Article Text

Abstract
Background The mechanisms of ACL injury in rugby are not well defined.
Aim To describe the mechanisms of ACL injury in male professional rugby players using systematic video analysis.
Methods 36 cases from games played in top professional leagues and international matches were analysed. 5 analysts independently assessed all videos to record the estimated frame/time of initial ground contact, frame/time of ACL tear and a range of play specific variables. This included contact versus non-contact ACL injuries, injury timing, joint flexion angles and foot contact with the ground. 37 side-stepping manoeuvres from a control game were analysed to allow comparison of non-injury versus injury situations.
Results 57% of ACL injuries occurred in a contact manner. 2 main scenarios were identified: (1) offensive running and (2) being tackled, indicating that the ball carrier might be at higher risk of ACL injury. The majority of non-contact ACL injuries resulted from a side-stepping manoeuvre. In most non-contact cases, initial ground contact was through heel strike. Statistical assessment of heel strike at initial ground contact versus non-heel strike cases showed a significant difference in injury versus non-injury outcomes, with heel strike associated with higher injury risk. Non-contact ACL injuries had lower median knee flexion angles and a more dorsiflexed ankle when compared with a control group (10° vs 20°, p≤0.001 and 10° vs 0°, p=0.033 respectively).
Conclusions Over half of ACL injuries in rugby in our analysis resulted from a contact mechanism. For non-contact injuries, lower knee flexion angles and heel-first ground contact in a side-stepping manoeuvre were associated with ACL injury.
- ACL
- Rugby
- Anterior cruciate ligament
- Knee injuries
- Contact sports
Statistics from Altmetric.com
Introduction
Rugby union (hereafter referred to as rugby) turned professional in 1995. As the rate of injury has increased since this time, it is important to understand the mechanism of injury with a view to reducing injury risk.1–5 Knee injuries result in the most days absent from playing in professional rugby.6 ACL injuries account for 29% of days missed due to knee injuries, on average 271 days absence per ACL rupture.6
Understanding injury mechanisms is an integral step in injury prevention research.7 ,8 Initial factors to assess are playing situation (skill performed before and at point of injury, as well as player and pitch position) and athlete behaviour. These can be followed by detailed investigation of the joint biomechanics and loading patterns that lead to injury.7 Little is reported about the mechanisms of ACL injuries in rugby.
Mathematical modelling, laboratory motion analysis and cadaveric studies have helped in understanding the possible mechanisms of ACL injury.9–11 However, these studies are limited by their challenges in assessing real injury scenarios and therefore sport-specific injury mechanisms. Retrospective interviews are limited by the athlete or coach's ability to comprehend, recall and articulate what occured.12 In contrast video analysis allows researchers to study playing situations preceding and during injury, as well as comparisons between injury and control groups. Several video analysis studies of ACL rupture in football,13 ,14 handball,15 basketball,16 Australian football,17 alpine skiing,18 and netball19 have been reported. Therefore, we aimed to use retrospective video analysis to describe ACL injury mechanisms in rugby. The focus was on comparing contact versus non-contact injuries, the timing of the injury, joint flexion angles and the nature of foot contact with the ground. In addition the most common non-contact injury scenario was compared with similar non-injury events in an effort to identify contrasting biomechanics and possible variations in the playing situation and player behaviour. We hypothesised that ACL injuries in rugby would occur predominantly in a non-contact manner through side-stepping and landing mechanisms similar to what has been previously reported for other team sports.
Materials and methods
A semiquantitative observational cohort study design was used to identify phase-of-play specific variables relating to ACL injuries in men's professional rugby using video evidence. No personal player information was accessed and therefore ethical permission was not required.
Data collection
A database of ACL injuries from rugby games from 1 January 2014 to 31 December 2015 was compiled using Google News. Tournament-specific searches (eg, ‘ACL injury Six Nations’) and club-specific searches (eg, ‘ACL injury Ulster Rugby’) were applied (see online supplementary appendix 1 for a list of all teams and tournaments searched). Fifty-four ACL injuries were identified in training, preseason and competitive matches (figure 1). Only competitive matches were included for analysis.
