Article Text

Abstract
Objective Pseudoephedrine is a stimulant that can be purchased over-the-counter to relieve symptoms of nasal and sinus congestion. Owing to its similar composition to ephedrine and other amphetamines, pseudoephedrine mirrors some of its ergogenic effects. This study investigates its possible ergogenic effect through a systematic review. Our primary aim was to determine the effects of pseudoephedrine in sport and its potential for performance enhancement.
Design We searched EMBASE, MEDLINE, PsychINFO and The Cochrane Library for trials conducted from their beginning to March 2015. Any published trial that used randomised assignment to the intervention and control groups in full text and measured pseudoephedrine as an independent variable were included.
Results Overall, the review showed that the ergogenic effect of pseudoephedrine is dose-dependent. None of the reviewed studies showed an ergogenic effect at the therapeutic dose of the drug (60–120 mg); however, supratherapeutic doses (≥180 mg) yielded clinically significant results.
Conclusions Owing to the limitations of the published studies in this field, we were unable to make any firm conclusions with respect to the overall effect of pseudoephedrine and its ergogenic effect. It is evident that there is a correlation between the dose administered and its ergogenic effects, but it is also evident that the side effects of using above the therapeutic dose outweigh the possible benefits of using pseudoephedrine in sport. Further research with larger sample sizes is required to determine the relationship between doses (≥180 mg) and concentrations in urine that cause an ergogenic effect.
- Doping
- Drug use
- Power output
- Ethics
- Evidence based review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
During the 1995 Pan American Games, Silken Laumann sailed to victory with her teammates in the women's quadruple event.1 Five days later, Laumann's drug screen showed levels of the prohibited stimulant pseudoephedrine (PSE), and the gold medal was revoked. It was later determined that Laumann had inadvertently taken over-the-counter PSE-containing medication for symptomatic relief of her cold.1 Jack Uetrecht, a professor of pharmacy and medicine at the University of Toronto claimed that the dose and form Laumann took ‘did not enhance performance’, the officials of the games did not agree.1 The banning of PSE has since become a highly debated topic in both the athletic and medical field.
PSE is a sympathomimetic amine that is readily available over-the-counter as a nasal and sinus decongestant.2 Specifically, PSE activates adrenergic receptors in presynaptic neurons, which causes vasoconstriction. This decreases inflammation and mucous production2 which relieves symptoms of the common cold. PSE has also been proposed to have ergogenic effects, likely due to its similarity to ephedrine and other central nervous system stimulants. These effects include increased muscle contractility, increased blood flow to skeletal muscles, increased glycogenesis, increased central nervous activation and heart rate, as well as decreased time to fatigue.3 The International Olympic Committee and other organisations have banned the use of any substance that may enhance the sympathetic nervous system and, by its nature, have concluded that PSE has the potential to have this effect. Owing to the ergogenic nature of this drug, it is believed that it is a violation of the spirit of sport. Therefore, PSE was banned from use in competition.
It has been debated whether or not PSE is actually capable of generating any ergogenic effect. This continued debate has resulted in multiple changes to its position on the prohibited and/or monitoring list. Until 2004, PSE was included on the International Olympic Committee prohibited list. From 2004 to 2010, PSE was removed from the prohibited list, and later added to the monitoring list for in competition in 2010.4 In this position, the use of PSE was considered doping if the urine concentration was greater than 150 μg while in competition.4 Recently, as of 1 January 2015, PSE has been removed from the monitoring list.4
Despite potential risks and uncertainty on the ergogenic effects of PSE, athletes have still been known to abuse PSE for its potential enhancement ability. Data collected by the World Anti Doping Association between 1996 and 2003 yielded 33 adverse analytical findings for PSE out of 52 347 in-competition analyses, or 4.1 positive controls per year.4 ,5 In 2007 and 2008, that is, 3 years after PSE was removed from the prohibited list, the prevalence of PSE and ephedrine was determined in 16 335 in competition doping control samples.4 ,5 The analyses resulted in 102 cases of PSE use or misuse.4 ,5
The purpose of this systematic review is to qualitatively consolidate the results of studies relating to the ergogenic effect of PSE in order to determine the validity of its ban from competition. Previous studies have yet to resolve the existing conflicting results, even when standardised testing methods are utilised.6–8 Therefore, this article aims to clarify the relationship between PSE and sport enhancement on various parameters, specifically relating to drug dosage.
