Article Text

Abstract
Background Preprofessional dancers partake in rigorous training and have high injury prevalence. Attempts to identify risk factors for dance injuries have focused on a diversity of intrinsic and extrinsic factors.
Objective To identify and evaluate the evidence examining risk factors for musculoskeletal injury in preprofessional ballet and modern dancers.
Methods Fifteen electronic databases were systematically searched to October 2015. Studies selected met a priori inclusion criteria and investigated musculoskeletal injury risk factors in preprofessional (elite adolescent, student, young adult) ballet and modern dancers. Two reviewers independently assessed the quality and level of evidence using the Downs and Black (DB) criteria and a modified Oxford Centre of Evidence-Based Medicine 2009 model, respectively.
Results Of 1364 potentially relevant studies, 47 were included and scored. Inconsistent injury definition and methodology precluded meta-analysis. The most common modifiable risk factors investigated were anthropometrics (ie, body mass index, adiposity), joint range of motion (ie, lower extremity), dance exposure (ie, years training, exposure hours) and age. The median DB score across studies was 8/33 (range 2–16). The majority of studies were classified as level 3 evidence and few considered risk factor inter-relationships. There is some level 2 evidence that previous injury and poor psychological coping skills are associated with increased injury risk.
Conclusions Because of the lack of high-quality studies, consensus regarding risk factors for musculoskeletal injury in preprofessional dancers remains difficult. There is a need for injury definition consensus and high-quality prospective studies examining the multifactorial relationship between risk factors and injury in preprofessional dance.
- Injuries
- Risk factor
- Adolescent
- Dance
- Systematic review
Statistics from Altmetric.com
Background
Preprofessional ballet and modern dancers participate in long hours of class, rehearsal and performance. Commitment to this level of training typically begins at a young age (particularly for ballet), occurs during the adolescent growth spurt, and involves repetitive movements (eg, jumps).1–3 Ballet movement often exceeds anatomical limitations (eg, turnout, pointe work)4 and modern dance tends to demand versatility (eg, improvisation, inversions).5 ,6 Rigorous training in both dance styles requires intense physical and artistic skill,7 and may consequently increase dancers’ susceptibility to musculoskeletal injury.8 Not surprising, the scope of epidemiological literature suggests that the most predominant musculoskeletal injuries in dance are overuse and lower extremity injuries.1 ,4 ,9 ,10 Reported prevalence and incidence rates of musculoskeletal injuries among dancers indicate that dance is a high-risk activity regardless of the style and level of participation.11–13 For example, Luke et al4 estimated an injury rate of 4.7/1000 dance hours in preprofessional adolescent ballet students, a rate comparable to youth indoor soccer (4.5/1000 h),14 and higher than that reported in elite adolescent gymnasts (2.6/1000 h),15 and ice skaters (1.4/1000 h).16
The burden of injury in the preprofessional dance population is of interest as injury may limit participation in class and performance, and consequently inhibit artistic development. This is particularly relevant for young dancers due to the financial implications of injury as well as to their limited timeframe for achieving artistic and academic goals.17 Additionally, the long-term consequences of musculoskeletal injury include increased risk for post-traumatic osteoarthritis and associated mobility disability, which in turn, can increase cardiometabolic risk.18
To date, studies aimed at identifying risk factors for musculoskeletal injury in dancers of all styles have suffered from inconsistent injury definitions, non-optimal study designs (ie, cross-sectional), limited sample size, a lack of simultaneous consideration of exposure and have focused on a heterogeneous group of potential risk factors.12 ,13 ,19 A systematic review of injury risk factors specific to preprofessional dancers and based on critical appraisal of the evidence is lacking. Therefore, the objective of this systematic review was to identify and critically appraise the evidence examining risk factors for musculoskeletal injury in preprofessional ballet and modern dancers.
Methods
This review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.20
Data sources and search
Fifteen online databases were searched from inception to October 2015 by the lead reviewer (SJK). Databases were selected based on their relevance to the research topics of health, medicine, kinesiology, sport and dance. These databases included: Web of Science; OVID (MEDLINE In-Process, EMBASE, PsycINFO, HealthSTAR, Cochrane Database of Systematic Reviews); EBSCO (CINAHL Plus, SPORTDiscus, International Bibliography of Theatre and Dance with Full Text); PubMed; Elsevier (ScienceDirect); ProQuest (International Index to the Performing Arts, Dissertations); SafetyLit; and PEDro: the Physiotherapy Evidence Database. In addition, Solomon and Solomon,21 a text of English language publications in Dance Medicine and Science (3260 references published between 1960 and 2011), was comprehensively hand-searched by subject.
