Article Text

Abstract
Background/objectives Walking has well-established positive relationships with, and effects on, physical health. In contrast, while poor mental health contributes substantially to global health burden, an overview of the benefits from walking has not previously been published. We aimed to scope the literature and present what is known, and highlight what is not known, about walking and mental health.
Methods Design: Scoping review.
Data sources: Ovid (Medline), ProQuest, Web of Science.
Screening and reporting: 13 014 records were identified and screened by a team of researchers. Included full texts were analysed and reported according to mental health outcome.
Results For the 8 mental health outcomes (identified a priori), there were a total of 5 systematic reviews and 50 individual papers included. Depression had the most evidence and existing systematic reviews were reported. Evidence for anxiety, psychological stress, psychological well-being, subjective well-being and social isolation and loneliness varied in volume and effectiveness, but no harmful effects were identified. There were no studies for walking and resilience. The setting and context of walking seems to be important variables.
Conclusion The evidence base that suggests walking benefits mental health is growing, but remains fragmented and incomplete for some important outcomes. Policy and national guidelines should promote the known mental health benefits of increased walking and future research should directly address the gaps we have identified.
- walking
- physical activity
- psychology
- mental
- health
Statistics from Altmetric.com
Introduction
Regular walking is known to confer many physical health benefits including better physical fitness, reduction in disease risk and reduced risk of disease specific and all-cause mortality.1 2 In addition to physical health, mental health also contributes substantially to global health burden3 and there is well-established evidence for the link between physical activity and several mental health outcomes.4 This includes variable levels of evidence for depression, anxiety, psychological distress, well-being, cognitive function, dementia, sleep, self-esteem, chronic fatigue and psychological events.4
While the link between physical activity and mental health is well established,5 6 substantially less is known about the role of walking in this respect.1 Morris and Hardman identified this gap in their seminal ‘Walking to Health’ paper in 1997 and stated that ‘The pleasurable and therapeutic, psychological and social dimensions of walking, whilst evident, have been surprisingly little studied’.7 Addressing this gap in knowledge is important as walking is an accessible behaviour conducted by all ages and sexes, and as such one with great public health potential.8
Consequently, the aims of this review are to
provide an overview of what has been learnt in the intervening 20 years in regard to preventing mental ill-being, promoting mental well-being and intervention effects;
Highlight current evidence gaps and research priorities.
Methods
We adopted the established five-stage scoping review process proposed by Arksey and O’Malley.9
Stage 1.1: identify the research question
We formulated the following research question: ‘What is known about the associations and effects of walking when considering various specified mental health outcomes?’
For the purposes of this review, we adopted the following definition of walking which we have used previously: walking was taken to mean all forms of purposeful or incidental bipedal locomotion within reasonable speed ranges (ie, not running or jogging).1
Stage 1.2: identify the relevant outcomes
The review team discussed each mental health outcome identified in the 2008 Physical Activity Guidelines Advisory Committee Report for relevance, appropriateness and feasibility for this study.4 Two authors were chartered psychologists registered with the British Psychological Society and provided expert opinion in this process (NM, AN). Depression (outcome 1 (O1)), anxiety (O2) and self-esteem (O3) were retained. Psychological distress was classified under psychological stress (O4). Well-being was split into psychological well-being (PWB) (O5) and subjective well-being (SWB) (O6) due to established evidence for the differences between these eudemonic and hedonic constructs.10 11 Resilience (O7) and social isolation and loneliness (08) were added as areas of particular mental health and public health interest. The outcomes were given operational definitions as shown in table 1.
Mental health outcomes included in this review
From the original list, dementia was classified under cognitive dysfunction (including Alzheimer’s and Parkinson’s). These were considered neurological health rather than mental health3 and were not deemed within the scope of this review. Sleep, chronic fatigue and psychological events were considered important but outside the scope and feasibility of this review. Health-related quality of life (HRQoL) was discussed extensively, but ultimately excluded as it contains physical, social and mental components. Mood was also not included as it is considered a comparatively transient state that cumulatively contributes more broadly to what we have captured in subjective and psychological well-being .12
Stage 2: identifying relevant studies
Studies were included if they met the following inclusion criteria:
research articles in any geographical location or setting
published in English in peer-reviewed academic journals
specify quantitative effects of walking on the predetermined mental health outcomes
preventive effects (negative outcomes)
health promotion effects (positive outcomes)
intervention effects (all outcomes)
designs including primary research studies (cross-sectional or longitudinal designs, interventions or natural experiments with pre–post measures and a non-walking comparison), reviews, systematic reviews, scoping reviews and meta-analyses of suitable primary research studies
include any age groups or sex.
