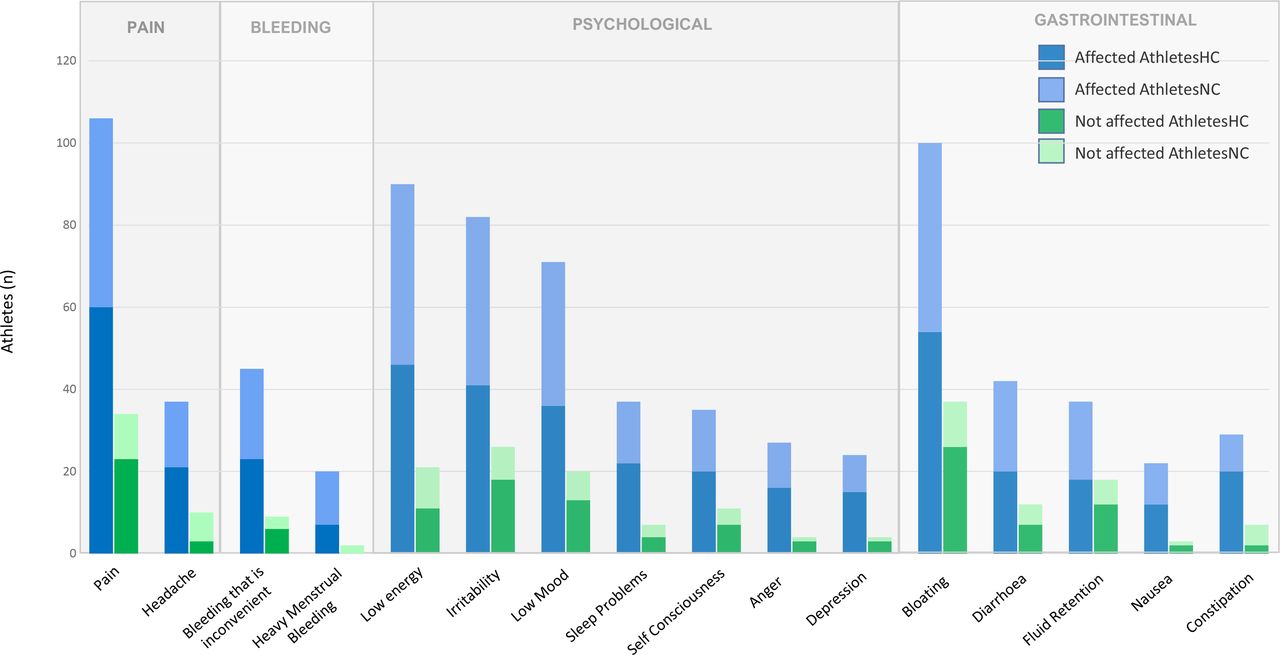
Reported MC symptoms are displayed in figure 1. The most common in the affected athlete group were pain (83%), bloating (78%) and low energy (70%). Athletes reporting three or more symptoms were twice as likely to be affected (RR=2.06). Athletes who identify as not affected by their MC commonly still report symptoms, most commonly bloating (55%), pain (51%) and irritability (39%). Athletes who report pain (RR=1.89) or the use of analgesia (RR=1.45) were more likely to be affected by their MC.

Menstrual symptoms as reported by affected and not affected athletes. HC, hormonal contraceptive; NC, naturally cycling.
HC use
HC use was reported by 113 (58% of the cohort) with 36% using combined contraceptive pill. 20% were using the progestin-releasing intrauterine contraceptive (Mirena); many reporting a favourable experience, for example, ‘Being on the Mirena gave relief physically and mentally’. HC use by type is described in table 3.
Hormonal contraceptive use
The most common reasons for using HC were for contraception (71%), timing and/or predictability of period (61%), symptom control (pain and/or heavy menstrual bleeding; 32%), and ‘performance reasons’ (23%). Multiple athletes articulated how, why and when they used HC to manipulate their MC; ‘I used oral contraception prior to a big event that involved travel’, or (to negate) ‘call room wait times/timing of tampon changes/uniform comp briefs, general discomfort with periods’
Of the 82 AthletesNC, 49 (60%) reported previously using HC. Of those with prior use, the most common reason(s) for ceasing were ‘because they didn’t need it’ (71%), or because of ‘side effects’ (59%).
