Article Text

Abstract
Objectives The Professional Rugby Injury Surveillance Project is the largest and longest running rugby union injury surveillance project globally and focuses on the highest level of rugby in England.
Methods We examined match injuries in professional men’s rugby over the period 2002/2003 to 2018/2019 and described trends in injuries over this time.
Results Over the period 2002/2003–2018/2019, 10 851 injuries occurred in 1 24 952 hours of match play, equating to a mean of 57 injuries per club per season and one injury per team per match. The mean incidence, severity (days absence) and burden (days absence/1000 hours) of injury were 87/1000 hours (95% CI 82 to 92), 25 days (95% CI 22 to 28) and 2178 days/1000 hours (95% CI 1872 to 2484), respectively. The tackle accounted for 43% injuries with running the second most common activity during injury (12%). The most common injury location was the head/face with an incidence of 11.3/1000 hours, while the location with the highest overall burden was the knee (11.1 days/1000 hours). Long-term trends demonstrated stable injury incidence and proportion of injured players, but an increase in the mean and median severity of injuries. Concussion incidence, severity and burden increased from the 2009/2010 season onwards and from 2011 to 2019 concussion was the most common injury.
Conclusion The rise in overall injury severity and concussion incidence are the most significant findings from this work and demonstrate the need for continued efforts to reduce concussion risk as well as a greater understanding of changes in injury severity over time.
- rugby
- injury
- epidemiology
- prevention
Data availability statement
All publicly available data are included in the article or uploaded as online supplemental information.
Statistics from Altmetric.com
Introduction
Rugby Union (herein referred to as ‘rugby’) is a field-based collision team sport comprising both low-intensity and high-intensity periods of exercise.1 In comparison to other team sports, the incidence and severity of injury in professional rugby is relatively high (83/1000 hours2 and 37 days per injury,3 respectively). The majority of previous injury surveillance studies in professional club rugby have been limited to one or two seasons3–5; Schwellnus et al 6 reported on five seasons of data. Multiple season, league-wide data are of substantially greater benefit, allowing injury trends to be examined as well as providing a larger sample size to give greater confidence in the data (especially when breaking injuries down into smaller injury categories). We aimed to examine match injuries in professional rugby over the period 2002–2019 and to describe trends in injuries over this period.
Methods
Participants
In the 2002/2003–2018/2019 seasons (August to June), a mean of 576 (SD:98, range: 413–763) players consented to participate in the study per season, with a total of 9213 player-seasons (3006 unique players). Data were collected from the 16 clubs (12 per season) in the top tier of English rugby with a mean squad size for the period of 48 players per season (range: 34 (2002/2003 season) to 64 (2018/2019 season)). Match exposure and injury data were recorded daily by club conditioning and medical staff as part of the Professional Rugby Injury Surveillance Project (which is mandated for all teams playing in the competition) and includes all match injuries from the Premiership, the National Cup and European Cups. Each team played 22 Premiership games each year with four teams involved in semi-finals and two in the final, while European and National Cup exposure was based on the success of English teams in those competitions. Individual informed consent was obtained from first-team eligible players on a yearly basis.
Procedures
From 2002/2003 to 2012/2013, data were collected using a paper-based format and then entered into a database at the host institution.7 From the 2013/2014 season, injury data were captured directly from the injury surveillance section of an online clinical electronic medical record keeping system, ‘Rugby Squad’ (The Sports Office, UK).7 For each injury reported, information including injury type, site, activity causing injury and severity was collected.7 An injury was defined as ‘any injury that resulted in a player being unable to take a full part in future rugby training or match play for more than 24 hours from midnight at the end of the day the injury was sustained’.7 Injury severity was defined as the number of days lost from match play or training, with the injury return date set as the day the player was deemed fully fit to play by the club medical staff, irrespective of whether a match or training was planned for that day.7 Match exposure was calculated as the number of matches per club multiplied by the number of players exposed (15), multiplied by the time exposed (1.33 hours (80 min)). Data capture was overseen by a lead researcher at the host institution, who implemented a quality control process to ensure all injury details were captured on a regular basis, as well as a validation of all reported match injuries using match report cards completed by match officials (as of the 2016/2017 season). This process conforms with the International Olympic Committee (IOC) consensus statement for injury epidemiology studies.8
Data analysis
Injury incidence was calculated as the count of injuries per 1000 player-match-hours (approximately 25 matches).4 9 Mean severity was calculated as the total sum of days absence divided by the total count of injuries, while median severity was calculated as the midpoint of the range of injury severities within the dataset. Both the mean and median were calculated to account for the potential skew in mean severity caused by a small number of long-term injuries. Injury burden was calculated as the product of mean severity and incidence to give the number of days absence per 1000 player-match hours.4 9 Incidence, severity and burden were calculated each season to identify trends over time. Injuries which led to a player retiring from the sport were included in the calculation of incidence but not severity, there were 118 such cases over the 16-season period. Injuries were subdivided into four categories; 2–7 day injuries, 8–28 day injuries, 29–84 day injuries and injuries greater than 84 days.7 Linear regression was used to identify meaningful trends over time. Significance was set at p ≤ 0.05, accompanied by 95% CI. To account for the multiple tests being undertaken, p values were adjusted using the false discovery rate method.10 All analyses were undertaken using IBM SPSS Statistics for Apple (V.24.0.0).
