Article Text

Abstract
Cardiovascular disease (CVD) continues to be a leading cause of death worldwide. Because regular physical activity (PA) independently decreases the risk of coronary heart disease (CHD) while also having a positive, dose-related impact on other cardiovascular (CV) risk factors, it has increasingly become a focus of CHD prevention. Current guidelines recommend 30 min of moderate-intensity PA 5 days a week, but exercise regimens remain underused. PA adherence can be fostered with a multilevel approach that involves active individual participation, physician counselling and health coaching, community involvement, and policy change, with incorporation of cardiac rehabilitation for patients requiring secondary prevention. Viewing exercise quantity as a vital sign, prescribing PA like a medication, and using technology, such as smartphone applications, encourage a global shift in focus from CVD treatment to prevention. Community-wide, home-based and internet-based prevention initiatives may also offer a developing pool of resources that can be tapped into to promote education and PA compliance. This review summarises the underlying rationale, current guidelines for and recommendations to cultivate a comprehensive focus in the endorsement of PA in the primary and secondary prevention of CHD.
Statistics from Altmetric.com
Introduction
Coronary heart disease (CHD) is the leading cause of death in men and women worldwide, responsible for 8.1 million deaths in 2013.1 As the global burden of CHD rises, prevention of heart disease has gained heightened medical attention, and aggressive lifestyle and pharmacotherapeutic interventions are increasingly being investigated. Several independent risk factors for the development of atherosclerotic cardiovascular disease (CVD) have been identified. Table 1 lists the major modifiable cardiovascular (CV) risk factors. Collectively, these account for ≥90% of the population attributable risk (PAR) of acute myocardial infarction (MI) in men and women. The first five risk factors in table 1 are responsible for ∼80% of the PAR.2 Accordingly, these nine risk factors provide feasible targets for CHD prevention.
Modifiable risk factors for coronary heart disease and associated risk of myocardial infarction
Physical activity (PA) is an independent and protective risk factor associated with reduced CV morbidity and mortality (OR 0.86, p<0.0001), conferring a PAR of 12.2% for acute MI. Regular PA also indirectly decreases disease risk by providing a gateway through which other risk factors can be favourably modified. Because >40% of the risk reduction associated with exercise cannot be explained by changes in conventional risk factors, a cardioprotective ‘vascular conditioning’ effect, including enhanced nitric oxide vasodilator function, improved vascular reactivity, altered vascular structure or combinations thereof, has been proposed.3 ,4 Data from the Behavioral Risk Factor Surveillance System show a slight increase in PA between 1988 and 2000, yet 25% of US adults report no participation in leisure-time PA.5 Physical inactivity is associated with an estimated 6% of CHD cases and a 0.68-year reduction in life expectancy.6 From 2006–2011, physical inactivity was associated with 11.1% of the aggregate healthcare spending in the USA. Inactive adults accounted for a 30% difference in mean annual US expenditure per capita compared with active adults ($1437 vs $713).7 This review examines seminal and recent studies to summarise the role of PA in the primary and secondary prevention of CHD.
Overview
PA involves bodily movements activated by skeletal muscles that expend additional calories relative to the resting state.8 The intensity of PA is objectively expressed as metabolic equivalents (METs). One MET indicates the amount of energy expended at rest and, for the average individual, represents an absolute and relative oxygen consumption of 250 mL/min and 3.5 mL/kg/min, respectively. An increase in oxygen consumption occurs as exercise intensity increases. PA may be quantified by using multiples of the resting energy expenditure, for example, 2 METs represents two times the resting oxygen consumption. Light activity corresponds to an intensity of <3 METs, moderate activity represents 3–<6 METs and vigorous physical exertion approximates >6 METs.8 ,9 Examples of light, moderate and vigorous activities are shown in table 2.10
Energy cost (METs) of common occupational and leisure-time physical activities
Primary prevention
The American Heart Association (AHA) and American College of Sports Medicine (ACSM) recommend at least 30 min of moderate-intensity PA 5 days/week, 20 min of vigorous aerobic exercise 3 days a week or combinations thereof, in addition to 2–3 days/week of resistance, flexibility and neuromotor exercises.11 To increase population PA, the US Preventive Services Task Force emphasises the effectiveness of clinician counselling.12 The Task Force recommends (Grade B) that overweight adults with CHD risk factors receive intense behavioural counselling.12 In contrast, medium- to high-intensity behaviour counselling—greater than 31 min of patient contact—by primary care physicians was associated with a small net benefit in patients without CHD, receiving a Grade C recommendation.13
