Article Text

Abstract
Objective To identify and quantify determinants of anxiety symptoms and disorders experienced by elite athletes.
Design Systematic review and meta-analysis.
Data sources Five online databases (PubMed, SportDiscus, PsycINFO, Scopus and Cochrane) were searched up to November 2018 to identify eligible citations.
Eligibility criteria for selecting studies Articles were included if they were published in English, were quantitative studies and measured a symptom-level anxiety outcome in competing or retired athletes at the professional (including professional youth), Olympic or collegiate/university levels.
Results and summary We screened 1163 articles; 61 studies were included in the systematic review and 27 of them were suitable for meta-analysis. Overall risk of bias for included studies was low. Athletes and non-athletes had no differences in anxiety profiles (d=−0.11, p=0.28). Pooled effect sizes, demonstrating moderate effects, were identified for (1) career dissatisfaction (d=0.45; higher anxiety in dissatisfied athletes), (2) gender (d=0.38; higher anxiety in female athletes), (3) age (d=−0.34; higher anxiety for younger athletes) and (4) musculoskeletal injury (d=0.31; higher anxiety for injured athletes). A small pooled effect was found for recent adverse life events (d=0.26)—higher anxiety in athletes who had experienced one or more recent adverse life events.
Conclusion Determinants of anxiety in elite populations broadly reflect those experienced by the general population. Clinicians should be aware of these general and athlete-specific determinants of anxiety among elite athletes.
- anxiety
- athlete
- elite performance
- injury
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Combined anxiety disorders affect the general population at an estimated (past 12 month) rate of 10.6%–12.0%,1 2 with broadly similar rates suggested among elite athlete populations (8.6%),3 defined as those competing at professional, Olympic or collegiate/university levels. Anxiety disorders are characterised by emotional responses associated with fear, apprehension, worry and tension in response to an actual or perceived threat.4 Anxiety modulates attentional networks, resulting in compromised executive function, stimulus processing and information selection5—all important domains for elite competition. While commonalities are present, diagnostic systems differentiate anxiety subtypes, such as generalised anxiety disorder (GAD) or social anxiety disorder.4 Additionally, anxiety can be a situationally or event-dependent transitory state (eg, state anxiety), or a relatively stable personality characteristic (eg, trait anxiety). State anxiety symptoms are more likely to occur in situations perceived as threatening.6
Athlete-specific factors may precipitate or exacerbate anxiety disorders, including pressures to perform and public scrutiny,7 career uncertainty or dissatisfaction,8 9 and injury.10–12 General psychosocial factors are also strongly implicated in the onset and maintenance of anxiety disorders within the general population. These include behavioural inhibition, social withdrawal or avoidance, and cognitive patterns of rumination.13 A recent meta-analysis found that female gender, younger age and lower athletic experience were associated with higher competitive anxiety in athletes14; however, the specific determinants of anxiety disorders in elite athlete populations has not yet been reported. Identification of putative subgroup differences may assist with early identification and indicated prevention efforts in this population, improving the timely management of anxiety disorders among elite athletes. The objective of this study was to perform a systematic review and meta-analysis to identify, quantify and analyse determinants of anxiety symptoms experienced by elite athletes.
Method
The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Search strategy
A systematic search strategy was developed by an experienced academic librarian (MEH). The search was executed in the PubMed, SportDiscus, PsycINFO, Scopus and Cochrane databases from inception until November 2018. The search strategy and MeSH terms are presented in online supplementary table 1. Citations were independently screened by SMR, RP and KG.
Supplemental material
Study inclusion
Studies were selected if they included (1) data on elite athletes, including para-athletes, defined by standard of performance level,15 competing at the professional (and professional youth, ie, members of elite sports schools), Olympic and collegiate/university levels; (2) a symptomatic or diagnostic anxiety outcome measure (as per the Diagnostic and Statistical Manual of Mental Disorders [DSM-5]4 criteria) in relation to GAD, specific phobia, social anxiety, panic disorders or obsessive-compulsive disorder (OCD); and (3) currently competing or retired athletes (authors adopted a maximum mean retirement length of 10 years to allow investigation of effects between anxiety and longer-term sport-specific outcomes [eg, concussion],16 and account for, yet limit the effect of retirement).17
Study exclusion
Studies were excluded if they were not published in English, were a case study or case report, used a qualitative design, were review articles or were not refereed journal articles (conference abstracts were excluded), or focused solely on state-based performance or competitive anxiety (ie, included studies needed to report on a measure/diagnosis of symptom-level anxiety as per DSM-5).