Results
Over the period 2002/2003–2018/2019, 124 953 player-hours of match exposure were recorded across 11 079 matches with 10 851 time loss match injuries captured. In total, 268 343 days were missed by players as a result of match injury, with 43% of players returning to full participation in 7 days or less, 63% in 14 days or less, 71% in 21 days or less and 77% in 28 days or less. Ninety-three per cent of players had returned within 84 days. On average, 54% of players sustained at least one injury each season (range: 39%–66%). The mean incidence of injury was 87/1000 hours (95% CI 82 to 92, range: 62–103). The mean and median severity of injury was 25 and 9 days, respectively (95% CI 22 to 28 and 8 to 10). The mean burden of injury was 2178 days per 1000 hours (95% CI 1872 to 2484).
Position
There was no significant difference in the incidence of injury in forwards compared with backs (89/1000 hours, 95% CI 86 to 92 compared with 83/1000 hours, 95% CI 80 to 86). The mean and median severity of injury in both positional groups was 25 days (95% CI 24 to 25) and 9 days (95% CI 8 to 10), respectively. The burden of match injuries was not different between forwards and backs (2186 days/1000 hours, 95% CI 1286 to 2547 compared with 2042 days/1000 hours, 95% CI 1744 to 2340).
Activity at the time of injury
Injuries associated with the tackle accounted for 43% of all injuries, with the next most common activity during injury being running (12%). Of the tackle-related injuries, 59% were to the player being tackled (21.6/1000 hours, 95% CI 20.8 to 22.4) and 41% to the tackling player (15.0/1000 hour, 95% CI 14.3 to 5.7)). The greatest burden of injury was to the player being tackled, followed by the tackling player (figure 1).

Injury burden as a function of activity causing injury for the seasons 2002/2003–2018/2019. The y-axis represents incidence (number per 1000 player-hours) while the x-axis represents mean severity (days absence).21 Green line: values to the left and below represent the under the 25th burden percentile, these are low-risk injuries. Orange line: values to the left and below represent the under the 50th burden percentile, these are low-medium risk injuries. Red line: values to the left and below represent the under the 75th burden percentile, these are medium-high-risk injuries. Values to the right and above the red line are the most high-risk injuries.