For each online database, specific Medical Subject Headings (MeSH) and text words (table 1) were searched independently in order to obtain the total number of studies. Combinations of search terms then formed relevant search strategies (table 2). Related subject headings reviewed in Solomon and Solomon21 included: adolescent dancers, dance injury, ballet injury, injury survey, risk factors, and injury prevention.
MeSH and tw used for online database search strategy
Example of full electronic search strategy used for each online database
Limits were set to include only peer reviewed, English language publications on human populations. The number of studies obtained from each search strategy was recorded. The titles and corresponding abstracts of results less than 500 were scanned to identify those potentially relevant. If a title did not have an accompanying abstract, the full article was scanned to ensure that a potentially relevant study was not overlooked. Reference lists of selected articles were hand-searched to identify appropriate studies not found by the search strategies. The lead reviewer (SJK) determined final study selection after examining the full text of all potentially relevant studies. Manuscripts were organised using the reference management software package, EndNote X6.0.2 (Thomson Reuters, 2012).
Study selection
Studies were included if they investigated the association between any potential injury risk factor (defined as any factor that may increase the potential for injury) or injury prevention strategy for dance injury (defined as any injury sustained during dance participation). Additional a priori inclusion criteria included: primary research of original data; analytic design (ie, experimental, cohort, case–control or cross-sectional); and study participants that included elite adolescent (18 years or under), young adult, student, or preprofessional ballet and modern dancers. Reviews (systematic and narrative) and case studies were excluded after their reference lists were examined in order to identify appropriate studies for inclusion. In addition, editorials, commentaries, and opinion-based papers; findings not specific to dancers (ie, where dancers’ information was combined with other athletes’); findings not specific to elite adolescent (18 years or under), young adult, student, or preprofessional dancers (ie, where young dancers’ information was combined with professional dancers’); and forms of dance for recreation and exercise (ie, aerobic, cheerleading, social, clubs, raves) were excluded.
Data extraction and study rating process
The following data was extracted from each study: study location and population (dance style, level, age, sample size), injury outcome (definition), injury estimates (incidence proportion, incidence rate, prevalence), measures of risk (difference in means, correlations, odds ratio (OR), incidence rate ratios (IRR) and risk ratio (RR)), risk factors and results (significant and non-significant). If available, injury estimates (injury rates) were used to estimate point estimates of IRR (injury rate in exposed/injury rate in unexposed). Two reviewers (SJK, JLW) independently assessed the quality and level of evidence for included studies. Quality of evidence was evaluated based on criteria for internal validity (study design, quality of reporting, presence of selection and misclassification bias, potential confounding) and external validity (generalisability) using the Downs and Black (DB) quality assessment tool. The DB criteria assigns an individual score calculated of 33 total points for each study (10 points for reporting, 3 points for external validity, 7 points for bias, 3 points for confounding and 1 point for power: see online supplementary appendix 1).22 The level of evidence represented by each study was categorised based on a modification of the Oxford Centre of Evidence-Based Medicine (OCEBM) 2009 model (see online supplementary appendix 2).23 The 2009 model of the OCEBM was chosen over the 2011 model as it more clearly demonstrated the distribution of the current dance science literature with regard to the hierarchy of evidence. It has also been used in a previous systematic review on risk factors for groin injury in sport.24 To accommodate the high quantity of cross-sectional studies identified, the 2009 OCEBM model was modified such that level 3 included cross-sectional study designs. As per study exclusion criteria, levels 1a, 2a, 3a (systematic reviews), 4 (case series) and 5 (opinion-based papers) were not included. Discrepancies in DB scores or OCEBM categorisation were resolved first by consensus between the two reviewers who rated the study and if required, by a third reviewer (CAE).
Data synthesis
Extracted data, quality and level of evidence across all studies were summarised. The quantity, quality and level of evidence for the most commonly investigated modifiable and non-modifiable risk factors for musculoskeletal injury in preprofessional ballet and modern dancers were collated.