Assessment of study quality
We assessed quality of studies with the Joanna Briggs Institute’s critical appraisal tools for systematic reviews.18 These tools are validated appraisal checklists specific to study design, capturing aspects of design quality, analysis and reporting. KG assessed studies using checklists for randomised controlled trials (RCTs), cohort studies, prevalence studies, cross-sectional studies and quasi-experimental studies. The appraisal score reported is the proportion of ‘yes’ responses on the total number of criteria. If a criterion was not applicable (N/A) to a given study, that item was not counted in the total number of criteria.
Data extraction
A standard template was designed for data extraction of study and sample characteristics including study design, aim, location, gender ratio, sport population, anxiety outcome and key findings. KG extracted the data and SMR reviewed them for consistency. For the meta-analysis, KG extracted a list of determinants of anxiety (associated variables) in each study to assess viability for meta-analysis. Once a determinant was identified, KG extracted the relevant quantitative data, while OS-E and SMR reviewed for consistency.
Data analysis (meta-analysis)
Pooled effect sizes were estimated using Comprehensive Meta-Analysis (CMA) software V.3.3.070.19 Raw data (mean, SD and n) were sourced for determinants of anxiety. When raw data were unavailable, we used effect size data (r, OR, t, β and F values). Overall effect sizes were estimated using the standardised difference in means (d) because this could be calculated for all types of extracted data. When we could not enter effect size data directly into CMA (eg, β, F and t statistics), transformations were made into an r statistic.20 21 All meta-analyses used the random-effects model to account for within-study error and between-study variation. Though a minimum of two studies are needed to perform a meta-analysis,22 CMA software requires at least three studies to perform publication bias analysis,23 hence we required three studies for inclusion in the overall (eg, non-subgroup) meta-analyses. An initial population comparison (elite athletes compared with non-athletes) was conducted, followed by analysis of the determinant variables.
Subgroup and sensitivity analysis
Where applicable, we conducted subgroup analysis to assess effect sizes across different anxiety outcomes (generalised, trait, diagnosis and global anxiety/depression) and playing status (current vs former). As subgroup analysis calculates an estimated effect size for each subgroup, a minimum of two subgroups with two contributing studies each were required to conduct a statistically sound analysis for a determinant.22 Additionally, sensitivity analysis was conducted when significant heterogeneity was observed. Sensitivity analysis is a repeat of the initial analysis which substitutes alternate inclusion or exclusion decisions to assess robustness of the results.24 Sensitivity analysis was calculated by removing any visual outliers or studies with dissimilar characteristics.
Interpretation of forest plots
A forest plot is a visual representation of the effect size for each study, represented by squares, and the overall estimated effect size, represented by a diamond. The side of the forest plot on which the effect size estimate falls indicates a higher anxiety score in that group. For plots with subgroup analysis, overall effect size estimates are reported in the text.
Heterogeneity and publication bias
The Q statistic measured the presence or absence of heterogeneity by testing the null hypothesis of no variation in true effect size across studies.25 Heterogeneity was assumed when the Q statistic was significant, as the null hypothesis of no variation is rejected. The I 2 statistic describes the proportion of variance in observed effects due to variance in true effects and can be interpreted as the percentage of variance that would remain if there was no sampling error.26 Low I 2 scores indicate lower heterogeneity. Publication bias was assessed using the Duval and Tweedie trim-and-fill funnel plot method.27 A funnel plot is a graphical representation of study size as a function of effect size; large studies generally appear at the top of the graph, close to the mean effect size, and small studies typically appear at the bottom of the graph, spread broadly around the mean effect size.28 Asymmetry in funnel plots (more studies falling to one side of the graph) indicates potential publication bias. To assess the scope of bias, the trim-and-fill method estimates the number of missing studies in an asymmetrical plot, balances it with the ‘fill’ of additional study points and recalculates the estimated effect size using the filled estimates.27
Results
Literature search
The database search returned 1163 articles (figure 1). After removal of duplicates, 1111 articles were screened for eligibility. Of the resulting 145 eligible articles, 61 were included in the narrative synthesis after full-text assessment. These articles are listed and grouped by anxiety outcome measure in table 1.