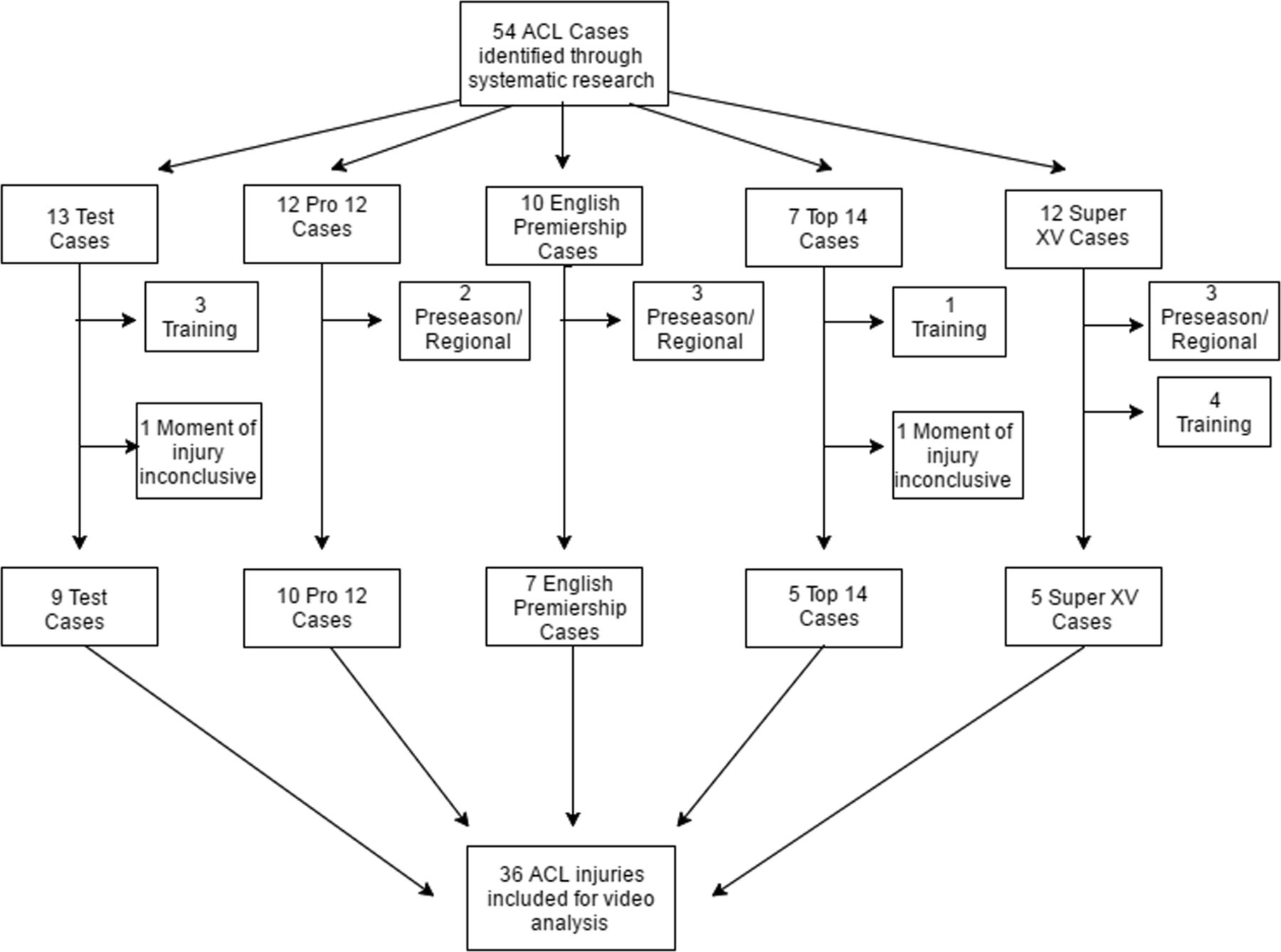
Flow chart indicating the 54 ACL ruptures identified and the screening process to make up the 36 cases of competitive match injuries used for video analysis.
supplementary appendix
Of the 54 injury cases identified, video footage for 36 competitive match injuries were obtained for analysis using (Optapro Rugby, London, UK) (figure 1). No medical information was available, apart from media reports of an injury. Fourteen cases were available with three camera views, 8 cases had two camera views, and 14 cases had one camera view; where possible, composite videos were created by manual synchronisation using visual clues (eg, initial foot ground contact).
Video processing
Injury sequences were cut and processed using Sportscode Elite V.9.8.3 software with all files converted to QuickTime (.mov), allowing frame-by-frame navigation using QuickTime player (V.7.7.9, Apple, Cupertino, California, USA). All videos were deinterlaced using the progressive scan feature of Elgato Turbo 0.264. Cases were cut as a sequence containing ∼10s before the injury event and 2–3s after the injury to assess the specific match situation.13 Another sequence was cut with 1–2s before injury and 1–3s after injury to analyse biomechanical variables.
Video analysis
Five analysts (an international rugby analyst with a background in bioengineering, an orthopaedics/sports medicine specialist, a chartered musculoskeletal physiotherapist, an orthopaedic surgeon and a bioengineer) independently assessed all videos in real time and frame-by-frame to record the estimated frame/time of initial contact (IC) as well as the frame/time of ACL tear, referred to as the index frame (IF).13 ,16 A meeting was held to establish a consensus for IC and IF for all cases, with consensus defined as four of the five analysts agreeing. The mean absolute deviation of the analysts individual estimates of IC and IF was 6 ms and 8 ms, respectively. All videos were categorised independently by the analysts using a form (see online supplementary appendix 2) adapted from protocols for other sports.13 ,16 ,18 ,20 This included categorical variables on injury circumstance and estimated flexion angles for the hip, knee and ankle (to the nearest 10°) for both IC and IF for all non-contact injury cases.
supplementary appendix
A non-contact injury was defined as occurring with no bodily contact with another player in the IF (figure 2). Contact to any body part other than the injured leg was defined as indirect contact, while contact to the injured leg was defined as direct contact.14 ,15 ,17

Scenario B, non-contact offensive running: a side-stepping manoeuvre leading to ACL injury. (A) Initial contact: player makes contact with the ground with his heel while performing a side-stepping manoeuvre. (B) Index frame: knee valgus is apparent as player attempts to complete manoeuvre.