Results
Identification of studies
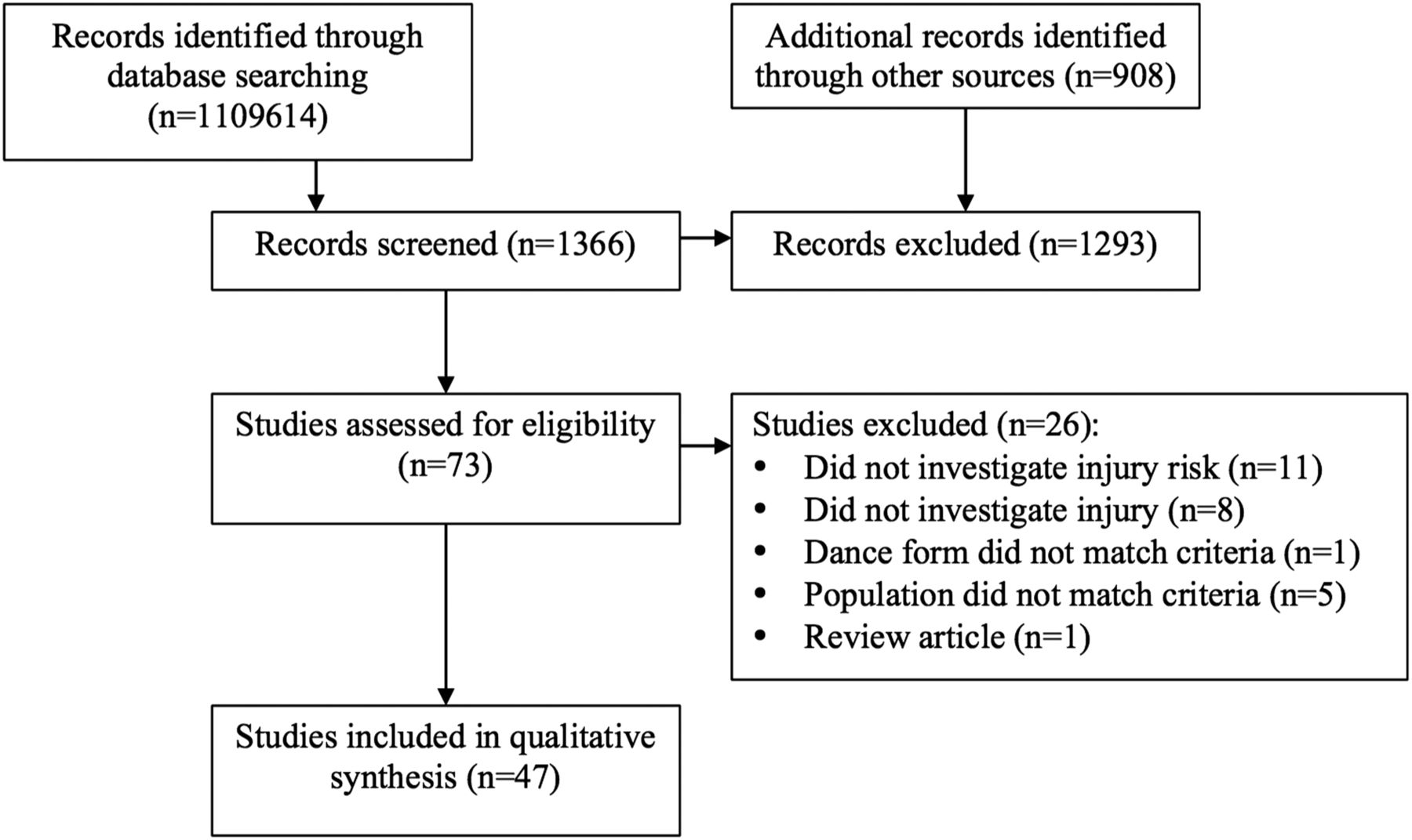
The initial search yielded 1364 potentially relevant studies. Following the removal of duplicates and studies not meeting inclusion criteria (ie, injury and injury risk were not investigated, population or dance form did not match criteria), 73 studies remained. A search of reference lists failed to identify additional studies. Subsequent to further evaluation by the two independent reviewers, 47 studies were deemed appropriate for critical appraisal (figure 1).
{kind=link}
Adapted Preferred Reporting Items for Systematic reviews and Meta-Analyses flow chart of study selection.
Study characteristics
Characteristics of the 47 included studies are summarised in the online supplementary appendices 3 and 4. Studies consisted of 27 cross-sectional and 20 follow-up studies (4 controlled trials (2 true, 2 quasi), 15 cohorts (13 prospective, 2 retrospective), and 1 case–control) representing 10 different countries. Among the 20 follow-up studies, the median time to follow-up was 10 months (ie, 1 academic year) with a range of 15 weeks (prospective cohort)25 to 5 years (retrospective cohort).1 The median number of participants per study was 60 (range 1326–278627). The combined total number of preprofessional ballet and modern dancers investigated across studies was 7978. Ten studies did not report sex. Of those that did, 22 investigated female and male participants, 14 focused solely on females, and 1 included males only. The combined total of females reported was 2360 (range 928–58829) and males was 822 (range 230 ,31–28129).