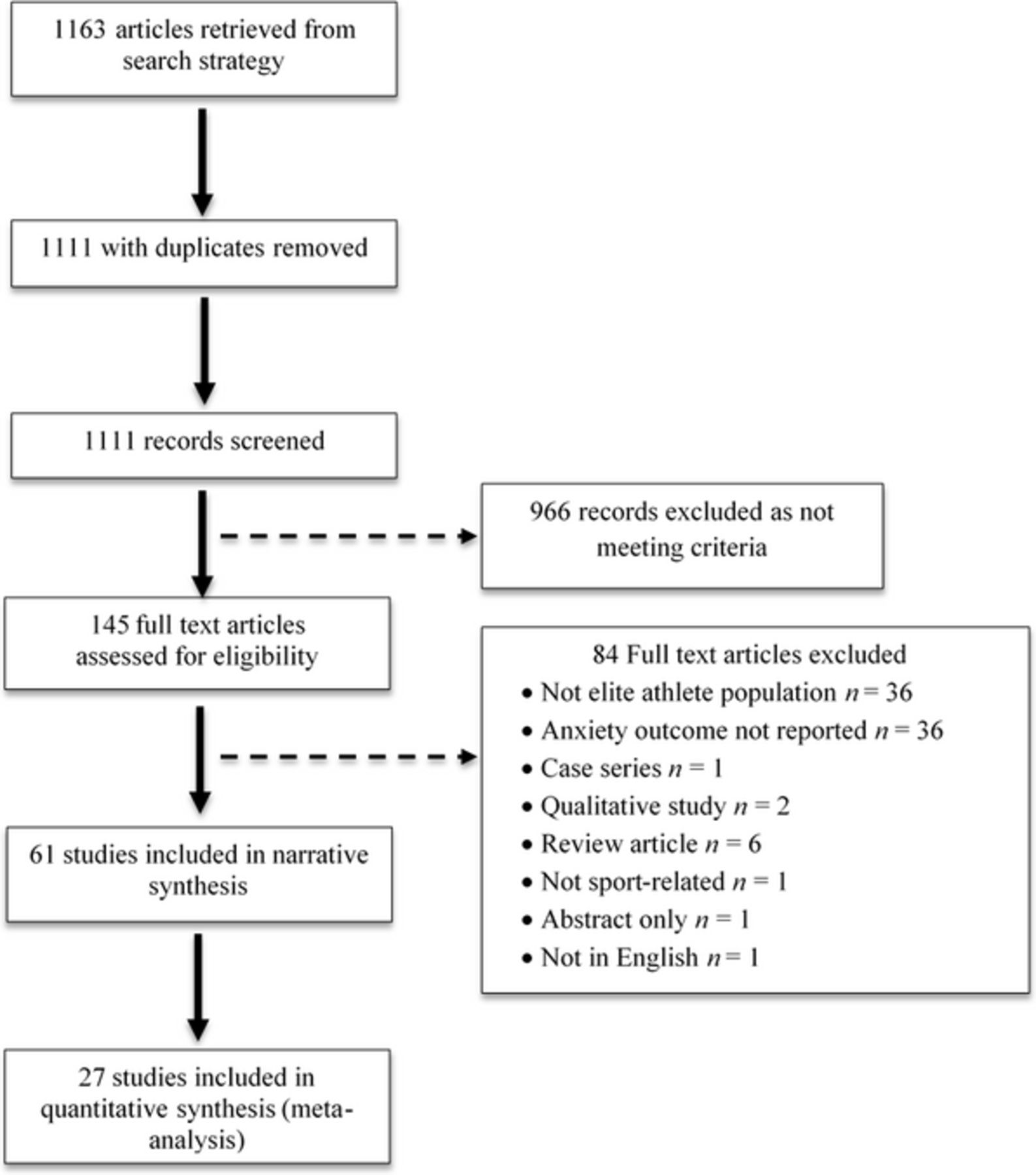
PRISMA study selection flow chart.
Included articles grouped by anxiety measure
Description of included studies
Table 2 summarises the study characteristics of the reviewed articles (see online supplementary table 2 for a detailed summary of study characteristics for each article). Of the 61 studies, 46 (75%) were published from 2014 onwards. Samples typically represented athletes from multiple countries (n=16, 26.2%). For single-location samples, the most common country was the USA (n=13, 21.3%), followed by Australia, France, Germany and Ireland with three studies each (5.0%). Italy, Korea, Spain, Sweden and Switzerland appeared twice (3.3%), and Canada, China, Denmark, Egypt, Israel, Netherlands, Norway, Tunisia, Turkey and the UK appeared once (1.6%).
Supplemental material
Summary of included article characteristics
Meta-analysis
Of the 61 articles, 27 (44%) were suitable for meta-analysis. After screening for determinants of anxiety, seven variables were identified: one population comparison (athletes vs non-athletes) and six determinant variables (gender, age, concussion, musculoskeletal injury, career dissatisfaction—typically measured as a dichotomous ‘yes/no’ variable, and recent adverse life events such as ‘death of close friend’ or ‘change in financial state’ within the past 6 months).