Studies were excluded based on the following exclusion criteria:
focus only on clinical groups with a specific physical or mental illness or condition that is not the illness or condition being treated with walking, that is, secondary mental health (eg, effects on depression in patients with stroke)
evidence types including guidelines, unpublished and ongoing trials, annual reports, dissertations and conference proceedings
qualitative and ethnographic designs
editorials, opinion pieces, magazine and newspaper articles, case reports, papers with no primary data.
In studies of participants aged <18 years, pedometers were not considered measures of walking exposure due to the likely large proportion of counts from other common forms of physical activity (eg, unstructured and structured play, and sporadic movement), but we did retain this as a measurement method in adults for whom pedometer counts are more likely to reflect walking.
Search strategy and databases
The strategy was designed to be as comprehensive as possible, within the constraints of time and resource.9 We used the outcomes in table 1 to define search terms that were adapted for each relevant electronic database and combined with common walking terms. Search terms and databases are shown in online supplementary table S1. Searches were conducted in October 2017.
Supplemental material
Stage 3: study selection
All identified records were uploaded to the online Covidence software (https://www.covidence.org). Duplicates were automatically removed. Titles and abstracts were reviewed by two researchers (PK, CW) with 20% cross-checked early in the process to assess agreement. Full texts were reviewed independently by two researchers (PK, section lead) with conflicts resolved by a third author.
Scoping reviews are known to be iterative in nature as the researchers become more familiar with the data.9 In this review, it became apparent that O1: depression had a more mature evidence base, characterised by many studies and a number of systematic reviews. We therefore changed our methods and criteria to include only existing reviews for this outcome.
Stage 4: charting the data
For each outcome, key information from the relevant included texts was extracted into a standard data form (modified for the depression systematic reviews). Information included author, year, location, design, sample size and characteristics, exposure or intervention characteristics, comparator or control characteristics, outcome measures and key findings.
Stage 5: collating, summarising and reporting the results
The analytic framework for collating the data was the eight mental health outcomes (see table 1). The aim was to report relevant information on the volume, nature, distribution and characteristics of published studies. We used the ‘descriptive-analytical’ method from the narrative tradition, which involves applying a common analytical framework to all the primary research reports and collecting standard information on each study.9 Narrative summaries for each outcome as well as key concepts and related research gaps were reported.
Results
In total, we identified 13 014 records from database searches. For depression we included five systematic reviews, while for resilience there were no included studies. Across the six other outcomes, there were 50 included papers (see figure 1) though some studies appeared in more than one outcome. The findings for each outcome are reported below, with further descriptive information in online supplementary table S2.
Supplemental material

Simplified study flow chart (full Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) charts available from authors on request).
Outcome 1: depression
Of the outcomes in this review, depression has the most developed evidence base. Specifically, we report five systematic reviews.13–17 There were no reviews of walking and prevention of depression, but a 2013 systematic review of physical activity and the prevention of depression included three prospective studies of walking and all found a protective effect.18–20 Further studies that distinguish whether there are differential effects for demographics such as age and gender/sex are needed.
Considering treatment, Robertson et al concluded from eight eligible randomised controlled trials (RCTs) that walking was an effective intervention for clinical depression with an effect size of −0.86.14 This can be considered a large effect and is at least comparable to effect sizes found in systematic reviews of exercise interventions for depression.21 This finding strongly supports the use of walking as a treatment for depression, and yet more needs to be known since eight studies in this review remain a relatively small evidence base when considering representation of all ages, genders and other relevant demographics.
A systematic review focused on walking group interventions concluded they were effective for reducing depression scores.15 However, these findings should be interpreted cautiously as it was not clear if depression was clinically defined and study design was not limited to RCTs. A further recent systematic review and meta-analysis looked at the effects of physical activity on postnatal depression (PND) and weight loss.16 Four of the nine included studies were walking or pram walking (with a fifth including walking) but effects on PND were no better than comparison groups.
A 2013 systematic review examined modes and settings in effective physical activity interventions to treat depression, identifying five eligible RCTs.17 The authors concluded that indoor or outdoor walking was a beneficial aerobic exercise to treat depression. They recommended at least some supervision, performed three to four times weekly at a moderate or self-selected intensity for 30–40 min over a period of at least 9 weeks.