Player velocities in the vertical and horizontal directions were categorised as high, low, zero or unsure. Low horizontal speeds refer to walking and jogging while high refer to running/sprinting. Low vertical speeds refer to running, stopping and cutting, while high refer to a distinct jump.
Knee valgus of the injured leg at either IC or the IF was recorded where possible. One case was excluded from joint flexion angle analysis due to inconclusive camera angles and in one case it was not possible to distinguish between a non-contact injury and a contact injury.
The categorical variables were established by consensus. The analysts also performed visual inspection of joint flexion angles in line with previous video analysis protocols.13 ,16 ,17 No measurement tools were used to aid the visual inspection estimates of the experts.16 The median joint flexion angles estimated by the five analysts were recorded along with the IQR.
Control group for non-contact injuries
The most common non-contact Injury was due to a side-stepping motion. To study these in more detail, we identified a control group where the player side-stepped but did not sustain an ACL injury. A randomly chosen game in the Rugby World Cup 2015 (including a Northern and a Southern hemisphere team) was used to assess every sequence in which a ball carrier performed a side-stepping manoeuvre: 51 cases were identified, 14 of which were excluded due to inconclusive camera angles to assess joint flexion. The joint flexion angles of the remaining 37 cases at IC were estimated as previously described. These cases were then statistically compared with the side-stepping injury cases.
Statistical analysis
All statistics were calculated using SPSS (IBM SPSS Statistics for Windows, V.22.0. Armonk, New York: IBM Corp.). Knee and hip flexion angles were reported as positive numbers, ankle flexion angles were reported as negative numbers for plantar flexion and positive for dorsiflexion. Normality of data was assessed using the Shapiro-Wilk test and results for not normally distributed data were reported as median and IQR. The Mann-Whitney U test was performed on the hip, knee and ankle angles of the non-contact side-stepping injury cases compared with the control cases. Statistical significance was set at the 0.05 level. Fisher's exact test was used to assess the association between heel strike or non-heel strike during side-stepping injury versus non-injury outcome. Statistical significance was set at the 0.05 level and the effect size was measured using Phi and Cramer's V with a score of >0.5 regarded as a large effect size.21 Inter-rater reliability for joint flexion angle estimations was assessed using the intraclass correlation coefficient (ICC). An ICC of >0.75 was regarded as excellent.22
Results