The effect of MC on performance
Two-thirds of athletes reported that their MC affected their performance. More athletes identified as affected in training (66%) when compared with racing/competition (58%). Individual, systemic and sport-specific factors influence the experience of the athlete, and these are grouped into domains in table 4.
Comparison of ‘affected’ versus ‘not affected’ athletes: factor analysis
Considering athlete experience, chronological age and years of representation on the national team alone played no significant role. However, lived experience may provide the confidence to perform around the MC, as one athlete articulated: ‘At the Rio Olympics I raced with my period and because I knew I’d done 1000 good sessions with it before, it didn’t bother me one bit’.
Aesthetic-sport athletes were most likely to report their MC affected their performance (RR=1.4), with athlete comment along the theme, for example, ‘I hate training with my period because I feel bloated and self-conscious wearing swimwear’.
Technical sport athletes were also likely to identify their MC affected their performance (RR=1.25), for example, ‘In sailing it’s uncomfortable and annoying when you’re on the water for up to 6 hours’.
An optimal performance window
Athletes were asked, ‘If you could choose any time in your cycle to race/compete in your targeted Olympic final/Paralympic final, when would it be?’ (figure 2). The most desirable time to compete was ‘just after their period’ (42%). Just eight athletes (4%) wished to compete ‘late-cycle’ and 1% ‘during their period’. Twenty-three per cent of all athletes responded as ‘unsure’ when they would prefer. AthletesNC were more likely to wish to compete ‘just after their period’ (54%). AthletesHC showed a more even-split of preference across the cycle, although a large proportion (30%) were ‘unsure’.

{kind=link}
{kind=link}
Athlete responses to the question ‘If you could choose any day in your menstrual cycle to race/compete in your Olympic/Paralympic final, when would it be?’ N/A, not applicable.
In aesthetic sports, 67% preferred to compete ‘just after their period’, and none wished to compete ‘late-cycle’. Previous Olympians and those with more than 4 years of experience on the senior national team were most likely to prefer to compete ‘just after their period’ (56%, 47%, respectively).
Sixty-one per cent of AthletesHC use HC to manipulate their MC for optimal timing, although athlete comment demonstrated resistance to depend on this, for example, ‘I have heard about people tailoring training because they can ‘push harder’ at certain points in their cycle. To be honest I disagree with this…you don’t want doubt in your mind…because of the stage of your cycle’.
Two-thirds of athletes wanted there to be ‘more focus’ in sport on the MC and female performance. Athletes called for education, and individual support for self-management, to optimise performance.
Discussion
The effect of MC on performance
This study found two-thirds of elite-female athletes perceive their MC to affect their performance. This is despite the current published findings that MC phase and hormonal change have a ‘trivial’ effect on performance.6 It is plausible that a ‘trivial’ effect of MC on performance may make a critical, although small difference to performance and one noticed by athletes; resulting in effects on performance we have not yet measured. A major strength of this study is the high number of elite-female athletes; 94% senior National team representatives with 55% training for their second or more Olympic/Paralympic Games. Years of specialised training and competing provide rich experience about readiness to perform; physiologically and psychologically.
Athletes in this study were more likely to be affected by their MC in training than competition. This finding is analogous to international rugby players, who reported they were more likely to notice symptoms in the gym, than in competition.10 British11 and Danish12 elite-female athletes rarely refrain from training at certain points of their MC (4%,13%).In contrast, Armour et al8 reported 59% of university and national-level athletes were affected in competition and only 50% in training.8 Elite-level athletes, despite MC symptoms experience pressure to perform in competition. Greater attentional focus during competition may indeed override the distraction of symptoms, or training in a familiar/home environment may allow athletes to tune-in to symptoms.10
Only one athlete identified primary amenorrhoea and failed to complete the survey; her response was excluded. Others, yet to have a period may have self-selected not to begin. Athletes articulated amenorrhoea as a sign of Relative Energy Deficiency in Sport (RED-S) and identified a risk of bone stress injuries in their comments. Some athletes noted strategic cessation of HC to allow MC tracking. Early recognition of MC disturbances may reduce the risk of associated injury and frequent illness with RED-S.13 14
Factors influencing perception of MC on performance
Considering factors influencing perception of MC on performance, there was no significant difference between more experienced and less experienced athletes. Athlete comment, however, reflected confidence from positive experiences competing across their MC, (ie, competing at selection trials and/or Olympic Games) or that of their teammates/mentors. Australian athletes have been previously shown to have poor knowledge in relation to the MC and HC.15 It is likely that knowledge gained through experience provides the confidence to perform.