Outcome 2: anxiety
We identified 14 studies focusing on associations between walking and anxiety.22–35 After depression this was the second biggest evidence base. Of five cross-sectional studies, four showed an association between walking and lower anxiety scores22–25 while one did not.27 Heesch et al. also found dose–response associations in prospective models.25
Four studies investigated the acute effects of walking on anxiety and found mixed effects.30–32 35 Five studies compared walking interventions to a comparison condition over time (6–12 weeks) and found favourable treatment effects.26 28 29 33 34
Overall, walking appears to be beneficial for anxiety. Despite our attempts to operationalise the meaning of ‘anxiety’ a priori this remains a broad construct, which made it difficult to draw overall conclusions. Given the magnitude of the global burden of anxiety, this may be sufficient rationale for more focused study of walking and anxiety. There is a clear need to develop more prospective epidemiology that could assess both walking and persistent symptoms of anxiety and or clinically defined anxiety disorders.
Outcome 3: self-esteem
We identified 11 studies that examined the association between walking and global self-esteem (GSE).31 36–45 There were two cross-sectional studies that examined the relationship between walking and GSE.37 38 Both reported no association. We found no prospective analyses. Two acute studies reported benefit on GSE following a single bout of walking.31 39
There were seven intervention studies that compared walking condition(s) with another condition over time (8–12 weeks) with both favourable and null effect findings.36 40–45 Walking programmes varied in length from 8 weeks to 12 months, and in frequency, duration, intensity and progression of dose. Two studies suggested significant improvement in GSE following walking compared with comparator groups. Three of the studies suggested significant improvement in GSE following walking, but this was no greater than the comparator, and two studies showed no change in GSE.
Overall, the evidence suggests that walking interventions have a positive effect on self-esteem, but observational findings were limited. While not a focus of this review, several of the included studies also incorporated other measures of self-perception (eg, physical self-worth) that contemporary theoretical perspectives of ‘self’ would suggest are more susceptible to change following walking than GSE, and particularly in acute studies.46
Outcome 4: psychological stress
We identified six studies that examined the relationship between walking and psychological stress.27 32 47–50 One cross-sectional study showed a large significant association27 and another showed a small non-significant association.27 Threes studies assessed the acute effects of walking on psychological stress32 49 50 and findings were contradictory. One 4-week-long intervention showed promising effects at intervention completion but had no effect at 12-week follow-up.48
In summary, there is emerging but limited evidence that walking is associated with lower psychological stress in observational studies, and that can be used as a potentially promising intervention to decrease psychological stress. It is however clear that available evidence is not yet sufficient for firm conclusions.
Outcome 5: psychological well-being
We identified 11 studies that examined the association between walking and PWB.27 29 51–59 There were three cross-sectional studies that examined the association between walking and PWB. The findings generally supported a positive association between PWB and walking.27 55 57 One large-scale longitudinal study showed positive findings for walking for transport.58 There were no acute studies.
Seven RCT studies compared the effects of walking interventions on PWB with another condition (typically minimal intervention) over 10–15 weeks. The findings were mixed with instances of no improvements, no between-group effects and some positive effects for walking.29 51–54 56 59 A targeted review to understand the differential effects of intervention design and/or study quality may be required.
To conclude, the evidence is limited but promising with cross-sectional studies and the one longitudinal study identifying positive relationships between walking and PWB. The findings from the intervention studies are more mixed with only two of seven studies demonstrating positive effects on PWB compared with control groups.
Outcome 6: subjective well-being
We identified 12 studies focusing on associations between walking and SWB.27 31 35 60–68 There was diversity in how SWB was described and measured in the identified papers including life satisfaction, happiness, emotional well-being and affective response. From four cross-sectional studies, three found significant associations between higher levels of walking and better SWB.27 60 61 64 Two prospective cohort studies found weak but statistically significant relationships between walking and subsequent SWB.63 65
Five studies found positive acute effects for a single bout of walking on indicators of SWB.31 35 66–68 One intervention compared walking to stretching and toning over 6 months and found equivalent improvements in ‘happiness’ and ‘life satisfaction’ in both groups.62
In summary, cross-sectional, prospective cohort and acute studies indicate an association between walking and SWB. The only long-term intervention study was inconclusive and further studies are clearly required.
Outcome 7: resilience
The relationship between physical activity and resilience is emerging,69 with associations shown in undergraduate students69 and healthy adults.70 However, we identified no published journal articles addressing the association specifically between walking and resilience.