The injury rate was 0.43 ACL injuries per 1000 player hours under match conditions. Of the 36 cases for which analysis was possible, 35 could be categorised into contact and non-contact cases: 15 (43%) were non-contact and 20 (57%) were contact cases. Contact cases were further subdivided into 8 (23%) indirect contact and 10 (29%) direct contact cases; 2 cases were contact injuries but could not be subdivided into direct/indirect contact. The majority of ACL injuries occurred in an offensive playing situation (63%, n=22). Injuries were spread evenly over the pitch locations, with 13 occurring in the offensive third, 11 in the defensive third and 12 in the middle third. Three matches (8%) had precipitation at the time of injury occurrence. There were 21 right knee injuries and 15 left knee injuries. Centres and hookers sustained the highest number of ACL injuries (figure 3).
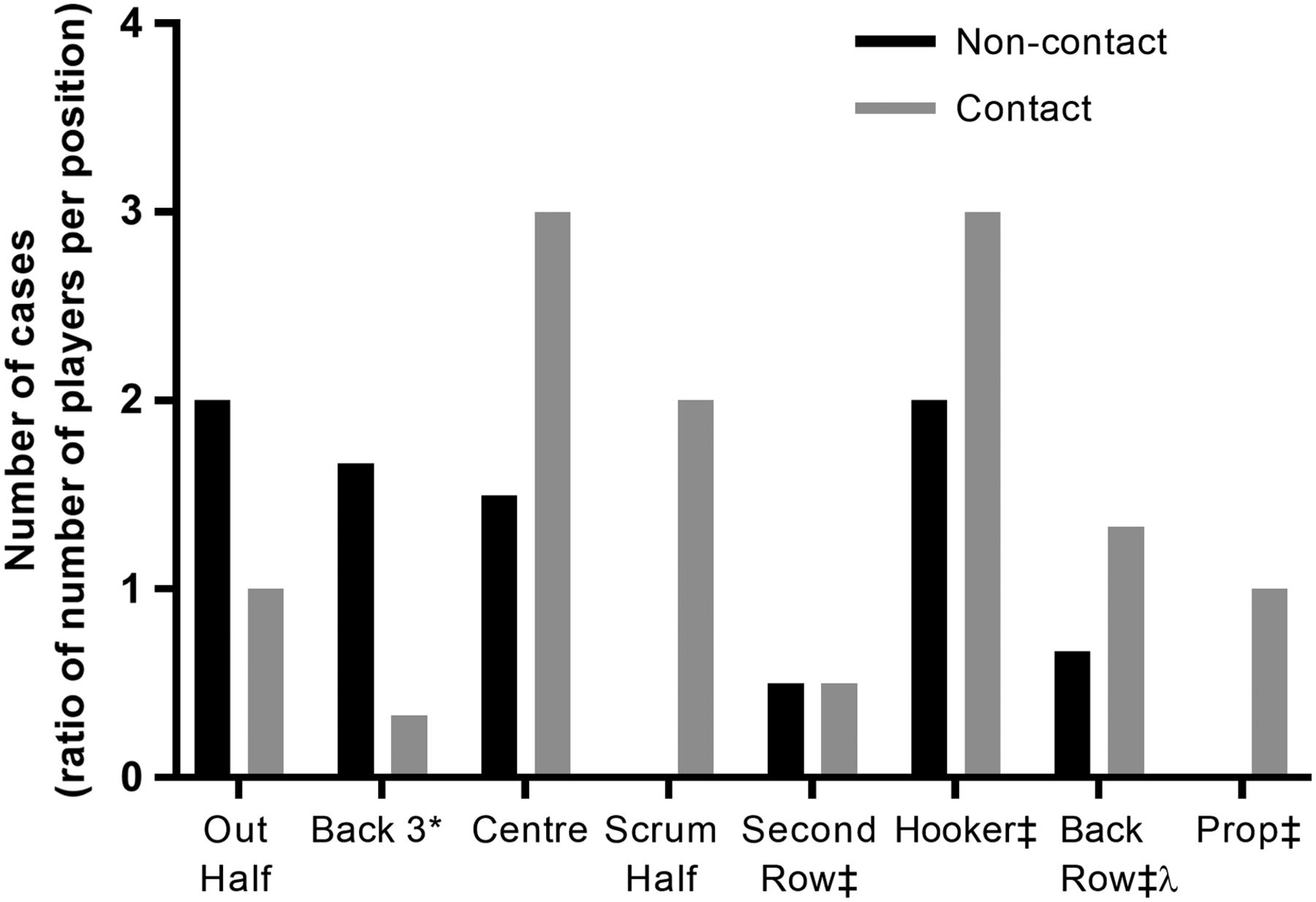
Break down of ACL injury by position (all positions of multiple players were calculated as a ratio of one player per position for comparative purposes). ‡denotes forwards, *back 3 includes: full back and 2 wings, λback row includes: number 8 and 2 flankers.
Playing situations for non-contact and contact injury cases
The contact injuries occurred during: rucking (n=4), tackling (n=5), being tackled (n=9), set play (n=1) and kicking (n=1). The non-contact injuries occurred during: offensive running (n=11), defensive running (n=3) and set play (n=1) (tables 1 ⇓–3).
Rugby-specific variables recorded for 36 ACL injury cases analysed using systematic video analysis
Biomechanical variables recorded for 15 non-contact ACL injury cases analysed using systematic video analysis
Biomechanical variables recorded for 20 contact ACL injury cases analysed using systematic video analysis
Contact injury mechanisms
The most common mechanism of contact ACL injury was being tackled (scenario A; see online supplementary video 1). The injured player was always in possession of the ball. A combination of both high (n=6) and low (n=3) speeds were observed. In six cases the player was moving forwards or in a combination of forward and sideways at the time of contact. Contact was evenly distributed between direct (n=5) and indirect contact (n=4) (n=1 unsure). Rucking cases occurred predominantly to defensive players who were either stationary or moving at low speed (n=3). Tackling contact injuries occurred at both high (n=2) and low (n=3) speeds.
supplementary video
Non-contact injury mechanisms
Ten non-contact ACL injuries occurred while a player performed a side-stepping (evasive) manoeuvre. The remaining injuries were sustained when landing, crossover cutting, stopping, passing, or running without possession. Foot contact at IC was heel strike in 10 of the 15 non-contact cases, with 9 of the 10 side-stepping cases having heel strike at IC. Eight of the 10 heel strike cases occurred in the second half of the game and five occurred in the last quarter (figure 4). Eleven non-contact injuries occurred to a knee that appeared to be fully load-bearing.

Non-contact ACL injuries in relation to when they occur and the category of foot strike at initial contact.
The most frequent non-contact injury situation was offensive running, (scenario B, figure 2 and see online supplementary video 2). In 9 of the 11 cases, the attacking player was the ball carrier and in 8 of the 11 cases the player was performing a side-stepping manoeuvre. The foot plant at IC was heel strike in eight of offensive running cases, flat in two cases and toe strike in one case. The flexion angles at IC all were ≤40° for the hip (n=9) and ≤20° for the knee.