Five studies examined athletes compared with non-athletes.29–33 No differences in anxiety symptomology were observed between athletes and non-athletes (d=−0.11, p=0.28; see figure 2). Separate subgroup analysis of anxiety outcomes found no differences in generalised anxiety (d=−0.04, p=0.36) or trait anxiety scores (d=0.07, p=0.74). There was significant heterogeneity (p<0.01), which became non-significant after removal of two studies that had mixed sport samples (Q=5.810, p=0.06; d=−0.06, p=0.798). There was no evidence of publication bias.

Forest plot for anxiety in athletes and non-athletes.
Demographic determinants
Ten articles measured anxiety by gender.3 31 33–40 Overall, female athletes reported higher anxiety scores compared with male athletes (d=0.38, p<0.001). Moderate effect sizes were found across all anxiety measurement types (see figure 3). Homogeneity was upheld for the overall analysis and trait anxiety analyses, but not the general anxiety (p=0.047) or diagnosis analyses (p=0.045). Homogeneity was achieved for general anxiety after removing the only single-sport sample (Q=1.658, p=0.437; d=0.28, p<0.001),33 though could not be reached for diagnosis as there were only two contributing studies. No publication bias was detected.

Subgroup analyses for anxiety outcomes in male and female athletes.
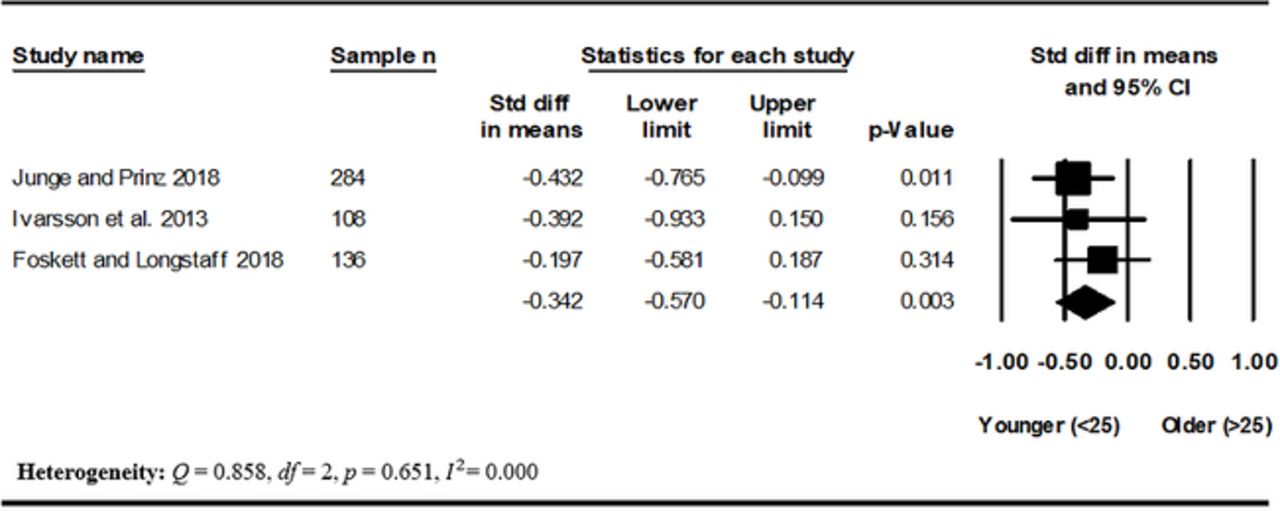
Three articles analysed anxiety by age.36 41 42 Younger athletes (<25 years) had higher anxiety levels compared with older athletes (>25 years; d=−0.34, p=0.003; figure 4). There were insufficient studies to perform subgroup analysis for anxiety outcomes. Heterogeneity and publication bias were not detected.

Forest plot for anxiety among athletes older and younger than 25 years.
Concussion and musculoskeletal injury
Four articles examined anxiety by concussion frequency and symptomology.43–46 Figure 5 denotes a non-significant effect of concussion (d=0.33, p=0.053). There was significant heterogeneity that became non-significant after visual inspection advocated removal of an outlier study.43 The removal of the study also led to a small significant effect (d=0.17, p=0.023), where athletes with concussion history showed higher anxiety symptoms. There was no evidence of publication bias in the initial analysis, though there was evidence after the outlier study was removed. Accordingly, these results should be interpreted cautiously.

Forest plot for anxiety in athletes with and without concussion history.
