Article Text

Statistics from Altmetric.com
Why all the fuss about adherence?
Have you ever wondered why some patients do not adhere to drug prescriptions despite warnings regarding the health consequences of non-adherence? The simple reason is that it takes more than just a prescription and education to get patients to take their drugs. A similar scenario has become apparent in the field of sport injury prevention. Over the past two decades, sport injury prevention researchers have developed innovative and proven interventions for injury prevention in athletes. However, most interventions have been developed without the optimal implementation context in mind. Researchers provide evidence of intervention efficacy and as much public advocacy as possible, more like the ’prescribe and educate’ tradition. Unfortunately, the challenge of non-adherence remains palpable.
The WHO defines adherence as ‘the extent to which a person’s behaviour – taking medication, following a diet, and/or executing lifestyle changes – corresponds with agreed recommendations from a healthcare provider’.1 The effectiveness of any treatment or prevention intervention is determined jointly by its efficacy and user adherence to the intervention. While it is common practice for ‘compliance’ and ‘adherence’ to be interchangeably used by researchers, these constructs have different meanings.1 2 Adherence has been identified as the more appropriate concept when capturing dynamic and complex changes required to assess interventions over time.2 In the clinical setting, the idea of compliance is associated with blame and signifies a paternalistic viewpoint between healthcare providers and patients.1 Thus, adherence is a preferred term from both a research and clinical perspective. Currently, very little information is available on adherence in existing sport injury prevention literature, as most studies have been efficacy trials that have focused on compliance. There is a need to advance sport injury prevention research by focusing more on implementation outcomes such as intervention adherence. This editorial highlights the importance of adherence in sport injury prevention research and practice, and provides a framework to raise the bar for sport injury prevention adherence research.
Adherence as a multidimensional implementation outcome
Despite irrefutable evidence of the benefits of sport injury prevention interventions (eg, the 11+, Nordic hamstring programmes3 4), implementation remains a major challenge in real-world settings.4 5 Adherence is an essential modifiable factor for successfully implementing proven interventions. Although adherence is a behaviour observed in athletes and coaches alike, causality extends beyond the athlete and coach. Adherence is a complex behavioural process determined by several interacting factors, which may include athlete, coach and/or intervention provider attributes, in addition to organisational, socioeconomic-related and programme-related factors.1 A multilevel and interdisciplinary approach is thus crucial in addressing low or non-adherence to sport injury prevention interventions.
To minimise the problem of low and non-adherence, researchers have been advised to ensure a fair balance between evidence and ongoing consultations with intended users throughout programme development.6 While this suggestion is fundamental for successful implementation, identifying and modifying determinants of adherence remain a worthwhile research challenge for new and existing interventions.
Four steps to advance adherence research
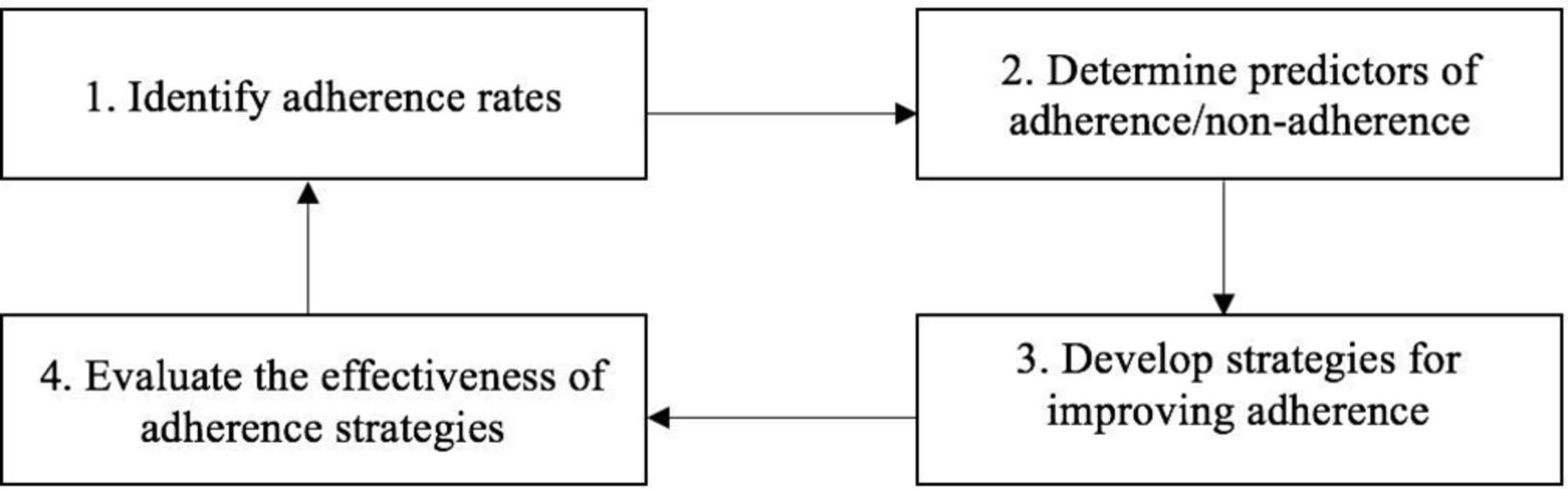