supplementary video
Control study
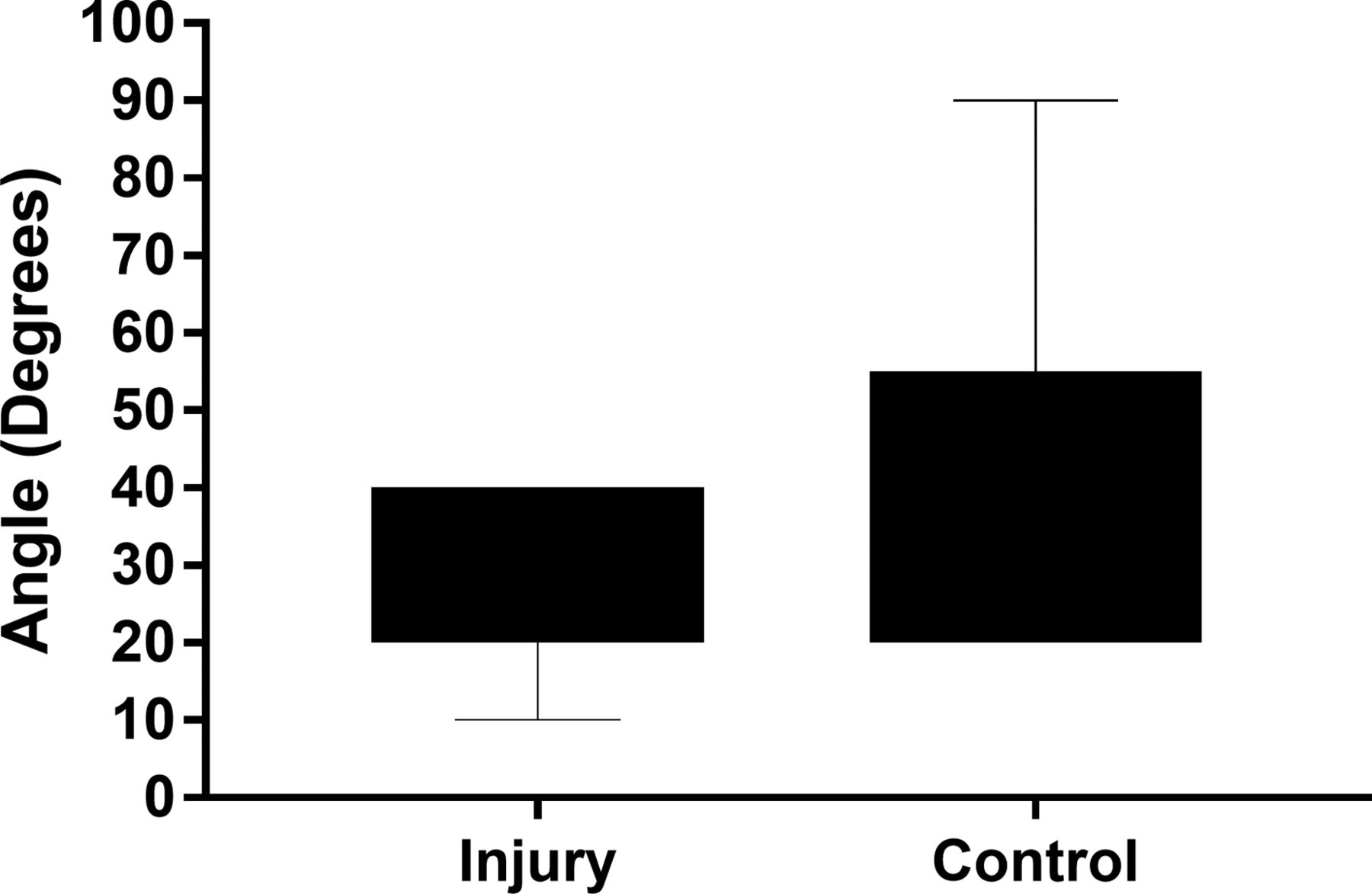
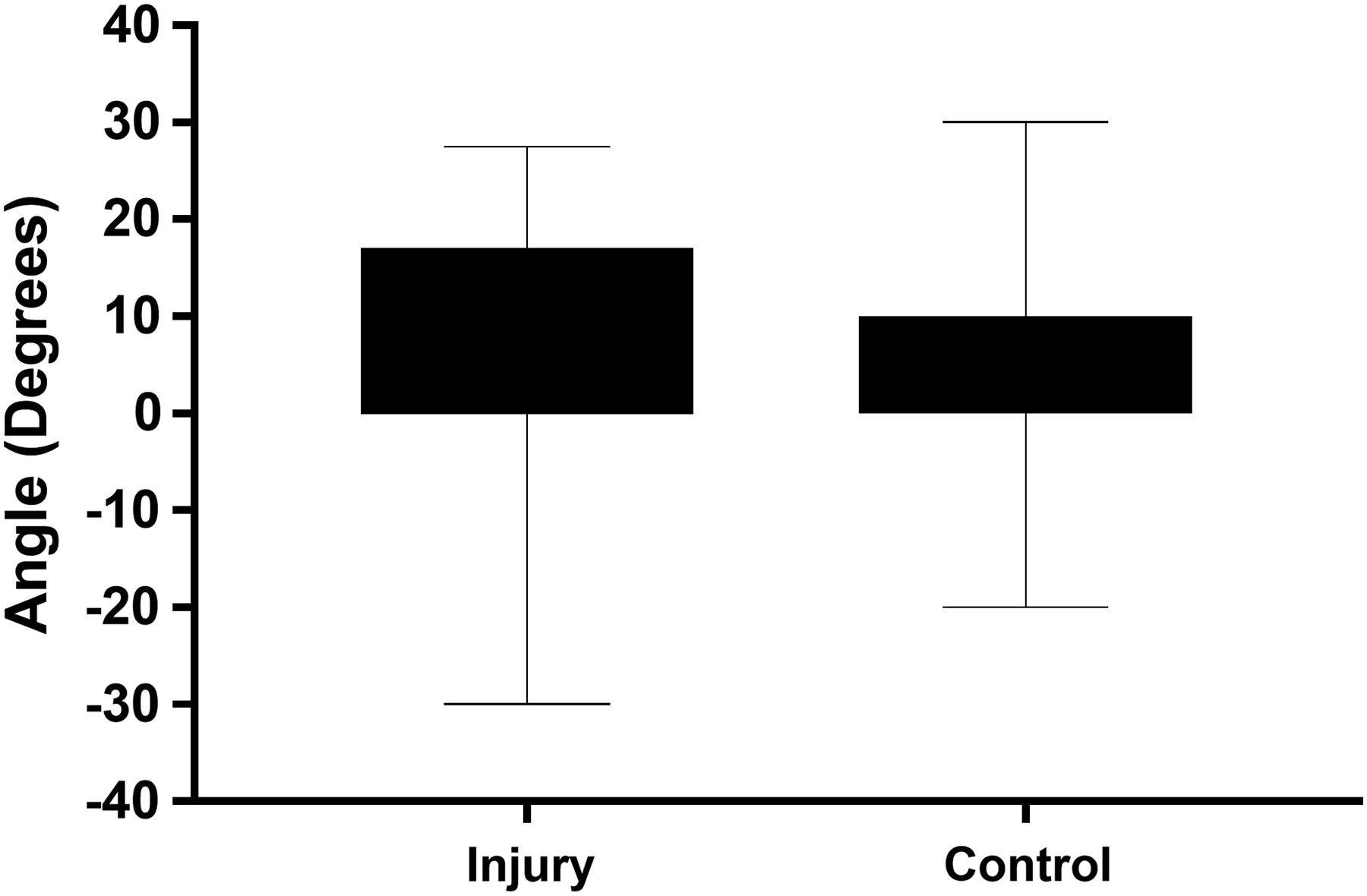
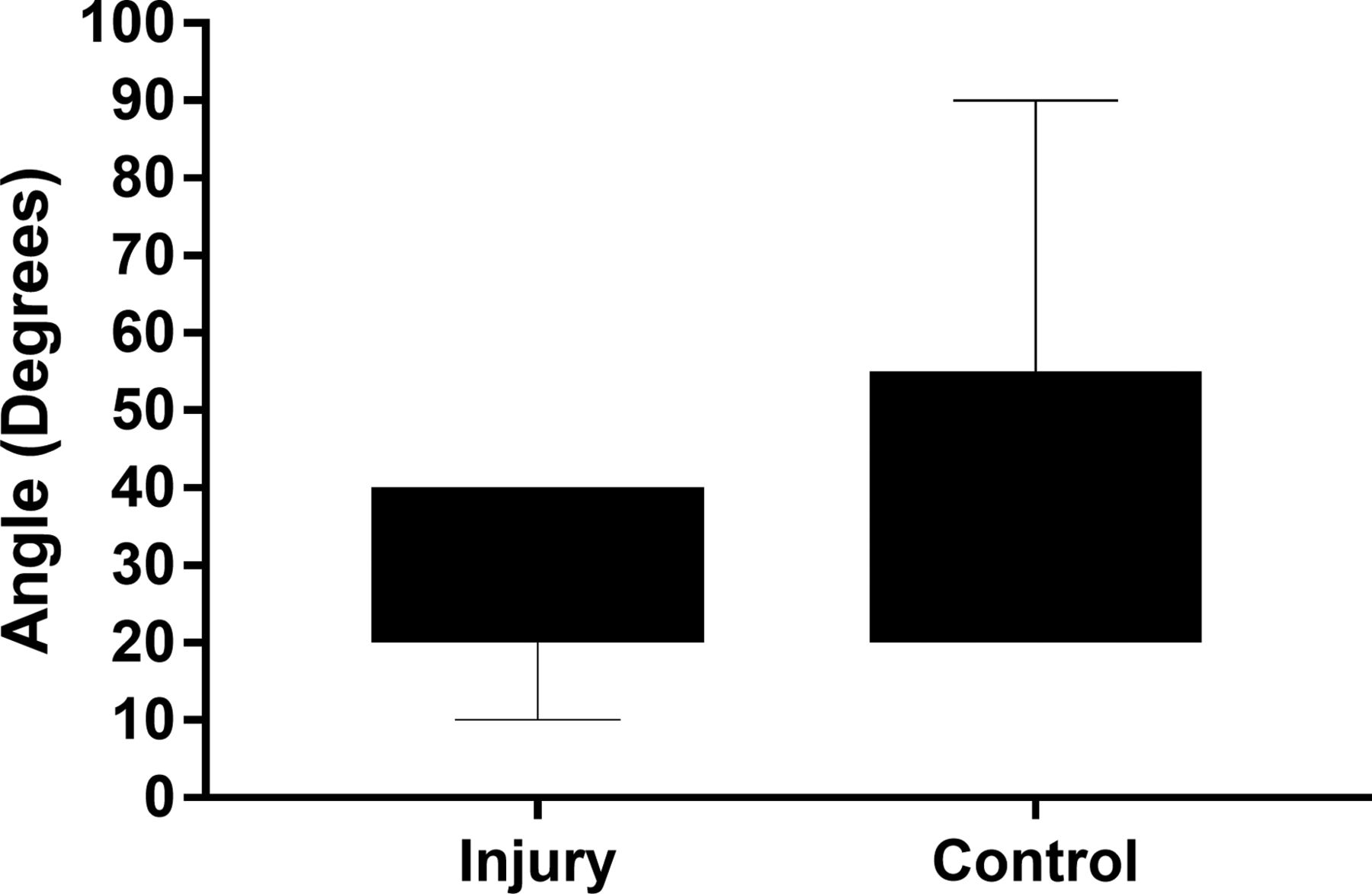
From the 37 cases of side-stepping manoeuvres involving no ACL injury only 8 had a heel strike at IC, while the remaining 29 were flat or toe strike. All heel strike cases occurred in the second half. Hip, knee and ankle angles data at IC were not normally distributed. The flexion angles for the control cases were compared with the side-stepping injury cases (see online supplementary tables 1 and 2). The median hip flexion was 30° for injury cases versus 30° in non-injury cases (figure 5). The median knee flexion angle was 10° for injury cases versus 20° in non-injury cases (figure 6). The median ankle flexion ankle was 10° for injury cases versus 0° in non-injury cases (figure 7). The differences in knee and ankle flexion angles for the injury and non-injury cases were statistically significant (p≤0.001 and p=0.033, respectively); the hip flexion angle differences were not statistically significant (p=0.26). Inter-rater reliability for joint flexion angles across the five analysts was ICC=0.97, ICC=0.96 and ICC=0.93 for the hip, knee and ankle angles, respectively. There was statistical significance seen for heel strike versus non-heel strike at IC when comparing injury to non-injury p≤0.001 (table 4) with a large effect size (Phi and Cramer's V=0.582).21
Foot strike at initial contact for side-stepping injury and non-injury cases statistically compared using fisher exact test and Phi and Cramer's V
Box plot of hip flexion angles: injury cases versus non-injury cases.

Box plot of knee flexion angles: injury versus non-injury cases.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plot of ankle flexion angles: injury versus non-injury cases.
supplementary tables
Discussion