The AHA recommends that clinicians use counselling interventions that include the following strategies: setting specific and short-term goals, providing feedback on progress, advocating strategies for self-monitoring, establishing a plan for frequency and duration of follow-up, using individually tailed interventions based on readiness to change and motivational interviewing and enhancing patient self-efficacy.14 Health coaching, in which dedication towards one's health is fostered via professional support and motivational interviewing, is generally well received and offers another approach to promote lifestyle changes.15 To increase and improve PA promotion within the healthcare system, a methodical structure should exist that motivates healthcare professionals to prioritise exercise, allows for realistic modifications and has strong advocacy from medical experts, leading scientific organisations and policy makers to endorse research and large-scale changes.16 In a time of rapidly evolving technology, pedometers/accelerometers, mobile applications and social media can all serve as accessible venues for increasing PA awareness, providing motivation and monitoring exercise progress.17
To help weave PA into routine outpatient visit dialogue, the ACSM and American Medical Association colaunched the non-profit initiative ‘Exercise is Medicine’ (EIM) in 2007.18 The campaign calls for PA to become standard of practice in healthcare, encouraging clinicians to evaluate their patients’ PA at every visit and ‘prescribe’ exercise at appropriate ‘dosages’. Healthcare systems, community resources and active health technology are the three modules suggested by EIM that establish the framework to promote international institutionalisation of exercise therapy; examples of recommendations stemming from each module include documentation of PA as a vital sign in the patient's medical record, referral to credentialled exercise professionals and using technology to track participation, respectively.18 Incorporating these suggestions we propose the algorithm in figure 1 for daily prescription of PA using the acronym ACTIVE.

Simplified approach to prescribing physical activity in daily practice for cardiovascular disease prevention using the acronym ACTIVE.
Effect on morbidity and mortality
Selected population studies have now demonstrated the relation between regular PA and reduced rates of CHD-related morbidity and mortality, as shown in table 3.19–22 Although PA plays an independent and additive role in the reduction of acute CV events, it also favourably modifies other CHD risk factors. With regular PA, systolic and diastolic blood pressures have been demonstrated to decrease by 2–5 mm Hg and 1–4 mm Hg, respectively, irrespective of baseline blood pressure levels. Moreover, regular PA was associated with reduced low-density lipoprotein (LDL) cholesterol levels (3.0–6.0 mg/dL) and non-high-density lipoprotein (HDL) cholesterol (6 mg/dL). Increased PA improves cardiorespiratory fitness (CRF), as well. In fact, PA functions as the strongest reversible element of CRF, showcasing the interlacing link between two CV markers also known to independently improve CVD risk profile.23 To achieve these cardioprotective benefits, an exercise regimen of 40-min sessions, three to four times weekly, and involving moderate-to-vigorous intensity PA is recommended American College of Cardiology (ACC)/AHA Class of Recommendation IIa, Level of Evidence B).6
Population studies evaluating the relationship between physical activity (PA) and coronary heart disease (CHD)/cardiovascular disease (CVD) risk
Secondary prevention
Cardiac rehabilitation
Exercise-based cardiac rehabilitation (CR) is the cornerstone for secondary prevention of CVD. CR comprises several core components, including baseline patient assessment, nutritional and psychosocial counselling, risk factor management, PA counselling and exercise training.24 In patients with CHD, CR is associated with a 13% and 26% lower all-cause and CVD mortality, respectively, in addition to a 31% reduction in hospital admissions at 12 months.25 CR participation is also associated with greater improvements in CHD risk factors, reduced angina symptoms and depression, improved exercise capacity and enhanced health-related quality of life (QOL).26–28 In patients with heart failure (HF) who are being optimally medically managed, exercise-based CR programmes confer an additional 11% reduction in all-cause mortality and hospitalisation, a 15% reduction in CV death and HF hospitalisation, and improved QOL.29–31 Given these significant benefits, most contemporary guidelines provide a Class I-level recommendation for referral to CR for eligible patients as delineated in box 1. However, in a recent study of 58 269 patients with acute MI and who were eligible for CR, only 62.4% were referred to CR at the time of hospital discharge and only 23.4% of all patients actually attended one or more CR sessions in the year postdischarge, suggesting vast CR underutilisation.32
Indications for cardiac rehabilitation
▸ Stable angina pectoris
▸ Myocardial infarction (non-ST-elevation myocardial infarction (NSTEMI) or ST-elevation myocardial infarction (STEMI)) within the past 12 months
▸ Undergone cardiac surgery (coronary artery bypass grafting (CABG), valve replacement/repair or heart/heart-lung transplant) or percutaneous coronary intervention (PCI)
▸ Systolic heart failure
Pre-exercise screening
A careful history and physical examination are important to ensure that patients with CHD do not have residual ischaemic symptoms, uncontrolled HF or threatening arrhythmias that may be triggered by vigorous exertion. The risks for these adverse events decrease significantly after the CV event, allowing patients to safely enrol in CR as early as 1–2 weeks after hospital discharge.33
Prior to prescribing PA for patients with CHD, physicians should assess the patients’ exercise tolerance. Peak or symptom-limited exercise testing should be considered to establish a baseline fitness level, determine the prescribed heart rate range for training, and evaluate for exercise-induced myocardial ischaemia or arrhythmias that may alter ongoing medical management.33 Patients should be continued on their usual medications during exercise testing to simulate the anticipated haemodynamic responses during exercise training.