Objectives
To determine the effects of PSE in sport and its potential for performance enhancement.
Criteria for considering studies for this review
Types of studies
Any published randomised control trial (RCT) in the English language, including cross-over studies. Owing to the controversy in this area, the authors felt that randomised controlled studies were the most appropriate research design to minimise bias to address the effectiveness of intervention. Studies were excluded if PSE was not the sole substance being administered to an athlete at a given time, or if the substance was not specifically being investigated for its ergogenic effects. This limitation was to ensure the data presented were not affected by any confounding variables.
Types of participants
Participants were male and female athletes of any level between age 18 and 65, with no other comorbid conditions.
Types of interventions
Studies must have used PSE as the only substance in the intervention. Studies that looked at other substances were included if athletes were not administered both substances simultaneously. The presence of a control and/or placebo group was also necessary for inclusion.
Types of outcome measures
Outcomes measured included any enhancement in sport above baseline such as timing, strength, time to fatigue and/or respiratory enhancement.
Methods
Search strategy
We searched EMBASE, MEDLINE, PsycInfo and Cochrane Library databases for trials from their beginning to March 2015 (figure 1).

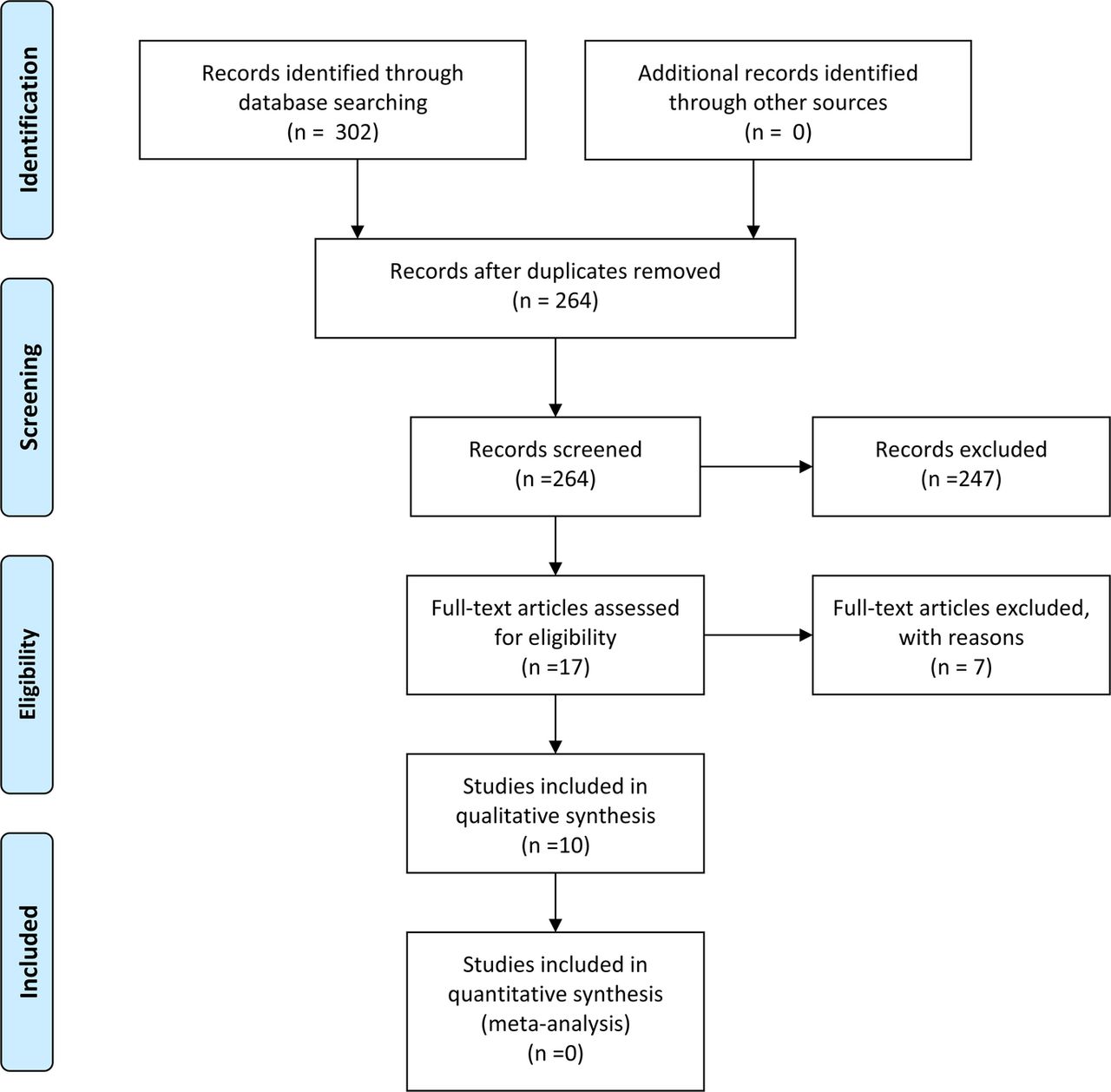{kind=link}
PRISMA 2009 flow diagram.