This is the first reported video analysis of the injury mechanism of ACL injuries in men's professional rugby. The ACL injuries evaluated were from the available videos obtained from leading international and club teams over a 2-year period (2014–2015). We identified two main scenarios: being tackled (scenario A)—a contact injury mechanism, and offensive running (scenario B)—a non-contact injury mechanism. These scenarios accounted for 56% of all ACL injuries. Fifty-seven per cent of ACL injuries occurred as a result of contact mechanism in rugby and a valgus force was present in 80% of these contact injuries. Side-stepping was the mechanism of injury in 67% of non-contact injuries.
Contact versus non-contact ACL injuries
The proportion of contact ACL injuries in rugby is substantial (57%, n=20/35). Rugby is a full contact sport which might explain the increased proportions of contact injuries compared with football and basketball (36% and 28%, respectively).13 ,16 In rugby, there were similar rates of direct contact injuries compared with Australian football (29% vs 32%) and higher than in football (15%), handball (5%) and basketball (10%).13 ,15–17 Rucking and scrummaging are unique to rugby and these actions accounted for 25% (n=5) of contact cases.
Playing situations associated with contact ACL injury
The unpredictable nature of contact situations may contribute to the lack of clearly defined injury patterns. For example contact cases were evenly distributed between defensive (n=8) and offensive situations (n=11), with the remaining case occurring during set play. Contact injuries were in combination with valgus loading at the knee (80%, n=16). A valgus force was present in 7/10 direct Contact injuries, and these results show a similar trend to football where 5/6 direct contact injuries occurred under a valgus force.13 Further research with a larger sample size may help elucidate any of the contact categories result in a significant increase in ACL risk.