Nine studies measured anxiety by musculoskeletal injury prevalence.33 35 40 41 47–51 An overall significant small-moderate effect indicated injured athletes reported higher levels of anxiety (d=0.31, p<0.001). Subgroup analyses indicated significant effects across all anxiety outcomes (see figure 6). Homogeneity was upheld across all analyses. There was evidence of publication bias, marginally adjusting the estimated effect size (d=0.29).

Subgroup analyses for anxiety outcomes in injured and uninjured athletes.
Career dissatisfaction and recent adverse life events
Six articles analysed anxiety by career dissatisfaction.41 48 50–53 Athletes with higher ratings of career dissatisfaction reported higher global anxiety/depression scores compared with career-satisfied athletes (d=0.45, p<0.01; figure 7). Heterogeneity was observed, though became non-significant after the removal of the only study with a retired athlete sample (Q=6.348, p=0.175; d=0.55, p<0.001).53 Publication bias was detected, slightly reducing the estimated effect size (d=0.45).

Forest plot for anxiety in athletes with and without career dissatisfaction.
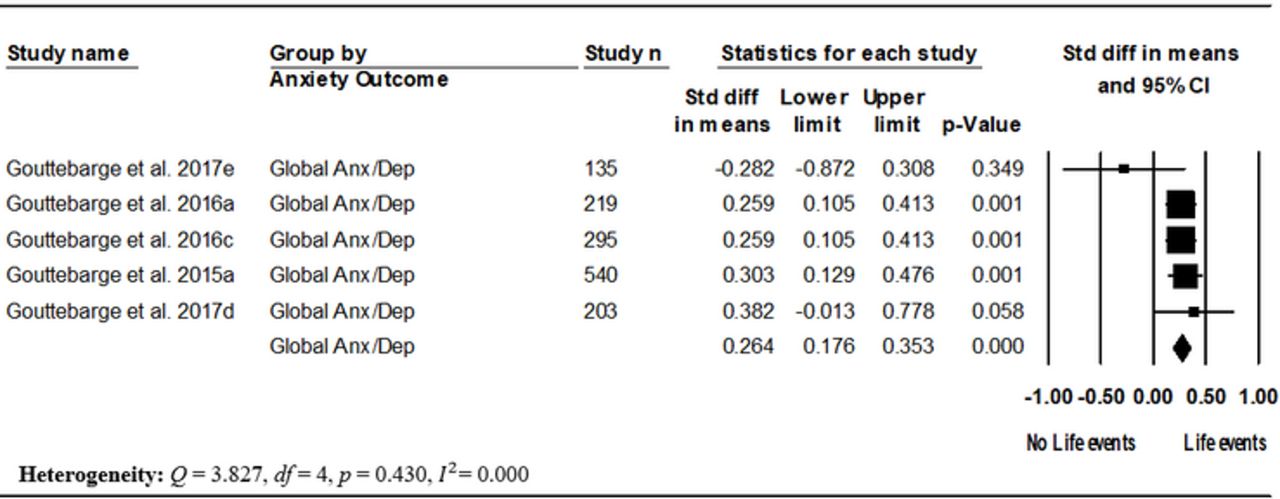
Five studies examined anxiety by recent adverse life events.50–54 Figure 8 shows a small effect of recent adverse life events on global anxiety/depression, where higher anxiety scores were found in athletes who had experienced one or more recent adverse life events (d=0.26, p<0.001). There was no evidence of heterogeneity or publication bias. Exploratory subgroup analysis of current versus former athletes found a small effect for former athletes (d=0.26, p<0.001, k=2),53 54 but not current athletes (d=0.23, p=0.113, k=3).50–52
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for anxiety in athletes with and without adverse life events within six months.
Narrative results
Online supplementary table 3 summarises key findings of each of the 61 articles. The following sections summarise other results not included in the meta-analysis.
