Article Text

Statistics from Altmetric.com
Introduction
Rotator cuff tendinopathies are the most commonly diagnosed musculoskeletal shoulder conditions and are associated with pain, weakness and loss of function.1 Tendon swelling may be associated with tendinopathy and may result from acute overload.2–3 An increase in tendon cells (tenocytes) and upregulation of large molecular weight proteoglycans, such as aggrecan, may increase tendon water content.2 There is uncertainty as to whether the swelling is related to the pain or is instead an observed but unrelated phenomenon. Weakness detected clinically may be due to pain inhibition.4–5
Early treatment of acute rotator cuff tendinopathy involves patient education and relative rest, and may include non-steroidal anti-inflammatory drugs (NSAIDs) to reduce pain, swelling and inflammation. Subacromial corticosteroid injections are also used to achieve the same purpose. These techniques show low to moderate evidence of reducing short-term pain but they do not improve function.6 The medications have side effects such as gastrointestinal tract complaints,7 and corticosteroids may damage tendon tissue.8 Identifying alternative ways to control pain and inflammation may be warranted.
Two clinical procedures to manage RC tendinopathy include ice wraps and isometric exercise, however, there are no empirical data supporting their use. This pilot study, conducted at the Illawarra Sports Medicine Clinic, NSW, Australia, was designed to test (1) the short term analgaesic effect of these interventions and (2) the feasibility of a larger clinical trial for adults diagnosed with acute rotator cuff tendinopathy (<12 weeks).
Method
Thirteen women and seven men, aged 20–67 years (mean age 50 years) with unilateral shoulder pain (<12 weeks duration) and symptoms aggravated with active or resisted movement participated in the study. Inclusion criteria also comprised of an unaccustomed increase in shoulder activity preceding onset of symptoms and evidence of tendinosis or bursitis on ultrasound imaging. Exclusion criteria included dominant biceps pain, frozen shoulder, full thickness or large partial thickness tears and traumatic onset of pain.
Participants were randomised to three intervention groups: (A) ice, (B) isometric external rotation (ER) exercises progressed from 3–5 times per day and from 10–20 s duration contractions, (C) a combination of group (A) and (B) protocols. Interventions were conducted for 1 week. Pain (visual analogue scale (VAS) scores), function (the disabilities of the arm, shoulder and hand (DASH) scores), strength (forward flexion at 90°) and structural integrity (ultrasound) were measured preintervention and postintervention. The sonographer and chief investigator were blind to group allocation. Ethical approval (HE11/183) was granted from the University of Wollongong, New South Wales, Australia.