Exercise recommendations
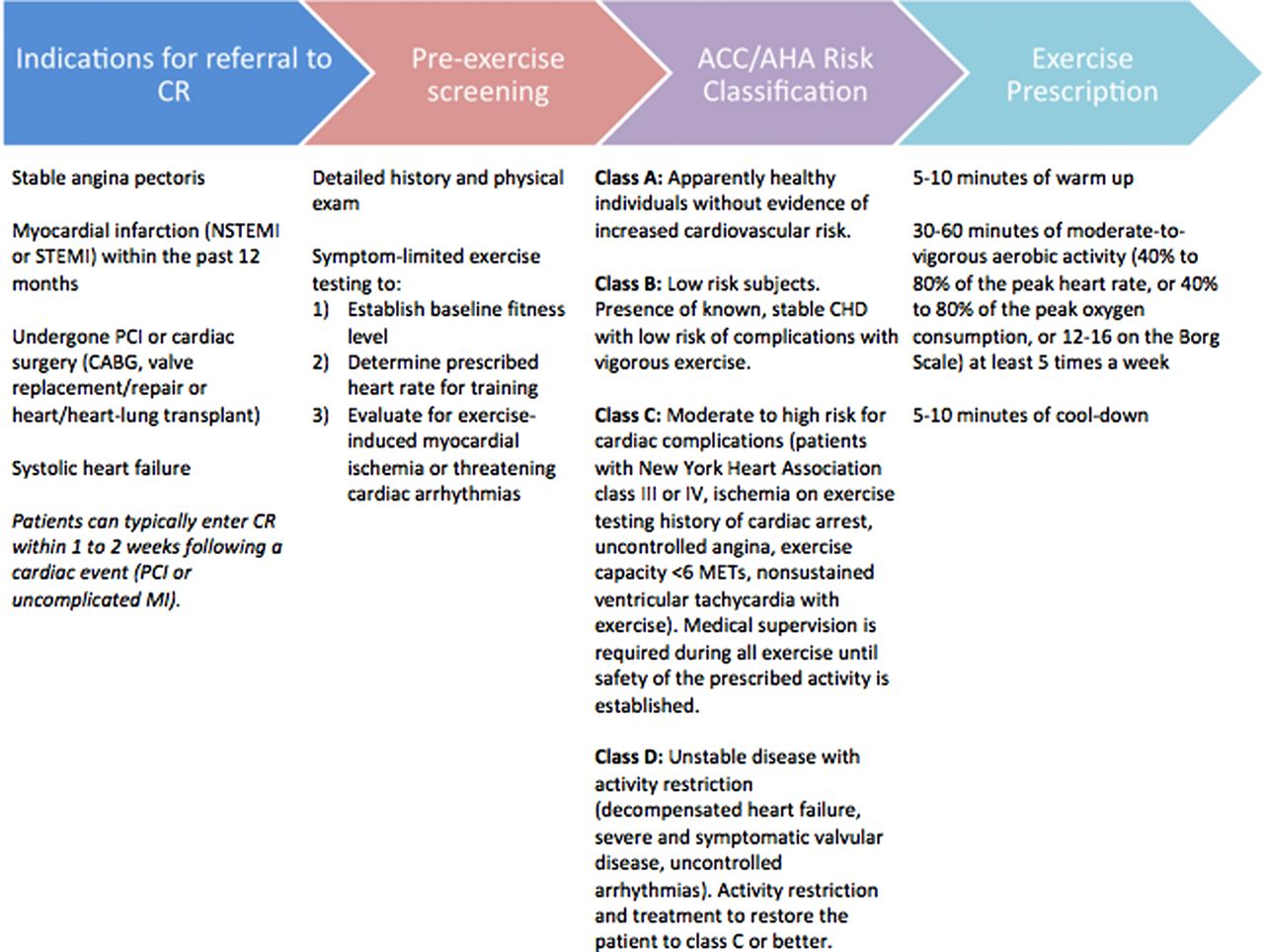
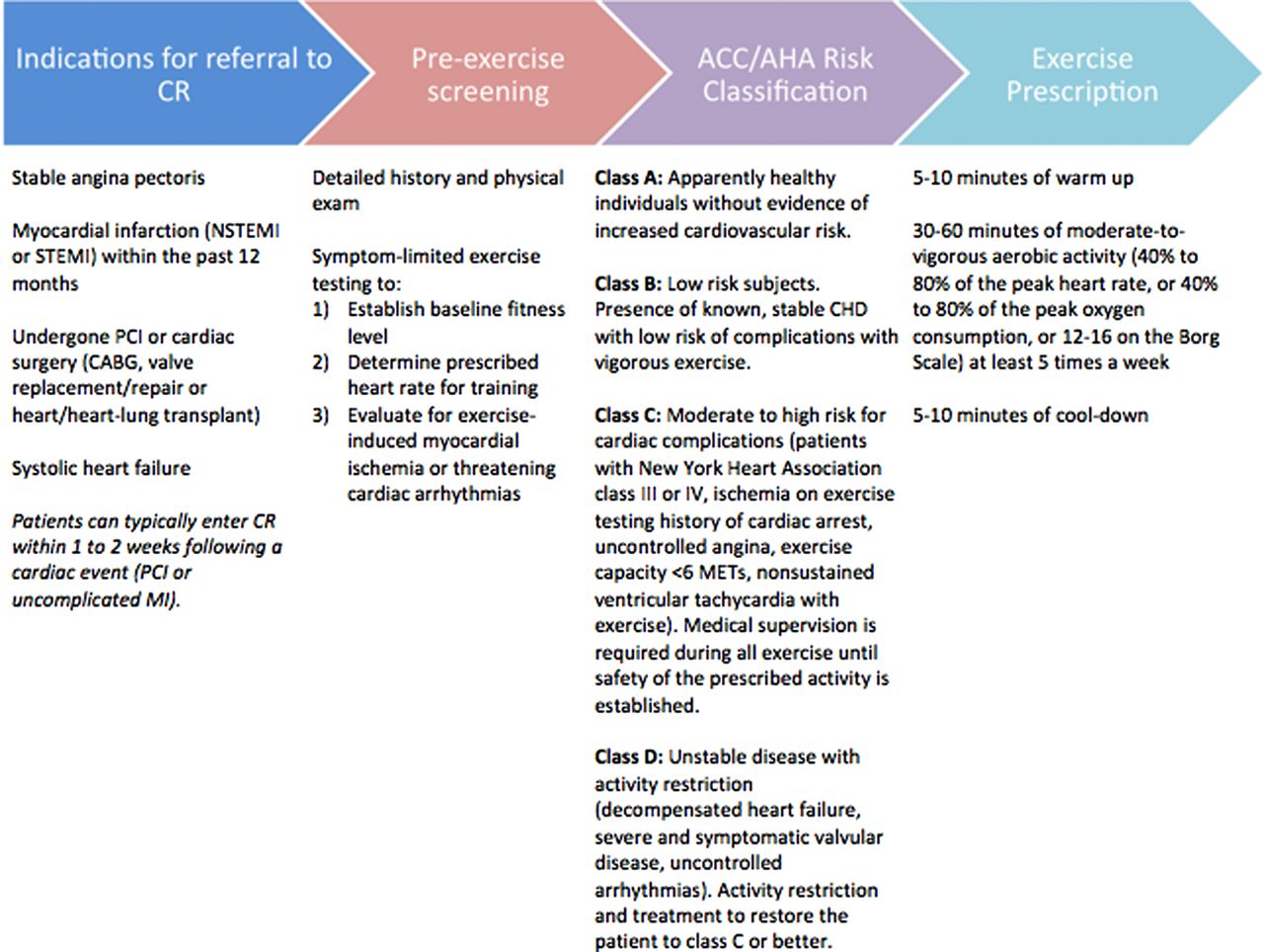
Recently discharged patients with CHD should be referred to CR for education, counselling and supervision, and monitoring of exercise training. After prescreening is completed to identify those in whom CR should be delayed or prohibited, the general recommendation for patients is 30–60 min daily of moderate-intensity PA for at least 5 days of the week and performed at an intensity of 40–80% of the peak heart rate.33 The subjective rating of perceived exertion using the Borg Scale can be employed as an adjunctive modulator of exercise intensity. For patients with ischaemic signs or symptoms during exercise, the intensity of exercise should be prescribed at a heart rate at least 10 beats below the ischaemic or angina threshold.33 While adverse CV events are rare, increased medical supervision is necessary for those patients with moderate to high risk of complications. A stable patient, however, can start CR as early as 1 week after discharge. Table 4 and figure 2 provide a summary of the general principles of exercise training prescription and the process of evaluating individuals for inclusion into a CR programme, respectively.