Supplemental material
Comorbidities
Diagnosed comorbidity was found for GAD occurring with depression,42 and for multiple anxiety disorders occurring together, for example GAD occurring with OCD, with agoraphobia or with panic disorder.3 For symptomatology, higher anxiety scores were commonly associated with higher depressive symptoms.40 46 Self-reported history of mental health disorders was also associated with higher self-reported generalised anxiety symptoms in rugby players during a competitive season and training season.55 Comorbidity of common mental health symptoms (including global anxiety/depression) was examined across multiple studies; however, due to non-specific reporting, it cannot be determined if indicated comorbidity encompassed anxiety symptoms.12 44 48 50 51 56–61
Competitive level and experience
Elite athletes playing at higher competitive levels typically reported fewer symptoms of anxiety than athletes in lower competitive ranks,42 62 63 for instance, first-league compared with second-league soccer and basketball players.42 62 Similarly, basketball and soccer players with more years of playing experience exhibited lower anxiety scores than athletes with less experience.42 62 Lastly, trait anxiety scores were lower in high-ranked compared with low-ranked professional golfers,64 although not in high-ranked and low-ranked baseball players.65
Motivation and coping
Two studies measuring team-sport athletes (eg, football, hurling) reported a negative correlation between trait anxiety and several measures of motivation, including autonomy, integrated regulation (behaviours congruent with one’s value system) and intrinsic motivation (actions that produce satisfaction from participation).39 66 Trait anxiety was also positively correlated with non-regulated motivation (lack of intention to perform an action).66 Combined team and individual sport athletes with panic disorder were less likely to use social support coping, positive reinterpretation (reappraising an adverse situation in an optimistic way) and information seeking compared with athletes without that diagnosis.67 Athletes with GAD also reported low social support coping and information seeking, while athletes with specific phobias indicated high self-blame, helplessness and emotion-focused coping (eg, regulating distress with relaxation techniques).67
Neurological and biological factors
Tension/anxiety, exemplified by uneasiness and nervousness,68 was negatively correlated with frontal alpha-asymmetries detected on electroencephalography (EEG) in soccer and American football players with concussion history who had returned to play.69 Tension/anxiety was also higher in team-sport athletes with an l/l genotype compared with an s/s genotype for the 5-HTTLPR serotonin transporter.70 Symptoms of generalised anxiety were negatively correlated with several markers of omega-3 polyunsaturated fatty acids, including blood levels of eicosapentaenoic acid, docosapentaenoic acid and HS-omega-3 indices, in athletes across a range of sports (basketball, soccer, rifle, and golf).71
Performance
Trait anxiety was negatively associated with performance in two studies, one regarding race times for long-distance runners72 and the other regarding performance errors following a competitive motor task in collegiate athletes.73 For state anxiety, accurate performance feedback from an experimenter was associated with lower anxiety shortly after a competitive task, whereas low feedback was associated with a short-term increase in state anxiety for rowing and cross-country athletes.74 Similarly, ‘optimal’ state anxiety (dependent on an athlete’s recollection) was associated with high performance in track and field athletes.75
Sport type
Comparisons across sport types were rarely reported in the included literature. One study found that aesthetic sport athletes (eg, gymnastics, figure skating) had the highest rates of GAD, while risk sports (eg, aerial sports, motor sports) had the lowest rates in both male and female athletes.3 One study found handball players had higher state and trait anxiety compared with volleyball players.30 Lastly, no differences in state and trait anxiety were found between team-sport and individual-sport athletes.76
Quality appraisal (risk of bias)
For full quality appraisal, see online supplementary files 4–9e. The overall appraisal score (as a proportion) for all studies was 0.8. Articles were typically of high quality, with 41 articles (67%) scoring 0.8 and above. Nineteen articles (31%) were of moderate methodological quality (0.5–0.79), and one article (2%) was of poor methodological quality (<0.5). No studies were excluded based on these analyses.
Supplemental material
Discussion
The present study sought to identify determinants of anxiety symptoms and disorders among elite athletes, in addition to summarising the extant literature on this population to date. As noted by others,77 findings of this review highlight a rapid increase in this research domain, with 75% (n=46) of included studies published within the last 5 years. The meta-analysis outcomes indicated several general factors as being salient to symptomatic anxiety in elite athletes, including female gender, younger age and recent experience of adverse life events. These factors are consistent with findings from a recent meta-analysis for competitive anxiety in athletes,14 and trends in the general population.14 78 79 Meta-analysis also indicated the role of two athlete-specific factors, namely current musculoskeletal injury and sporting career dissatisfaction, as being associated with anxiety symptoms. This is the first meta-analysis to highlight these domains as potential risk factors for symptomatic anxiety among elite athletes.
Considering the athlete-specific factors, musculoskeletal injury and career dissatisfaction can be understood as prominently biopsychosocial influencers of mental health.80 Attention to these factors, when present for elite athletes, may assist sports medicine practitioners in planning for the psychological management needs of athlete cohorts. While individual intervention may be required for affected athletes (eg, psychotherapy, pharmacotherapy), sport administrators and officials may also wish to consider the broader environmental factors that may contribute to athlete injury or career dissatisfaction. For example, systemic approaches may involve challenging once normative attitudes about the need for athletes to play or train though pain or injury in order to demonstrate resilience or ‘toughness’.81
Additionally, retirement status as an athlete-specific subgroup analysis indicated that experiencing recent adverse life events was associated with higher global anxiety/depression in former but not current athletes. Established support services for athletes that have transitioned out of elite sport should consider the presence and impact of recent adverse life events in this population as a potential risk factor of symptomatic anxiety.