Injury location and type
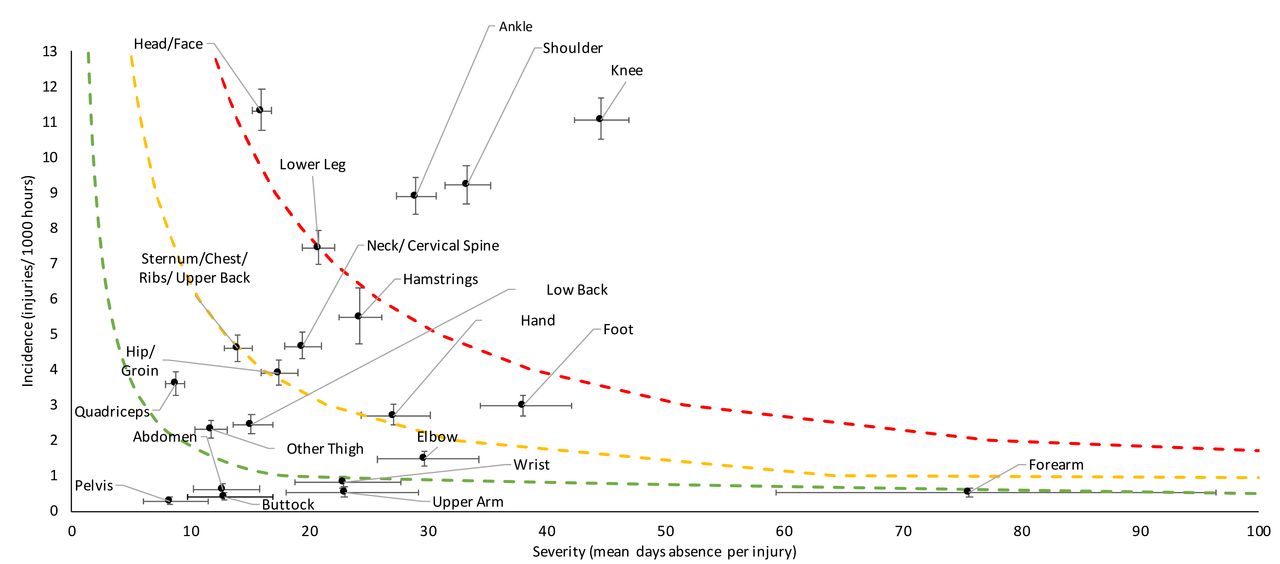
The body region with the highest incidence of injury was the lower limb (45/1000 hours, 95% CI 44 to 47), followed by the head/neck, upper limb and trunk (online supplemental table S4). The body region with the highest injury severity was the upper limb (32 days absence, 95% CI 31 to 34), followed by the lower limb, head/neck and trunk (online supplmental table S4). When divided into more location specific grouping, injuries to the head/face had the highest incidence (11.3/1000 hours: figure 2). Injuries to the forearm had the highest mean severity (76 days absence), but occurred infrequently (0.5/1000 hours, 95% CI 0.4 to 0.7). Knee injuries had the greatest burden (493 days per 1000 hours, 95% CI 413 to 573) as they were among the most common (11.1/1000 hours, 95% CI 10.5 to 11.7) and highest severity (45 days absence, 95% CI 42 to 47) injuries (figure 2). Of the three highest burden injury types, the tackle was the cause in 46% of ankle injuries, 45% of knee injuries and 66% of shoulder injuries.
Supplemental material
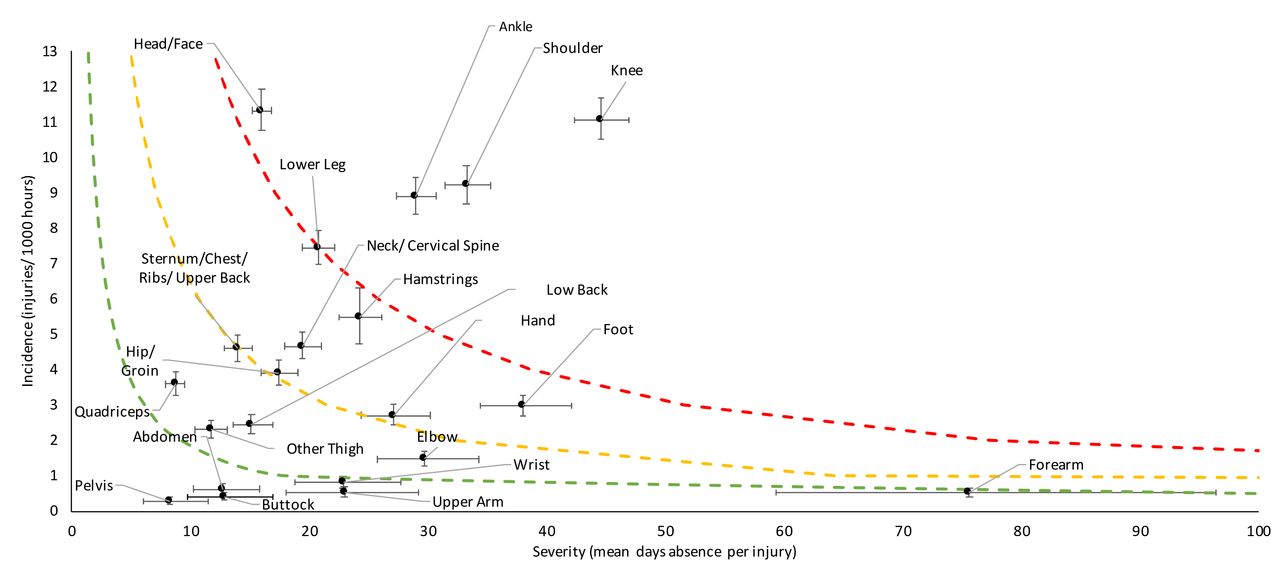
Injury burden as a function of body site for the seasons 2002/2003–2018/2019. The y-axis represents incidence (number per 1000 player-hours) while the x-axis represents mean severity (days absence). Green line: values to the left and below represent the under the 25th burden percentile, these are low-risk injuries. Orange line: values to the left and below represent the under the 50th burden percentile, these are low-medium risk injuries. Red line: values to the left and below represent the under the 75th burden percentile, these are medium-high-risk injuries. Values to the right and above the red line are the most high-risk injuries.