Playing situations associated with non-contact ACL injury
Side-stepping injuries accounted for 36% (n=13) of cases overall, and for 67% (n=10) of all non-contact ACL injuries. This is higher than in Australian football, where 37% of non-contact ACL injuries resulted from side-stepping.17 This may be because Australian football has higher incidences of injuries resulting from players competing for a high ball, an integral part of Australian football but much less common in rugby. Illustrating this landing accounted for only one case in our study.
Sixty-one per cent (n=22) of all ACL injury cases occurred during offensive situations and these accounted for 73% (n=11) of the non-contact cases. The opposite was found in football.13 ,14 This is most likely because in rugby, the ball carrier performs evasive manoeuvres to avoid contact.
Knee and ankle flexion and foot strike
The median knee flexion angle for non-contact injury cases (10°, range 10–20°) was statistically lower than for non-injury cases (20°, range 10–60°). The median difference is small, but the injury cases have a small spread around the median, whereas the non-injury cases have a much larger spread. This suggests that these injuries might be more likely to happen at a lower knee flexion angle. These findings are similar to previous studies of Australian football and football where all injury cases in both studies were found to occur ≤30°,13 ,17 while a detailed study estimating joint kinematics in ACL injury in basketball and handball reported a median knee flexion angle of 23°.23 Three dimensional joint angle analysis should be applied to ACL rugby injuries in future. Since anterior shear force on the ACL at low knee flexion angles is known to be a contributing factor in ACL rupture,24–26 we anticipate that such an analysis would corroborate our results.