Meta-analysis of the five studies that also reported data from a non-athlete control group29–33 indicated that athletes report anxiety symptoms at comparable severity with the general population. Similarly, a recent meta-analysis identified that high-performance athletes were no more likely than non-athletes to report mild to severe symptoms of depression.82 This is consistent with assertions that elite athletes are not necessarily protected from mental health symptoms by virtue of their sporting role,83 strengthening the rationale for an increased focus on the mental health of this population, and the broader development of the field of sports mental health.84 85 Anxiety disorders (especially GAD and social anxiety) are relatively prevalent in the general population, and may be similarly so in elite athletes, although research into diagnosed disorders (relative to symptoms) in this population is lacking.
This study also examined a range of broader outcomes that were not suitable for inclusion in the meta-analysis. Unsurprisingly, it was found that anxiety symptoms in elite athletes were associated with symptoms of depression,40 46 or a depression diagnosis,42 in addition to other concurrent anxiety disorder diagnoses.3 Anxiety symptoms were lower among more experienced athletes,42 62 63 and may have a negative relationship with both motivation39 66 and discrete aspects of sporting performance.72 73 These findings further support the role of preventative or early intervention approaches in the management of anxiety disorders in elite athletes, as this may lower the likelihood of developing comorbid mental health problems (such as depression), and increase the likelihood of motivation and performance remaining intact. Psychological factors considered essential for elite athletes successful at the highest levels include affect and self-regulation, maintaining motivation, self-confidence and adaptive coping strategies, alongside supportive interpersonal relationships.86 Development of and attention to such factors will almost certainly assist athletes in managing anxiety (either at the symptom or diagnostic level), and coupled with evidence-based intervention (eg, cognitive behavioural therapy), should be considered by sports medicine practitioners and sports officials in supporting the mental health of athlete populations.
The overall mean age for participants in the included studies was 24.5 years, which is inclusive of several studies that incorporated recently retired athletes. For most Olympic and professional sports, the years of competitive elite competition directly overlap with the peak ages of onset for mental disorders, with 75% of all mental disorders shown to emerge prior to age 25.87 As anxiety disorders account for a large proportion of the burden of disease among all mental health problems,88 their presence among and impacts on elite athlete populations affords greater attention and action where needed. Younger populations are also known to experience particular barriers to accessing mental healthcare,89 and elite athletes have additional role-related barriers including concerns about stigma and the impact of disclosure and help-seeking on team selection.90 The development of youth-specific models of mental healthcare for those under 25 years has resulted in decreased stigma and service barriers, improving access to evidence-based intervention.91 Athlete-specific models of care are emerging,92 and efforts to consolidate and expand such initiatives warrant the support of governing bodies, codes, and competitions.
Limitations and future directions
We acknowledge several limitations. In general, the quality of study reporting was relatively high, suggesting an overall low risk of bias in the included studies. Nonetheless, a wide range of anxiety symptom rating scales were employed in the studies included in the meta-analysis. Where possible, we conducted subgroup analyses for measures differentiating trait, generalised, global and diagnosed anxiety. Heterogeneity was initially observed for the gender, concussion and career dissatisfaction analyses, though resolved after inspection of sample-specific differences (eg, differences between sports). Additionally, only a small proportion of the included studies reported a confirmed clinician-rated or interviewer-rated diagnosis of anxiety, with most studies employing self-reported symptoms. Distinguishing anxiety symptoms from diagnostic disorders is important given functional impairment and associated distress is likely to be more severe in the latter. Studies examining outcomes of athletes within the clinical range for anxiety disorders are currently lacking, and as the field progresses, future reviews should look to examine potential group differences according to clinician or interviewer-rated diagnoses of anxiety versus self-report symptoms, given there may be bias in self-report measures, either in terms of under-reporting or over-reporting.93 Further, attention should be given to patterns of symptom onset, duration, severity and associated distress4 in order to distinguish anxiety disorders from competition-based performance anxiety.