Aesthetic-sport athletes in this study (competing in leotards and swimwear) were most likely to report their MC affected their performance, noting bloating and inconvenient bleeding. Across the larger group, athletes identified using HC to avoid inconvenient bleeding, that is, during the extended time on the water in sailing, or athletics call-rooms. This is consistent with the study by Armour et al8 where half of the athletes were concerned about ‘bleeding through’' in competition. In this study, almost two-thirds report using HC to manipulate the timing of their period, more commonly than the 53% of athletes at national or university level8 and one-third of team-sport athletes in the study by Clarke et al16
One-fifth of all respondents were using an intrauterine progestin-releasing HC (Mirena), which has the intended effect of locally induced oligomenorrhoea, preserving circulating estrogens. Table 2 shows a lower number of periods experienced in HC users, which may be in part due to the high rate of use of the Mirena. Use of this form of HC is higher than in previous research, so it would be interesting to understand prescribing preferences and patterns in Australian Sport and Exercise Physicians, Gynaecologists and General Practitioners working with elite athletes in future research.
Coach gender was not a significant factor influencing whether an athlete perceived their MC to affect performance, yet athletes called for education specifically for their male coaches. In a recent study, one-quarter of athletes thought their male coaches would not understand because of their gender.8 The results of this study suggest that male coaches and staff can have a similar ability to support female athletes, and should be supported with education to do so.
An optimal performance window
Three-quarters of elite-female athletes could identify an individual optimal performance window. More than half of AthletesNC reported an optimal performance window of ‘just after your period’, or the mid-follicular phase. It has been suggested that progesterone may have a negative impact on competitiveness, with females more likely to select into a competitive environment during the follicular phase.17 ‘Just after your period’ eliminates the inconvenience of bleeding in competition; logistics of changing sanitary items and risk of leakage. Aesthetic-sport athletes (67%) showed an even-stronger preference for this window.
AthletesHC described using HC to manipulate the timing of their cycle to compete away from the late luteal phase and early-follicular phase, minimising their perceived effect on performance. Strength-sport athletes showed a more even-distribution between ‘just after their period’ and ‘mid cycle’. Whether this has relevance to the oestrogen spike just before ovulation cannot be determined, but warrants further investigation. AthletesHC are exposed to medication-specific exogenous hormones, so as expected there was a more even-distribution of preference across the cycle.
Menstrual symptoms and management of pain
MC symptoms in elite-female athletes are common (77%–93%).10–12 In this study, athletes reporting three or more symptoms were twice as likely to identify as affected. Athletes who self-identified as not affected by their MC commonly still report some symptoms. It could be suggested there is environmental pressure to under-report impacts of MC, particularly in the high performance context when there is a focus on appearing fit for selection.
Experiencing pain increased the likelihood of an athlete identifying as affected. Screening for pain and referring to medical practitioners is important, to diagnose and manage underlying causes (eg, endometriosis, gastrointestinal or musculoskeletal pathology). Medical advice on safe and effective analgesia use around training and competition is essential and should be part of a strategy to minimise the effect of symptoms on performance.
Considerations for para-athletes
This study surveyed 52 para-athletes, and 40 (77%) reported their performance to be impacted by their MC, higher than the group mean. Valuable athlete comments introduced specific symptoms not asked; such as ‘nerve pain’ and ‘exacerbation of multiple sclerosis symptoms’.