Outcome 8: social isolation and loneliness
The topic of ‘social health’ is broad, and for the purposes of this scoping review we have restricted the focus to social isolation and loneliness given their direct impact on mental health.71 We identified five studies.62 72–75 A cross-sectional study found significant positive associations for frequency of contacts with neighbours, neighbours’ social support, neighbourhood involvement and participation, and walking behaviour.72 However, four intervention studies showed mixed evidence.62 73–75
As noted previously,71 76 the social environment is complex and lacks consensus regarding definitions of core constructs, which we believe has limited this scoping review. In line with the call to action by Hunter et al in this special edition,71 further research in this area is required to (1) create a taxonomy providing a consensus of definitions for core concepts of the social environment; (2) synthesise this complex evidence base to better guide the development of theory and conceptual models for walking behaviour and mental health; and (3) develop interventions that use walking to promote social interactions to enrich existing social networks or help create new social networks.
Summary of key findings for mental health outcomes
Table 2 summarises the state of the evidence for walking and the eight mental health outcomes included in this study. Depression and anxiety are the two outcomes with consistent evidence for beneficial effects. Self-esteem, PWB, SWB and psychological stress have either limited or mixed findings for prevention and treatment. We found no studies investigating resilience. Social isolation and loneliness remains a particularly complex area requiring further conceptual mapping. The volume and distribution of study type suggests that there is a particular evidence gap for prospective designs (see figure 2).
Summary of key findings for mental health outcomes

Distribution of studies by outcome.
Discussion
We aimed to scope and understand what is known about the associations and effects of walking when considering various specified mental health outcomes. To our knowledge, this is the first review of the evidence of multiple mental health outcomes and walking. We have shown areas where the evidence base is well developed, and also areas where it is limited and findings are mixed.
Key concepts and research gaps in the walking and mental health literature
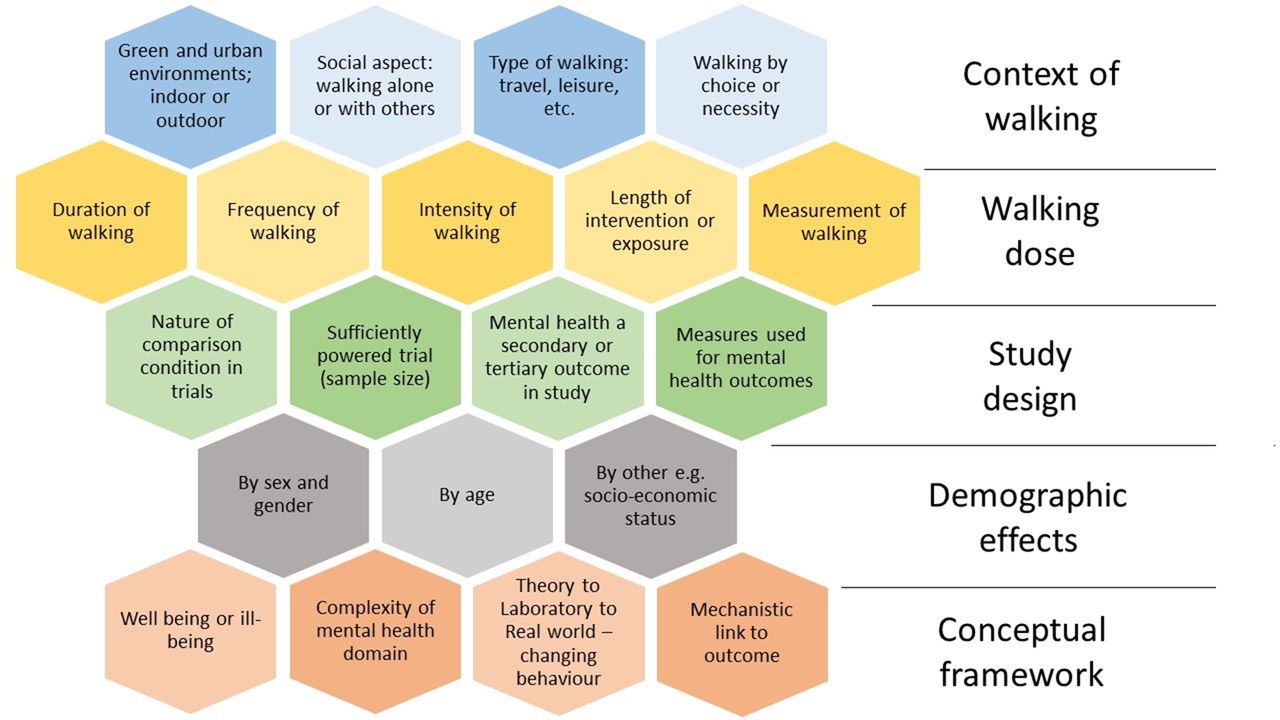
Having addressed the nature and sources of evidence for walking and mental health, we then mapped the key concepts in the included studies and highlighted research gaps and priorities.9 These are displayed in figure 3, organised in five overall themes: (1) context of walking, (2) dose of walking, (3) study design, (4) demographic effects and (5) conceptual framework.