Statistical analysis
Mean changes, range and SDs were calculated for all outcome measures, and relative change was recorded where applicable. The intervention effect on all outcome variables was assessed via a repeated measures analysis of variance, with paired (time effects) and independent (group effect) t tests used for post hoc analysis. All statistical analyses were conducted using SPSS software (SPSS 21 for Windows, Illinois, USA).
Results and discussion
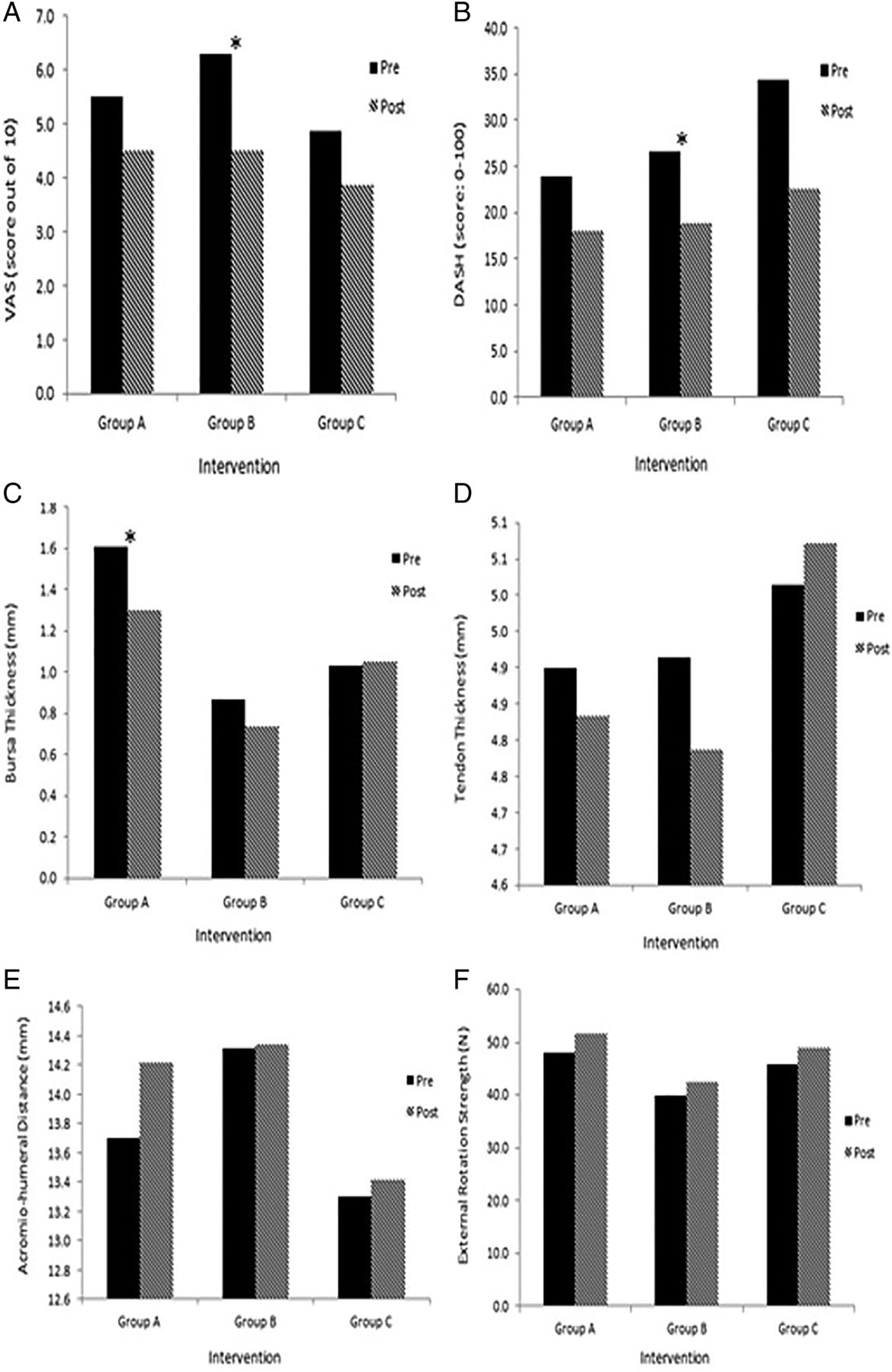
There were significant improvements (p<0.05) in pain and function, isometric elevation strength at 90° and reduction in bursal size following one week of intervention group (A) ice or (B) isometric ER exercise (figure 1). There was no significant difference between the groups and no added benefit demonstrated when both therapies were combined (C).

{kind=link}
Rotator cuff tendinopathy symptoms treated by ice (group A), Isometric exercise (group B) or Combined Treatment (group C; *indicates a significant within-groups difference, p<0.05).
Reduction in bursal thickness (figure 1C) was principally observed in group (A) ice. This reduction may have been due to the effect of reducing sub-acromial volume, which may have influenced subacromial pressure. This suggestion, however, remains speculative.
Within group (B) isometric ER exercise, a small reduction in tendon thickness was observed for 71% of participants following intervention (figure 1D) although this was not statistically significant. Of these participants, 80% also demonstrated improvement in VAS postintervention. We speculate that ice and isometric exercise possibly target different structures or pain mechanisms.
As a pilot study, our results are encouraging, however, due to the small number of participants and lack of control group, these results should be interpreted with caution and a definitive reason for pain relief cannot be extrapolated. Participants indicated that neither the treatment schedule nor the assessment procedures were excessive and they reported no adverse events. Our methodology is feasible for a study with a larger cohort.
Footnotes
Twitter Follow Phillip Parle at @Phillip Parle@Philparle
Competing interests None declared.
Ethics approval The University of Wollongong Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full results from the unpublished full manuscript are available for discussion at philparle@optusnet.com.au