Study selection
At least two authors independently conducted citation identification, study selection and data abstraction. Disagreements were resolved through a third assessor.
Methodological assessment
At least two authors independently assessed each RCT for methodological quality and bias, based on the Cochrane's GRADE scale and the Cochrane's collaboration tool for assessing risk of bias.9 ,10 Disagreements were resolved through a third assessor.
Data extraction
Two authors independently extracted raw data for demographics, descriptions of interventions and all outcomes to predesigned forms.
Data analysis
Data were retrieved and filed into abstraction forms. Differences between assessors were resolved by repeated review and consensus. The risk of bias of the RCT was assessed through the use the Cochrane collaboration's tool for assessing risk of bias. A third assessor resolved differences between assessors.
Description of studies/study selection
In consultation with two research librarians, we developed search strategies to identify potentially relevant studies from the EMBASE, MEDLINE, PsycInfo and Cochrane Library databases (see online supplementary appendix 1). We sought reports of RCTs, including cross-over trials, in relation to PSE use for its ergogenic effect. Clinical judgement was used to review the search and retrieve potentially relevant studies. Studies were excluded if they had co-interventions with other drugs (table 1).
Excluded studies
Methodological quality
Methodological quality was graded using two sets of criteria:
Risk of bias: based on selection, performance, detection, attrition, reporting and other biases.10
Cochrane GRADE table: began with highest quality rating for randomised trial evidence with downgrades to moderate, low or very low depending on the presence of limitations in design, indirectness of evidence, inconsistency of results, imprecision of results and high probability of publication bias.9
Results
Out of 301 articles retrieved from EMBASE, MEDLINE, PsycInfo and The Cochrane Library, 39 duplicates were removed. From the 262 remaining, 17 studied the ergogenic effects of PSE and PSE-like substances. Of these 17, only 10 were devoted solely to studying the ergogenic effects of PSE and were used for this systematic review. Therefore, 10 remaining studies met all inclusion criteria (table 2).
Characteristics of included studies
Continued
Placebo versus PSE
Of the 10 chosen studies, 3 showed significant improvement in athletic performance.20 ,24 ,25 These three studies used a supratherapeutic dose of at least 180 mg or 2.5 mg/kg of PSE, whereas the other studies used a therapeutic dose (60–120 mg or 1–2 mg/kg). The studies that used lower dosage of PSE showed no significant improvement for all measured parameters.18 ,19 ,21–24 ,26 ,27 The authors compared both 60–120 mg or 1–2 mg/kg and ≥180 mg or 2.5 mg/kg of PSE to a placebo of similar appearance on the effects on maximal torque and peak power, decreased time to complete trial, and respiratory function. While the placebo and 60–120 mg or 1–2 mg/kg PSE categories showed no significant change, the ≥180 mg or 2.5 mg/kg PSE group showed significant improvement for all measured parameters. However, due to heterogeneity of the measurements selected in the trials, quantitative synthesis of data was not possible.