{kind=link}
{kind=link}
{kind=link}
Key concepts and research gaps in the walking and mental health literature.
Context of walking
A considerable proportion of studies compared the effect of setting or type of walking. Additional papers that did not meet the inclusion criteria included studies on types of outdoor environment,77 green environments compared with urban,78–80 forest settings,81 parks compared with woodlands82 and green exercise that included walking.83 They suggested a multitude of positive effects on a range of mental health outcomes for green, outdoor and natural environments, with variations by types of green settings.
A 2011 systematic review of indoor versus outdoor exercise identified 11 studies, 7 of which were walking.84 Outdoor walking showed positive effects across a range of mental health outcomes compared with indoor walking, as well as increased intention for future walking. However, the authors concluded that there was still a paucity of high-quality evidence. A 2010 systematic review of mental health effects of walking in natural versus synthetic environments had similar findings.85 Conversely, the social context, whether walking alone, with friends, partners or in a group, has not been extensively studied.
There was insufficient evidence to draw conclusions on purpose of walking. This issue may be more critical than physiological dose for both effect and public health messaging. Very few studies we identified compared, for example, commuter walking to leisure walking or dog walking. Furthermore, the difference between walking by choice, or necessity, is not well understood. More needs to be known about the role of context of walking, and this is a clear research priority.
Dose of walking
Differential ‘dose–response’ effects by frequency, duration, intensity and length of intervention or exposure time are not yet well understood. More needs to be known about the optimal dose of walking to benefit different mental health outcomes and the relative importance of this factor. Intensity of walking is a particular area of interest. The differences between a brisk walk, a slow shuffle and the differential effects as fitness declines with age and relative intensity of walking increases need to be better understood for effective public health messaging and intervention. Increasing evidence suggests physiological health effects for walking differ by intensity;86 it is important to understand if the same is true for mental health.
Understanding these dose-related factors will be intrinsically linked to how walking is measured. When considering intensity, self-report measures can explore perceived intensity, within the limitations of recall bias, while objective measures like pedometers may be able to assess cadence. Measures of pace/speed and associated measurement of aerobic fitness or response may be required. Our scoping review found that measurement of walking varies considerably, and much learning is required in this area.
Study design
In terms of study design, there are evidence gaps around the nature and content of comparison conditions, sample sizes with many small studies and insufficiently powered analyses of mental health outcomes as secondary or tertiary outcomes. Selection and application of appropriate mental health measures is also a key concept in the literature.
Demographic effects
The effects of walking by sex, age, socioeconomic status and other important demographics remain a research priority. We are not able to say if existing evidence is generalisable across demographics. The potential interaction of demographics with dose and context of walking is another important research gap.
Conceptual framework for walking and mental health
This review highlights areas where the theory of walking and mental health could be expanded through development of an appropriate conceptual framework. The different outcomes, the complexity of the outcomes, the development of ecologically valid interventions and understanding the mechanisms could benefit from an agreed framework.
There is comparatively less research on mental well-being (eg, SWB, self-esteem) as opposed to mental ill-being (eg, depression, anxiety) particularly for interventions. It is important to note that these are independent mental health constructs rather than descriptors that sit at opposite ends of the same spectrum. While the absence of depression or anxiety is clearly desirable, it does not necessarily equate to high levels of SWB or self-esteem. This mirrors the overall definition of health—not merely the absence of disease, but the presence of well-being—and serves as a reminder of the holistic nature of public health in practice. It may also be an important factor to consider when developing public health messaging that is targeted at behaviour change. Specifically, positive messages about improving well-being through walking may resonate more with segments of the population than the disease-aversion messages that have historically pervaded the health promotion sector. Further investigation of the relative contribution of walking to well-being and ill-being outcomes is indicated and should also take into the account the most effective methods to influence physical activity behaviour.