The injury type with the highest incidence was sprains and ligament injuries, which were also the highest burden with an incidence of 22.6/1000 hours (95% CI 21.8 to 23.4) and a severity of 30 days (95% CI 29 to 31). The next highest burden injuries were muscle injuries followed by fractures (online supplemental figure S5). The most severe injury type was dislocation/subluxation, with a mean severity of 74 days (95% CI 65 to 83).
Trends in match injuries from the 2002/2003 to 2018/2019 season
Table 1 reports the trends in match injury data from 2002/2003 to 2018/2019. The incidence (figure 3A) of match injury was stable, while the mean severity (figure 3B), median severity (figure 3C) and burden (figure 3D) of match injuries rose significantly.

{kind=link}
{kind=link}
{kind=link}
Trends in match injury incidence (A), mean severity (B), median severity (C), burden (D), proportion (E). No data were collected during the 2004–2005 season. Dotted grey lines represent 2 SD from the mean for the whole period (depicted by grey dashed line).
Long term trends in match injury in rugby (2002/2003 to 2018/2019 seasons)
The 2–7 days injury severity category had the highest incidence of injury (38/1000 hours, 95% CI 37 to 39; online supplemental table S3), however, this significantly decreased over time (table 1). The incidence of injury in the 7–28 days severity category was stable with an incidence of 30/1000 hours (95% CI 29 to 31, online supplemental table S3). The incidence of injury in the 28–84 day severity category was 13/1000 hours (95% CI 13 to 14, online supplemental table S3), while the incidence of the greater than 84 day injuries was 6/1000 hours (95% CI 5.6 to 6.4, online supplemental table S3). Both of these severity categories significantly increased over time (table 1).
We calculated the incidence, severity and burden of concussion (online supplemental figure S2). Concussion incidence, mean severity, median severity and burden all increased significantly (table 1), with a steep annual rise in the incidence and burden from the 2011/2012 season onwards (online supplemental figure S2A and D). Mean concussion severity increased annually from the 2013/2014 season, (online supplemental figure S2B) while median severity increased annually from 2014/15 (online supplemental figure S2C). Over the period 2002/2003–2018/2019, the mean number of concussions per club per season was 6, however this ranged from two per club (2005/2006) to 14 per club (2016/2017).
The incidence of non-concussion injuries decreased (ß: −1.25, 95% CI −2.50 to −0.01, p=0.06, online supplemental figure S6). In contrast, the severity of all injuries (excluding concussions) increased significantly (ß: 1.74, 95% CI 1.40 to 2.08, p<0.001, online supplemental figure S7).
Examining the activities causing injury with the highest burden demonstrated no significant change in the incidence in tackle (ß: 0.73, 95% CI −0.05 to 1.51, p=0.07) or ruck (ß: 0.10, 95% CI −0.08 to 0.28, p=0.25). However, there was a significant decrease in the incidence of running related injuries (ß: −0.31, 95% CI −0.57 to −0.05, p=0.02). Over time, the number of tackle related injuries at the ankle rose significantly (ß: 1.17, 95% CI 0.10 to 2.25, p=0.03), with no significant change at the knee (ß: 0.01, 95% CI −0.78 to −0.80, p=0.99) or shoulder (ß: −0.08, 95% CI −0.85 to 0.70, p=0.83). The incidence of injuries to the hamstrings decreased significantly (ß: −0.14, 95% CI −0.24 to −0.04, p=0.01), however, the severity of hamstring injuries increased (ß: 1.00, 95% CI 0.45 to 1.54, p=0.001), with no significant increase in burden (ß: 2.27, 95% CI −1.11 to 5.64, p=0.17).