Discussion
Our objective was to determine the effects of PSE on athletic performance in athletic individuals in good general health. Qualitative analysis showed overall positive results in favour of PSE over placebo for PSE doses ≥180 mg or 2.5 mg/kg. Doses below 180 mg or 2.5 mg/kg and placebos showed insignificant changes in athletic performance.
Interventions varied with respect of duration of treatment, doses of PSE, diet and type of exercise trial. For instance, though Pritchard-Peschek et al25 and Hodges et al24 showed significant improvements in timed trials using PSE doses ≥180 mg or 2.5 mg/kg, the studies could not be meta-analysed as their interventions were different (1500 run25 and 7 kJ/kg body mass work24 time to completion, respectively). Owing to such heterogeneity, using the qualitative method of synthesising the evidence was more appropriate. However, this method is sensitive to how studies are categorised, as meeting the criterion of a certain level of evidence depends on the number of studies present in a category, methodology and risk of bias.
All studies were assessed to have a low risk of bias (table 3). For their quality of evidence, the studies were downgraded from high level of evidence to moderate, low or very low depending on the presence of limitations in design, indirectness of evidence, inconsistency of results, imprecision of results and probability of publication bias with the Cochrane GRADE scale (table 4). All studies were RCT in design and implementation and had a low likelihood of bias; thus, none of the studies showed limitations in design. The results of all parameters were also consistent based on dose; only PSE doses ≥180 mg or 2.5 mg/kg showed significant results, while placebo and doses below 180 mg or 2.5 mg/kg did not. However, only two studies measured the parameters of Wingate test, peak power of maximal cycling and isometric muscle test, leading to small sample sizes. We believe that high quality of evidence should be reserved for conclusions in which the likelihood of making an incorrect reference is small, that is, having consistent findings in multiple sampled studies with low risk of bias. Thus, these categories were downgraded from high-to-moderate quality due to their risk of imprecision. Publication bias of the studies was unclear to assess as only published trials were available through literature search. Additionally, none of the studies directly compared the effects of variable therapeutic doses of PSE. The question of whether higher doses of PSE impact athletic performance would have been more directly addressed if studies had two explicit interventions—a high and low therapeutic PSE dose group—and a control placebo group. This would allow direct analysis between the variables and strengthen the studies’ quality of evidence. Thus, all evidence was downgraded in quality due to the indirectness.
Risk of bias
Summary of findings
The approach to summarising the literature has several strengths. We used a comprehensive, librarian-assisted search of multiple databases. Healthcare professionals decided on article relevance and assessed quality. At least two people extracted the data and the principal investigator verified data entry.
The effect of PSE on athletic performance is a highly debated subject in both the medical and athletic fields. The findings of this review are useful for the design and planning of a larger clinical trial that assesses the effect of PSE on performance with a focus on a direct comparison of doses. PSE has been on and off the WADA guidelines for some time, and present evidence does not indisputably support the banning of PSE at a lower dose. Thus, a large-scale study should be conducted to formulate an approach to this question.
Authors’ conclusions
Implications for practice
The authors of this review conclude that there is moderate evidence suggesting that higher doses of PSE may be more beneficial than inactive placebo pills or lower doses in enhancing athletic performance. Therefore, these findings should be considered throughout the process of developing substance laws in competition. This would provide a more accurate maximum use of PSE to be considered as doping or whether it has a place on the monitoring list. Since PSE is present in over-the-counter decongestants, changes may allow athletes to take appropriate doses for symptomatic relief while taking the necessary precautions to avoid doping allegations and harmful side effects.
Implications for research
The banning of substances in competition is a highly debated and continually changing field. Therefore, there is need for a large, high-quality RCT to determine the role of dosing of PSE on enhancing athletic performance.
Implications for an updated systematic review
There is no recent systematic review on the effects of PSE on athletic performance. Thus, a current systematic review on this topic is necessary to summarise the current findings on PSE use and doping regulations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors JK and AR ran the literature search, analysed and chose the relevant studies, critiqued their methodology and quality of evidence, and formed relevant conclusions. KVT analysed and chose the relevant studies, critiqued their methodology and quality of evidence, and formed relevant conclusions. All authors proofread the paper.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.