Article Text

Statistics from Altmetric.com
The WHO declared COVID-19 a global pandemic on 11 March 2020.1 On 20 and 23 March 2020, faced with a rising number of both COVID-19 cases and deaths, the UK government imposed a range of measures in an attempt to control the pandemic in the UK. Although individuals were allowed to run and cycle outdoors, these instructions effectively put sport on hold, resulting in widespread training disruption to the elite athlete population.
Collaborating to form ‘one voice’
The chief medical officers of many of the major Olympic, Paralympic and Professional Sports in the UK formed a group to share thinking around how elite sport might best plan for a return at the appropriate time. While it was acknowledged that there were fundamental differences between the sports, including but not limited to current and future competition schedules, financial and personnel resources, potential risks of COVID-19 transmission between participants and their ability to align with any relaxation of population social distancing (SD), a collaborative approach to planning ‘how’ elite sport might restart was agreed to be the most effective manner to inform a single dialogue with government and Public Health England.
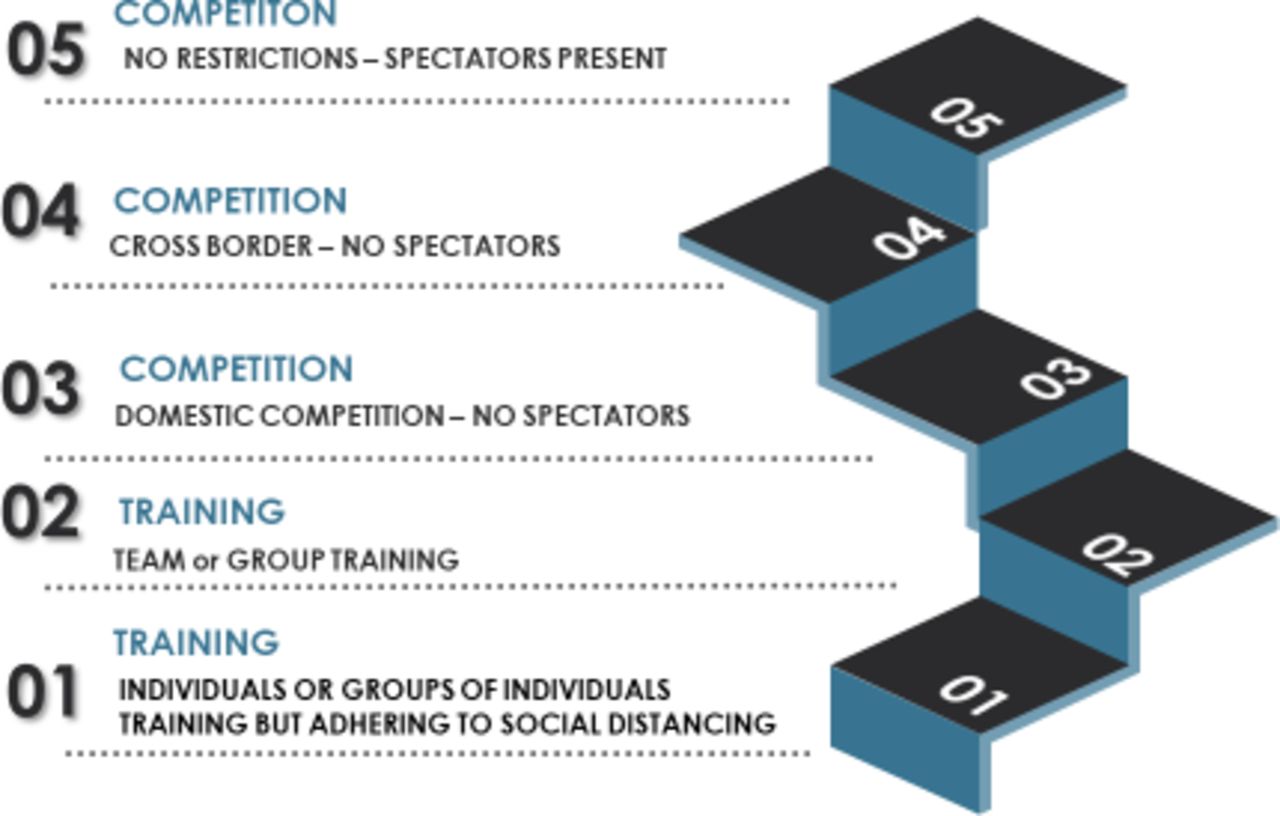
Central to this approach was the development of a five-stage model (figure 1) that set out the discrete stages that sport would need to progress through, to ultimately return to unrestricted competition, starting with stages with a lower risk of COVID-19 transmission. It was hoped that this model would help create a consistent taxonomy when in conversation with government, health agencies, athletes, coaches and sports administrators.