Discussion
This is the longest running and largest injury surveillance study in professional rugby, capturing nearly 125 000 hours of match exposure and 10 851 time loss match injuries over 16 seasons between 2002/2003 and 2018/2019. This equates to a mean of 57 injuries per club per season and 1 injury per team per match. The incidence of injury was stable, while mean severity, median severity and injury burden rose significantly. Concussion incidence, severity and burden also all rose significantly. The lower limb was the most commonly injured body region; the knee represented the anatomical region with the highest injury burden. The tackle was the game event most commonly associated with injury contributing 43% of all injuries (25% player being tackled, 18% tackling player).
Trends in match injury
A key benefit of longitudinal injury surveillance is the ability to track trends in injury over time. Over the 16 season period, the overall incidence of injury did not change, however, the incidence of injuries excluding concussion decreased by a mean of 1.2/1000 hours each year (online supplemental fgure S7). The incidence of injury (87/1000 hours) was higher than that in professional rugby in Australia (66/1000 hours3), but lower than South Africa (100/1000 hours6). The severity of injuries increased over time, with an injury on average lasting 1.2 days longer per year (including concussions) and 1.7 days longer per year (excluding concussion). Mean severity of injury in this study was lower (25 days) compared with Australian professional players (40 days3).
Explaining the changes demonstrated in this study is difficult, in part because the game has evolved, with more contact events occurring in tackles and rucks.11 Both of these match events are considered among the highest burden events (figure 1), given their unpredictable nature and high speed contact. Over the same period, exposure to lower burden events such as scrums and lineouts has declined.11 Other possible reasons for the changes in injury severity and burden include the increasing mass and stature of players12 as well as improvements to injury surveillance processes (improving the reporting (capture) of injuries). We note that increasing severity (longer time to return from injury) will follow if clinicians employ more conservative return to play strategies.13 Whether changes to the game or more conservative management strategies are the driving force behind the rise in severity is unknown—we speculate that both are likely at play. Injury surveillance alone cannot determine the causal nature of this change, and different study designs are required to answer this question. Further research might incorporate mixed methods (both qualitative and quantitative) to establish the causes of increasing severity of injury.
Concussion
While concussion was not the focus of this study, it has emerged as the most common injury in rugby since 2011. The study mean concussion incidence does not portray the changes in concussion reporting over time, nor the potential importance of changes in concussion recognition tools and more conservative return to play strategies. In our study, concussion increased in incidence, but also in severity and thus burden (online supplemental figure S2) and this extends findings reported in other elite rugby settings.6
In an effort to improve concussion recognition and management a number of tools have been introduced, including an off-field in-game assessment as part of the Head Injury Assessment (HIA) protocol14 in 2012/2013, real-time pitch-side video review for medical staff of head injury events in 2017 and the introduction of independent match day doctors to identify significant head injury events and supervise the application of the HIA protocol in 2018. We opine that these interventions increased clinicians’ recognition of concussion in professional rugby, however it is still to be determined whether the increase in reported concussions is due to this awareness alone, or due to an increase in the rates of concussion itself.15 It is incontrovertible that the current rates of concussion in professional rugby are consistently high (accounting for an average of 21% of all injuries in the five seasons from 2014/2015 to 2018/2019) and governing bodies should continue to investigate strategies to lower the risk.
Activity causing injury: tackles and more
The most common activity causing injury was the tackle (43% of all injuries, 25% to the player being tackled, 18% to the tackling player: figure 1). This mean figure is slightly lower than those documented in South Africa, with 50% of all injuries linked to the tackle in that setting,6 however, the yearly proportion in this study ranged from 36% to 52%. The tackle accounts for an injury burden of 987 days absence per 1000 hours of match play, which is nearly four times higher than the next highest burden activity (running: 270 days absence/1000 hours, figure 1). Nevertheless, efforts to reduce the injury risk in the tackle are hampered by the frequency and dynamic and unpredictable nature of this game event. Despite this, several law variations for reducing the risk of injury in the tackle are being considered,16 with one law variation to reduce the legal height of the tackle having been evaluated in the second tier of professional rugby in England.17 With a lower legal tackle height, incidence of all injuries did not change and neither did overall concussion incidence, but the incidence of concussion while tackling increased, which demonstrates the challenges associated with improving safety in this high risk component of the game. While the focus of many injury prevention strategies have been on concussion, it must not be overlooked that the three highest burden injury locations in rugby are the ankle, knee and shoulder (figure 2). Given that a high proportion of injuries to these body locations are associated with the tackle (ankle: 46%, knee: 45% and shoulder 65%), investigations and injury prevention strategies targeted at these sites should be considered alongside those specific to concussion.