General principles of exercise training prescription
{kind=link}
{kind=link}
Exercise training for secondary prevention of cardiovascular disease. Indications for referral to cardiac rehabilitation and the general process of developing an exercise prescription for patients are outlined.
Due to the significant CV benefits of exercise, patients unable to attend supervised exercise sessions should continue to exercise independently. The recommended exercise intensity may be reduced to ∼60% to 75% of the peak heart rate to decrease the risk of MI or threatening arrhythmias.34 To still maintain the desired energy expenditure, the frequency or duration of exercise training may be increased. Another way of monitoring exercise intensity is to use the ‘talk test’, where patients are instructed to exercise at the highest intensity possible while able to maintain a comfortable conversation.33
Extreme exercise and CV outcomes: the reverse J-curve pattern
The graded cardioprotective benefit of regular PA is well established. Observational and epidemiological studies have generally focused on moderate to vigorous exercise intensities. In contrast, few data are available regarding the added health benefits, if any, associated with high volume and/or high-intensity endurance training regimens.35 Some studies suggest that extreme exercise may evoke acute elevations in troponin I and B-type natriuretic peptide and evidence of transient myocardial dysfunction.36 These data and other reports raise the possibility that excessive exercise may have some acute and/or chronic adverse effects.37
Recent studies in patients with CHD examined the dose-response relation between exercise and CV-related mortality during long-term follow-up.38 ,39 Regular walking or running were associated with progressively lower CV mortality up to a point, beyond which much of the survival benefit was lost. Two major findings emerged from these investigations: (1) the least physically active cohorts were at the highest risk for CV and all-cause mortality; and, (2) the most physically active subsets (those performing high-intensity exercise at the greatest weekly dosage) were at increased risk of CV mortality as compared with more moderately active individuals. Similar studies focusing on healthy populations have now reported comparable patterns for exercise and mortality.40 ,41 These findings suggest there is the potential for a plateau or even a decline in benefit at more extreme levels of endurance exercise, with heightened risks for acute CV events.37 Clinicians refer to this as a reverse J-curve or U-curve pattern, where it is preferable to be in the middle of the distribution. However, while the general consensus of the data suggests that ‘more is not always better’, additional data are needed to determine if ‘more is actually worse’ regarding exercise dose and the risk for CV events.42
Moderate continuous versus high-intensity aerobic interval training
Recent studies have compared the effectiveness of moderate-intensity continuous exercise training versus high-intensity interval training on changes in aerobic capacity and measures of CV function in coronary patients with and without postinfarction HF who were being optimally medically managed. Wisloff et al43 randomised 27 patients with stable postinfarction HF to either moderate continuous training (70% of peak heart rate) or high-intensity aerobic interval training (95% of peak heart rate) three times per week for 12 weeks or to a control group that received standard advice regarding PA. Improvements in CRF (46% vs 14%, p<0.001), left ventricular remodelling and brachial artery flow-mediated dilation (endothelial function) were greater with high-intensity aerobic interval training than moderate continuous training. Interval training seems more effective than continuous exercise for the improvement of aerobic capacity in CHD, but additional long-term studies assessing safety, compliance, and morbidity and mortality following interval training are needed.44
Risks of PA
The potential risks of PA should also be considered when physicians prescribe exercise to their patients. Although the most common risk is musculoskeletal injury, unaccustomed vigorous PA can trigger adverse CV responses, including acute MI, malignant arrhythmias and sudden cardiac death. While musculoskeletal and CV complications from exercise increase with higher intensity PA, regular exercise and enhanced CRF unequivocally confer partial protection against them.45 ,46 When previously sedentary patients initiate an exercise programme, level walking (2–3 METs) should be strongly recommended, gradually increasing the walking speed or intensity of exertion over time (2–3 months), provided they remain asymptomatic. This ‘progressive transitional phase’ decreases injury and increases CRF without going through a period during which each bout of vigorous exercise is associated with large spikes in relative CV risk.47 The safety of contemporary exercise based CR programmes is well established, with a reported incidence of cardiac arrest and death approximating 1 in 115 000 and 1 in 750 000 patient hours of participation, respectively.25 ,26 ,33