The complexity of the mental health domain was a key theme. To quote one of the included studies, ‘Mental health is a vast and complex domain, which reaches far beyond symptoms, disorders and diagnoses.’27 Whether studies looking at single outcomes could address this domain adequately is for discussion. The reductionist nature of examining these outcomes in isolation may not be appropriate when considering the interwoven nature of psychological constructs and the high prevalence of comorbid mental illnesses, while studies with multiple outcomes may be accused of cherry-picking favourable findings. Furthermore, despite efforts to define different mental health outcomes in the literature, there appears to be ongoing confusion and conjecture in the language to describe these constructs. This was particularly challenging when attempting to categorise studies that used varying outcome definitions.
To have population-level effects, there is a need to transfer promising laboratory and treadmill findings to ecologically valid, free-living settings. This will require the development of robust programme theory to understand and evaluate delivery and impact. Similarly, the need to establish and understand mechanisms of effect is an important priority for future research. For example, is it the physiological dose of walking that provides the effect or is walking a vector for increased social contact and support? Or is it a combination of pathways?87 Furthermore, the interaction and relative importance of the contextual setting (eg, forest trail vs urban street) of walking and its underlying purpose (eg, leisure vs commute) remains unclear.
Implications and future research
Our findings suggest that while the gap identified by Morris and Hardman has seen a growth in research and evidence, it is not as developed as other areas (eg, physiological responses, cardiovascular disease or all cause-mortality). Nor is it as developed as we expected when we began this review. Specifically, once mental health was categorised into individual outcomes, in many cases the number of studies found was not high. There remains a vast number of questions and evidence gaps as summarised in figure 3.
The implications for future research clearly include addressing the limited volume and quality of prospective and intervention studies for each mental health outcome. In terms of policy and practice, discussion and expert consensus is required on whether the current evidence base is sufficient to make recommendations for walking and mental health. For example, to what extent could the mental health benefits of walking be included in the upcoming update of physical activity guidelines by the UK Chief Medical Officers?
Strengths and limitations
The present study has a number of strengths. It is the first review of such a broad range of mental health outcomes specific to walking. It considers both prevention and intervention effects, and it identifies the volume and distribution of the evidence base. This has shown where we have good evidence for walking, and where more research is warranted. We have also mapped the key concepts and research priorities within the literature.
There are a number of limitations to consider. We only included quantitative studies. This decision was made as qualitative designs address different questions outwith our research aims. However, several qualitative studies were evident in the searches and a similar review of this evidence could be highly instructive. As with any review, publication bias is an issue. It is not clear how many other studies showed no effect or deleterious effects and were not published.
In many studies, walking was reported as physical activity or aerobic exercise. Alternatively, the exposure or intervention was walking and running/jogging or progression from walking to jogging. This excluded a large volume of literature. We did not include a number of critical outcomes such as dementia, cognitive function, mood and HRQoL. These contribute substantially to health burden. Additionally, we did not include secondary effects in clinical populations. There is a substantial volume of literature in these populations that may need scoping in the future.
It was necessary to limit our search terms and publication language to ensure the review was feasible and focused. It is possible we missed some important literature and a broader search strategy would have identified additional relevant studies.
Conclusions
Walking is known to benefit physical health. We have shown how the evidence base for specific mental health outcomes and benefits has grown since Morris and Hardman’s ‘Walking to Health’ review in 1997.7 In 1997, they stated that ‘the pleasurable and therapeutic, psychological and social dimensions of walking, whilst evident, have been surprisingly little studied’. Despite the growth in the evidence base, given the importance of mental health, and the evidence gaps identified, we think this statement still holds true. We anticipate that this scoping review will stimulate more research in this area.
What are the new findings?
Over the last 20 years the evidence base for the beneficial effects of walking for mental health has grown, but remains fragmented and incomplete for some important outcomes.
For depression and anxiety, there may be sufficient evidence to promote walking to prevent and treat these conditions.
There has been more research on the negative disease-based outcomes (such as depression and anxiety) than for the positive well-being outcomes (such as happiness or subjective well-being).
The evidence base seems to indicate that across the mental health outcomes there are additional benefits from walking outdoors in natural environments compared with indoor, treadmill-based walking.
Acknowledgments
The authors thank Marshall Dozier, Evy Horton and Olivia Alliott for their help and support.
References
Footnotes
Contributors PK conceived the study. PK, NM, AGN, JR and CW designed the search strategy. CW conducted searching of databases. PK and CW screened records. All authors contributed to screening full texts. All authors led analysis and writing for at least one mental health outcome. PK and CW drafted the full manuscript, and all authors reviewed and approved final submission.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.