The para-athlete population are diverse in both their impairments and sport-specific requirements and are not well studied in this area. In 1 study of 110 elite-female US para-athletes training for the 2016 and 2018 Paralympic Games, 44% of premenopausal females had oligomenorrhoea/amenorrhoea.18 The IOC update on RED-S14 highlighted considering potential alteration to the hypothalamic–pituitary axis in the setting of central neurological injury regardless of energy status, when examining menstrual dysfunction in para-athletes. Difficult cases should involve an interdisciplinary team. The para-athlete population requires regular screening of menstrual symptoms and low energy availability. Practically, it is important to especially consider athletes with a functional impairment or who require personal care assistance, and how that may impact timely changing of hygiene products. Performance-focused, and individualised solutions should be sought, involving the athlete.
Limitations and suggestions
The MCq perception were an opt-in survey, with likely limitations of the sample, including self-selection bias suffering impact of MC on performance, had minimal support and/or those who have had prior education on MC. One in five athletes noticed a change in their MC, in this period of training curtailed by the COVID-19 pandemic.19 Answer bias may have occurred due to normal or circumstantial MC phase experienced at time of survey completion. Unaffected athletes may not have prioritised participation.
This study adds the athlete perception data, that there are individual preferences for a performance window across the MC. Exploring psychological changes (ie, competitiveness) across the MC may provide further clarity, or explore the relationship between severe symptoms and a reduced desire to compete.
Another limitation is that severity of symptoms were not objectively captured; however, athletes used free text to describe how particular symptoms were debilitating, impairing their ability to perform. Pain was the most impactful symptom and analgesia use was high. Further research is suggested into non-pharmaceutical management (ie, nutrition) and specific analgesia strategies in the athletic female population.
Conclusions
Two-thirds of elite-female athletes, preparing for Olympic and Paralympic Games report their MC affects their performance. Athletes are more likely to be affected in training than competing. When asked to choose an optimal performance window for performance, the highest proportion of elite Australian athletes preparing for the Olympic/Paralympic Games wish to compete ‘just after their period’.
Aesthetic-sport athletes, those with three or more symptoms or specifically ‘pain’ are more likely to identify as affected. Screening for menstrual-linked pain should be undertaken, diagnosis and treatment. Para-athletes are more likely to be affected, and further research and individualised practical strategies for para-athletes are needed. This study also highlights the lack of female coaches, and hence the need to ensure both better education of male coaches and more development of female coaches.
Supplemental material
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available on request (dralicemcnamara@gmail.com).
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from Griffith University Human Ethics Committee (GU 2020/309).
Acknowledgments
Ali Campbell for her vision and leadership, initiating the AIS Female Performance and Health Initiative. NSO support staff for championing this research and distributing the survey hyperlink to athletes. Dr David Hughes CMO of AIS, and Dr Peter Fricker CMO of AOC, Justin Crow Senior Manager High Performance Paralympics Australia for supporting research in this area.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @alice_mac6
Contributors This study was designed by AM/RH/CM, Communication to Sports was via RH, data were collected and analysed by AM; data interpretation and manuscript preparation were undertaken by AM/RH/CM. All authors approved the final version of the paper. AM acts as guarantor.
Competing interests RH as CMO of Paralympics Australia, sought approval from PA to collect data in parasport. AM as Pathways Medical Lead of Rowing Australia sought approval from PMO of Rowing Australia and Head Coach of Women’s Rowing NTC to collect data in rowing.
Patient and public involvement statement In 2019 the Australian Institute of Sport conducted its first Female Performance and Health Initiative focus group gathering together current high performance coaches, sports scientists and sports medicine practitioners, academics, and past athletes to discuss the priorities for the Female Performance and Health Initiative. The meeting outcomes shaped the aims and objectives of the MCq-perceptions, and the question design. At the end of the collection period, both group mean and sport-specific mean data was distributed back to the Sports. Those sports who had less than five respondents received group-mean data to preserve anonymity for their athletes. Some sports have used their data in education sessions. The broader preliminary data was used to help inform priorities of the Female Performance and Health Initiative in 2021-22.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.