The median ankle flexion angle for non-contact injury cases (10°, range −10° to 10°) was statistically higher than for non-injury cases (0°, range −20° to 20°). This indicates that players who sustained ACL injury cases were more likely to have a dorsiflexed ankle at IC when compared with non-injury cases (who tended to have a neutral ankle). This corresponds with the predominance of heel strike cases we observed occurring in the injury cases versus non-injury cases. In cases with flat or heel strike landings, the calf musculature may be unable to absorb the ground-reaction forces adequately, which are then transmitted directly to the knee.27 Therefore landing on the forefoot may be crucial to preventing ACL injury.9 The high proportion of heel strike cases seen in non-contact ACL injuries in rugby may be an important aspect to target when creating rugby-specific ACL injury prevention programmes. A sidestep cut with toe planting decreased knee abduction moments, and an improvement in side-stepping technique reduced ACL risk.28 Therefore, interventions that target the side-stepping technique may have merit in rugby injury prevention programmes.
Fatigue
In our study, 47% of non-contact injuries (n=7) and 42% (n=15) of all injuries occurred during the last 20 min of the match. This was similar to a previous study where 29% of all ACL injuries occurred in the last quarter of a match.6 Eighty-nine per cent (n=16) of heel strike cases for both injury cases and controls occurred in the second half of the match. We hypothesise that fatigue plays an important role in determining the nature of foot strike, which may subsequently predispose the player to ACL rupture. Although important, limitations to note are that substitutions and preceding training load and match congestion for the injured players were not assessed in our study. Fatigue significantly increases tibial anterior shear force and decreases knee flexion angles when performing stop-jump tasks.29 Therefore, changes in lower limb control as a result of fatigue may increase the risk of non-contact ACL injuries during landing.30
Limitations
Our analysis is based on 36 cases, but these are all of the ACL injuries identified in the major league rugby tournaments over a 2-year period for which analysis was possible. This is a similar sample size to equivalent studies in other sports.13 ,15–18 The cases were evenly distributed among all of the leagues and test matches, with at least seven cases in each competition. We also observed an almost identical injury rate to that reported in a two-season study of English professional rugby union performed in 2002/2003 (0.43 vs 0.42 per 1000 player hours). Therefore, our results should be representative.6 In addition we used the same methodology used by most other systematic video analysis studies on ACL injury mechanisms in other sports.13 ,16 ,17 The cases only included injuries that occurred in men's competitive games—it is unknown whether training injuries and injuries sustained by amateur and women players occur as a result of the same mechanisms or playing situations.
The database was collected by a structured search of worldwide media, and it was not possible to confirm independently that ACL rupture occurred, or the extent of associated injuries or the history of previous injuries. However, there is no reason to suspect any selection bias in the reported results, and we expect that media reports of ACL injuries are generally reliable due to the long injury absences involved.
Video analysis studies are dependent on the quality and resolution of the images and the number of camera angles available. The exact moment when the ACL tear occurred could not be accurately determined, so the time point identified as the IF is an estimate based on the subjective observations of the five experienced analysts. A high degree of agreement was seen in their initial IF and IC estimations. We excluded 1 injury case and 13 control group cases from flexion analysis due to poor video quality or inconclusive camera angles. The remaining 14 injury cases and 37 non-injury cases had a varying number of camera angles. The accuracy and precision of video assessment of joint angles may be limited.31 However, we had an excellent inter-rater reliability (all ICC values >0.9268) for joint flexion angle estimations for both injury and control cases. This allowed for identification of trends rather than attempting to identify a precise flexion angle associated with injury. Future studies would benefit from using model-based image-matching techniques when analysing joint flexion angles,32 ,33 although this is a time-consuming process and requires multiple camera angles.
Conclusions
Two scenarios in rugby accounted for 56% of all ACL injuries: (1) a player being tackled and, (2) offensive running. Over half of the ACL injuries had a contact mechanism. Most non-contact ACL injuries resulted from a side-stepping manoeuvre by a ball carrier. In most of these non-contact cases, initial foot contact with the ground was through a heel strike. Heel strike versus non-heel strike cases showed a significant difference in injury versus non-injury outcomes, with heel strike associated with higher injury risk. Furthermore, non-contact ACL injuries occurred with lower knee flexion angles compared with the control group.
What are the findings?
Offensive running and being tackled accounted for the majority of ACL injuries indicating that the ball carrier might be at most risk of ACL injury in professional rugby union.
A large number of ACL injuries in rugby had a contact mechanism.
Heel strike during side stepping was significantly associated with non-contact ACL injuries in rugby.
How might it impact on clinical practice in the future?
Our systematic video analysis of ACL injuries in male professional rugby players suggests that injury prevention programmes should target the following areas:
Change of direction technique particularly in side-stepping manoeuvres with a focus on increasing knee flexion at initial contact.
Footwork training with a focus on avoiding heel strike.
Acknowledgments
The authors would like to thank Dr Mathew Lyons for advice with the statistical analysis and Mr Paul Ryan for acting as a collaborator and one of the analysts for this research.
References
Footnotes
Contributors All authors were involved in the research concept and design, as well as data analysis and paper writing. CM, JB, GT and DW also performed the analysis.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data from our research has been discussed at least in part in the manuscript.