The four key steps towards more rigorous approach to promoting adherence to interventions are shown in figure 1.

{kind=link}
Proposed research framework for the development of effective adherence strategies (adapted from van Mechelen et al’s7‘sequence of prevention’).
Step 1
Sport injury researchers should identify and describe the extent of (non-)adherence (adherence rates) in pragmatic trials and quasi-experimental studies. Researchers should also examine the type and extent of any modifications made to sport injury prevention interventions by users. There is currently no consensus on how adherence should be reported, so we propose that researchers should clearly provide theoretical and operational definitions of adherence, including relevant calculations. For instance, researchers should specify the measures of adherence to an exercise-based intervention using specific terms and definitions (box).
Measures of adherence to exercise-based interventions (example)
Utilisation frequency: sessions completed per week.8
Utilisation fidelity: components completed of total possible per session.8
Duration fidelity: sessions completed in prescribed time of total possible.
Exercise fidelity: proportion of players performing all aspects of exercises correctly.9
Cumulative utilisation: sessions completed of total possible.8
Step 2
Identify predictors of (non-)adherence, considering programme-related factors (eg, intervention components), psychosocial factors (eg, determinants of behaviour change such as intention and self-efficacy), social factors (eg, socioeconomic status) and organisational factors (eg, club structures). These should be assessed across the spectrum, from the individual user (eg, coach, player, healthcare provider) to the broader sports context (eg, administrators). Additionally, barriers and facilitators to programme adherence within the specific context of implementation should be identified.
Step 3
Using the evidence obtained from steps 1 and 2 and current literature, develop and introduce strategies for improving adherence rates to the sport injury prevention programme in the clinical context (eg, a multilevel approach targeting more than one factor and across the dimensions of adherence). This might include strategies to change user behaviour, improving organisational support, providing user incentives, reducing SIP intervention length and removing identified barriers.
Step 4
Evaluate the effectiveness of the adherence strategies introduced in step 3 through pragmatic trials or by repeating step 1. This final step is imperative to guide stakeholders on what works and where to direct resources to promote behaviour change.
These steps may be followed using appropriate research designs such as the following:
mixed methods including focus group interviews and direct observations
pragmatic trials and quasi-experimental studies using open and closed-ended questionnaires to obtain specific information of interest.
It is important that sport injury prevention intervention effectiveness be re-evaluated whenever intervention-related modifications are made (eg, modifications affecting programme components/duration). The measurement and unraveling of adherence is an evolving science, and these four steps provide a framework to improve adherence research and ultimately intervention implementation.
Footnotes
Contributors OBAO conceptualised the idea in the editorial. CDM and EALMV contributed to its development. CDM, EALMV and CAE gave feedback on drafts, and all authors approved the final version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.