Running and the ruck make up the second and third highest burden activities causing injury in rugby, with the incidence of running injuries decreasing significantly over the study period (figure 1). No significant changes have occurred in the incidence of ruck related injuries; however, given recent evidence suggesting inconsistent law application in the professional game,18 this may be an area that could benefit from an injury prevention focus.
Limitations
We acknowledge several limitations. Over the course of the 16 seasons in this study, the project has been led by a number of researchers using a number of methods in line with the consensus statement for injury surveillance in rugby union.7 We aimed to ensure the continuity of methods among researchers over this time period but it is likely that small systematic changes occurred over time.
Larger changes in the system include the change from a paper-based recording system to a web based platform in 2012, as well as the change from a three digit Orchard code (OSICS-8) to a four digit Orchard code (OSICS-10).19 One of the difficulties associated with studies of this type is validating the data input into the system (while avoiding double entry of data).20 To address this, a number of quality control processes have been added to the data collection. During each match, a match report card is completed by an official, which notes the reasons for substitutions (tactical, injury, blood substitution, HIA, etc). These report cards are cross-referenced against match injuries entered into the database to ensure that all injuries sustained are captured. Furthermore, concussions reported in the database were crosschecked with CSx (concussion management mobile application) data to ensure all concussions are logged correctly. Finally, before data were analysed, all injuries were checked for duplicates and inconsistencies. We gained final approval of the included injuries from the medical lead in each club. These practices ensure data quality and are in-line with those included in the 2020 IOC consensus statement on injury surveillance.8
Summary and conclusion
Over the course of 16 seasons, the incidence of injury remained stable, while injury severity and burden rose steadily. Our study provides insight for future investigation into specific areas of interest, including activities such as the scrum, ruck and tackle as well as specific injury types such as concussion. These data provide an important resource for practitioners working within the sport, as to the most common and highest burden injuries.
We call for studies examining the specific types and activities causing injury associated with commonly injured body locations such as the knee, shoulder and ankle. We also call for continued support from all stakeholders for this important prospective study which informs injury prevention strategies and thus, has the potential to influence player welfare in professional rugby.
What are the findings?
This is the largest injury surveillance study globally in professional rugby union, with nearly 11 000 injuries recorded over a 16-season period.
Injury incidence and the proportion of players injured each year remained stable between the 2002/2003 and 2018/2019 seasons.
Between the 2002/2003 and 2018/2019 seasons, there was a significant rise in the mean and median severity of injuries.
The incidence, severity and burden of concussion rose dramatically between 2010/2011 and 2016/2017.
How might it impact on clinical practice in the future?
Identifies the need for more focused studies examining specific body locations including the knee, ankle and shoulder.
Provides medical teams with expected injury rates and severities for rugby related injuries, to inform interdepartmental return to play strategies within clubs.
Supports the ongoing need for injury prevention strategies to mitigate risk in the tackle.
Data availability statement
All publicly available data are included in the article or uploaded as online supplemental information.
Ethics statements
Ethics approval
The study was subject to ethical approval from the host academic institutions (University of Leicester (2002–2007), University of Nottingham (2007–2012) and University of Bath (2011–2019).
Acknowledgments
The authors would like to thank the medical and sport science staff at each of the Premiership clubs who partook in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @westy160991, @drsimonkemp, @drkeithstokes
Correction notice This article has been corrected since it published Online First. Typographical errors within the title have been corrected.
Contributors Each of the authors was involved in the original conception of the paper, data collection process, analysis of results and interpretation of findings. SWW and LS drafted the original manuscript and all other authors provided significant feedback and comments in refining the final manuscript.
Funding This project was funded by the Rugby Football Union and Premier Rugby.
Competing interests SK and KAS are employed by the Rugby Football Union. MC is employed by Premier Rugby.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research; however, the project steering group includes a range of stakeholders and practitioners.
Provenance and peer review Not commissioned; externally peer reviewed.