{kind=link}
Five stages for the resumption of elite sport in the UK.
Carmody et al 2 proposed an approach to the risk assessment of sporting events, based on WHO guidance that informs much of the planning within stages 3, 4 and 5. It is also recognised that the stages may need to be descended, or progress paused, depending on the disease epidemiology within wider society and the government and public health response.
Our group’s focus has been how best to plan, question, brief and ultimately influence and co-produce government-approved guidance documents. Protecting the well-being of the athlete, support staff and spectators have remained a priority throughout. The guidance has also needed to accommodate our rapidly evolving understanding of the science while not adversely affecting the whole population R number, nor negatively impacting key healthcare resources, including personal protective equipment.
The guidance provides a framework for each sport in the UK to progress, from the 23 March position f(stage 0) to stage 1 (the organised training of individual elite athletes) in hygiene optimised performance facilities while maintaining SD at all times. Sports can then progress to stage 2 (close contact group and team training) where for a number of the sports involved SD or avoidance of sharing sports specific equipment/items, cannot practically be maintained or avoided at all times, and subsequently to stage 3 (competition behind closed doors where SD often cannot be maintained at all times and opposition are included). Following discussions with UK Sport and the Department of Culture Media and Sport, minimum practice guidance for stage 1 was published on 13 May 2020,3 stage 2 on 25 May 20204 and stage 3 on 30 May 2021.5
The stage-specific guidance highlights the minimum standards that elite sports will need to meet at all times. All existing current government and Public Health England (PHE) guidance remains applicable unless otherwise specified. A summary of the key considerations for each stage are as below in table 1.
A summary of the key considerations for stages 1–3
The guidance for each stage builds on the approach and principles set out in the guidance for the previous stages. In stage 2 where strict SD in some sports cannot be observed during all training activities, the risk of COVID-19 transmission between athletes is consequently increased. The stage 2 guidance highlights the role of enhanced screening protocols for athletes and support staff, together with minimising close and face-to-face contact activities, consistent with effective training in mitigating this risk. The potential for significant disruptions to teams, squads and competition as a result of the isolation requirements both for athletes confirmed with COVID-19 and their close sporting and non-sporting contacts is recognised. Levels of community transmission are anticipated to be an important factor in the decision of sports with a greater risk of close and face to face contact as ‘when’ to return to stage 2 (and subsequently stage 3). The guidance for step 3 (competition without spectators) builds on the approach and principles set out in the step 1 and step 2 guidance with specific considerations for competition where strict SD cannot be observed at all times.
These guidance documents, read in conjunction with existing guidance around the risk assessment and minimum standards for competition,6 7 provide the major elite UK sporting organisations with a quality assured framework to plan ‘how’ they might return. Further consideration is needed to determine ‘when’ a return is appropriate. It is envisaged that for an individual sport, this will be based on a sport specific risk assessment, close consultation with relevant public health authorities and consideration of the time needed to safely recondition its athletes.8
Acknowledgments
We wish to acknowledge Anna Deignan, DCMS: Sally Munday and Michael Bourne, UK Sport, for their assistance in the production of the guidance.
Footnotes
Twitter @drsimonkemp, @drccowie, @peirce@123
Contributors All authors made substantial contributions to the conception and design of the work. SK drafted the work, and all authors revised it critically for important intellectual content and provided final approval of the version published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SK is the medical services director for the Rugby Football Union. CMC is the head of medicine at the Football Association. MG is the medical advisor to the Premier League. RH is the medical advisor to the English Football League and a sports physician at the English Institute of Sport. JH is the chief medical advisor to the British Horseracing Authority. IZ is chairman of the Premier League Doctors Group and head of sports medicine at Crystal Palace Football Club. PJ is the deputy national medical director at the English Institute of Sport. RJ is the director of medical services at the English Institute of Sport. JL is the chief medical officer to the LTA. NP is the medical director to the England and Wales Cricket Board. GP is the team doctor for Hull Kingston Rovers Rugby League Club. JC is a board member of the Fortius Clinic.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.