While a relatively large number of studies were included in this review, only one study reported on the effects of an intervention, and there were only a handful of studies using a longitudinal design. The single included intervention study was a small RCT testing a mindfulness-acceptance–based approach.94 While other groups have developed athlete-specific mental health interventions (eg, the athlete optimisation approach for college athletes of Donohue et al),92 anxiety outcomes of these interventions are yet to be explored. The present results highlight the urgent need for well-conducted intervention-based RCTs, and specific attention towards the acceptability and efficacy of psychotherapy approaches among elite athletes is needed. Similarly, longitudinal studies in elite athlete populations are needed to shed light on anxiety symptom patterns according to temporal factors. Related to this, the present study was unable to conclude whether time in competitive season impacted outcomes. It is possible that a seasonal effect of athlete anxiety may exist in line with peak training loads, recovery and proximity to major competition.95
The present review discovered markedly higher symptomatic anxiety among female athletes than their male counterparts. Emerging research suggests that younger males, who can be socialised to deny or suppress perceived vulnerabilities in sport settings,96 may exhibit mental health symptoms through a constellation of behaviours beyond those included in diagnostic criteria for internalising disorders such as anxiety.97 98 Research attention to anxiety symptoms (which are known to be higher in females), in the context of broader comorbidity domains of risk-taking, problematic anger or aggression, and substance misuse (which are known to be higher in males),99 100 may be an important step in recognising athletes at risk of mental health symptoms or disorders who may otherwise go unidentified via existing anxiety rating scales or diagnostic criteria.
Further, the present study identified an under-representation of female athletes and para-athletes. The ratio of males to females was roughly double, and only one article reported data for para-athletes.32 Future research should aim to explore these samples. Additionally, some factors pertinent to mental health are yet to be examined, including athlete sexuality and ethnicity. Future studies should consider these factors given consistent findings that minority sexuality and ethnicity differently impact mental health.101 102
To date, studies are yet to conclusively determine cross-sport comparisons for anxiety disorders in elite athletes. The main exceptions to this are work by Schaal and colleagues,3 who found higher rates of GAD among elite athletes competing in aesthetic sports, and work by Levit and colleagues,76 who found no differences in anxiety symptoms between team-based and individual athletes. Comparatively, growing literature of depression in elite athletes suggests that individual-sport athletes exhibit higher depressive symptoms than team-sport athletes.3 103 Future comparisons are needed, particularly taking account of the relative contribution of general versus athlete-specific factors in this regard. Future studies using meta-regression techniques may help quantify the unique contribution of athlete-specific factors.
Any link between the presence of an anxiety disorder or anxiety symptoms and competitive performance impacts is not yet well understood. As an extension, it is unclear whether athlete-specific interventions that provide remission of anxiety symptoms may be associated with changes in performance. Furthermore, while GAD and generalised anxiety symptoms were well addressed in this review, at present we know far less about other anxiety disorders (eg, OCD, panic disorder, social phobia) and a related personality disorder (ie, obsessive-compulsive personality disorder; OCPD) in elite athletes. Ritualistic behaviours or routines are common among elite athletes,86 and potential overlap between such behaviours and anxiety disorders, especially OCD and OCPD, remains poorly understood.
Finally, additional research is needed on neurological or biological aspects of anxiety in elite athletes. There was a relative lack of attention to this among included studies, and such research could consider EEG profiles,69 or imaging approaches, the effects of biotherapeutic agents such as omega-3 polyunsaturated fatty acids71 or cannabidiol, which is currently not a prohibited substance for athletes,104 and genomics and related hereditary analytic approaches.104
Conclusions
Factors associated with anxiety symptoms among elite athletes provide useful information for preventative intervention or acute phase management. While there are research gaps related to particular subtypes of anxiety in elite populations (eg, OCD, panic disorder), this review highlights both general factors and athlete-specific factors associated with symptom burden. Though data are lacking, it seems feasible that focused and acceptable interventions for anxiety symptoms among athlete populations may enhance career longevity and improve role satisfaction. Youth-specific models of mental healthcare that have been established internationally are likely to be useful for those aiming to develop innovative athlete-specific services. While it remains to be seen whether such approaches will improve sporting or athletic performance, the next decade is certain to see major investment into the mental health of athletes and expansion of sports mental health as a discipline.
Acknowledgments
The authors thank the other participants in the 2018 International Olympic Committee Consensus Meeting on Mental Health in Elite Athletes, including Cindy Miller Aron, Antonia Baum, Abhinav Bindra, Richard Budgett, Niccolo Campriani, Joao Mauricio Castaldelli-Maia, Alan Currie, Jeff Derevensky, Lars Engebretsen, Ira Glick, Michael Grandner, Doug Hyun Han, David McDuff, Margo Mountjoy, Aslihan Polat, Margot Putukian, Allen Sills, Torbjorn Soligard, Todd Stull, Leslie Swartz and Li Jing Zhu, for their input on the development and interpretation of this research.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 43.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
Footnotes
Contributors All authors conceived the study. MEH conducted the search, and SMR, RP and KG screened the articles. KG abstracted the data and performed the statistical analysis. SMR and OS-E reviewed the data for consistency. SMR and KG drafted the manuscript. All authors critically reviewed the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.