Prevention initiatives
While the evidence showcasing the health benefits of PA is bountiful, the knowledge must be intelligently applied for successful PA promotion to take effect. The aforementioned EIM uses a new philosophy of viewing PA as a multidisease targeting pharmaceutical equivalent that should be monitored and re-dosed as needed during clinic visits in order to encourage patients and physicians to adopt a mindset that exercise is indeed medicine. In addition to EIM, other US-wide campaigns exist to promote utilisation of PA and negative consequences from inactivity. A multilevel intervention that stretches from individuals (eg, establishment of personal goals) to community programmes (eg, better school physical education) to state/national policies (eg, community scale urban design with additional parks, trails and recreational areas) is more beneficial for producing positive change than individual approaches.48 Interventions aimed at increasing the percentage of individuals meeting contemporary PA guidelines can be grouped into community-wide, home-based and internet-based programmes.
Community-wide programmes
Community-wide programmes target general populations and involve broad interventions, including communication through media, health screening and education, and substantive modifications to the community environment and public health policies. A systematic review evaluated 10 studies and found that community-wide programmes led to overall increases in PA, number of active residents and associated energy expenditure.49 However, a 2015 Cochrane review of 33 studies involving varied interventions and exercise intensities found no evidence to support community-wide programmes for increasing population PA levels.50 Notably, the four studies identified as low-risk for bias found no effect of community-wide interventions.50
Home-based programmes
Home-based interventions are varied in nature but often involve an initial educational session and subsequent contact by phone or letter.51 A 2013 Cochrane review analysed nine studies measuring self-reported PA with at least 12 months follow-up and found a moderate and significant pooled effect for remote interventions.51 Only two of those studies included assessments of CRF, of which one found no significant difference between groups. Yet, the pooled effect was moderate and positive.51–53
Internet-based programmes
Internet-based initiatives represent another emerging area of growth. One meta-analysis of 34 randomised control trials compared internet-based initiatives for increasing PA with usual-care control groups.54 Although these studies were limited by short follow-up times (range 2–52 weeks, median 12 weeks) and publication bias, a small but significant effect was noted at 6 months.54 A subsequent review included non-randomised and randomised-controlled trials, experimental studies lacking control groups, and single-group observational studies.55 The intervention duration ranged from 2 weeks to 13 months (median 12 weeks). Forty-four of the 72 studies (61.1%) reviewed reported significant increases in PA after the intervention. However, only 6 of the 16 studies (37.5%) that included extended post-intervention follow-up demonstrated increased PA levels that were maintained.55 Additional studies are needed to clarify the effectiveness of these interventions.
Conclusion
Although data support PA as a bona fide preventive and therapeutic CV intervention, incorporating exercise into a comprehensive care plan remains largely neglected in contemporary medicine. Patients at risk for CHD should be identified early, risk stratified and offered a prevention programme that includes structured exercise and increased lifestyle activity. Enhancing the PA and CRF of our patients will require innovative strategies to adapt to their increasingly busy lifestyles and commitment on a community and national level. More research is needed to understand how internet, cellular and smartphone applications, along with home, work and community-based programmes, can be appropriately prescribed to optimise adherence and CV outcomes. As healthcare accessibility increases, our approach to CHD prevention and management must evolve to encompass pharmacological, interventional and lifestyle modifications in the treatment armamentarium.
References
Footnotes
Contributors TV, WMS, AAM, CTL and PBS wrote the review and constructed the figures/tables. DJE, NFG, BAF and LSS provided critical revision to the paper. All authors agree with the content of this manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.