Eighteen studies did not include an injury definition. Of those that did provide a definition, variations of modification to dance participation/time loss was the most common (n=18). Only two very recent studies included multiple definitions relating to time loss, medical attention, and physical symptoms.2 ,32 Twelve studies defined specific types/locations of injuries. These included: stress fractures,33–35 patella28 and Achilles tendinopathy,36 hamstring injuries,37 shin splints,38 lumbosacral pain,30 ,39 hip/knee pain,40 and ankle sprains.41 ,42
Injury estimates
Descriptions of injury estimates (incidence proportion, incidence rate, prevalence), effect estimates (IRR, RR, OR) and significant and non-significant injury risk factors are presented in the online supplementary appendices 3 and 4. Of the 27 included cross-sectional studies (see online supplementary appendix 3), an injury estimate was reported in 16. The most common estimate reported was prevalence of previous injury (8 studies; range 47–100%) with a time of recall ranging from 6 months to a dancer's lifetime. Reported prevalence of previous injury specific to the lower extremity (ie, low back, hip, knee, hamstrings) ranged from 6% to 62%. Of the 20 follow-up studies, representing controlled trials, cohorts and a case–control research design (online supplementary appendix 4), 17 reported injury estimates. The most common were incidence proportions (10 studies; range 37–85%) and incidence rates per 1000 dance hours (8 studies; range 0.77–4.71 injuries/1000 dance hours).
Quality and level of evidence
On the basis of the DB criteria, the median methodological quality of all 47 studies was 8/33 (range 2–16). The aim of the DB criteria is to assess the methodological quality of scientific research (inclusive of experimental as well as observational studies). Owing to the majority of included studies being observational in nature, 7 items (4, 8, 14, 19, 23, 24 and 27; totalling 10 points) on the DB checklist were not applicable. Therefore 43 of the 47 articles did not have the opportunity to achieve a full score due to their study design.
The highest level of evidence demonstrated by all reviewed studies was level 2b (ie, low-quality randomised controlled trials and cohort studies). The majority (27/47) of studies were classified as level 3c (ie, cross-sectional design).
Synthesis of results
Reported significant and non-significant findings, along with the quantity, quality and level of evidence of each study, are summarised in table 3.
Summary of significant and non-significant injury risk factors by quantity, quality and level of evidence
Level 2 evidence suggests that the following factors are significantly associated with increased risk of injury in preprofessional dancers:
Psychological factors
Anthropometrics
Poor aerobic capacity25
Level 3 evidence suggests that there are significant associations between dance injury and:
Psychological factors
Lower extremity alignment
Sacrum inclination angle in turnout greater than 30° (for lumbosacral pain)39
Jump landing technique
All remaining risk factors across all included studies were inconclusive (ie, showed equal reports of significant and non-significant results) or reported null findings.
Discussion
To the best of our knowledge, this is the first systematic review to evaluate risk factors for musculoskeletal injury in preprofessional ballet and modern dancers through critical appraisal.
Key findings—risk factors
Despite the quantity of risk factors investigated, the critical appraisal of included studies suggests that the quality and level of evidence is lacking and therefore little consistency in findings exists, which is similar to conclusions drawn in two previous systematic reviews.12 ,13 For example, among the most common risk factors investigated (ie, anthropometrics (n=18), lower extremity joint range of motion (n=18), dance exposure (n=15), and age (n=12)), evidence remains inconclusive, as there are similar reports of significant and non-significant associations with dance injury, regardless of study design.
Significant findings from the strongest level of evidence (ie, low-quality randomised controlled trials and prospective cohort designs) indicate that previous injury43–45 and insufficient psychological coping skills (ie, freedom from worry, confidence, negative dance stress)46 ,47 are modifiable risk factors for injury in preprofessional dancers. These findings are not surprising considering the high physical, psychological and artistic demands of dance training, particularly at the preprofessional level.7 Given the ‘fear and avoidance’ culture prevalent in dance, that few preprofessional dancers seek medical attention for fear of having to discontinue,5 ,53 ,54 it is highly likely that dancers do not fully recover from their initial injury. In sport, inadequate rehabilitation from an initial injury is also suggested as a mechanism behind previous injury as a risk factor.24 While having a previous injury may not be modifiable, the importance of rehabilitation from an incurred injury, prior to returning to full dance training may be a key ingredient in the education and subsequent injury prevention of young dancers.
Competitive auditions, approaching performances, relationships with choreographers, maintaining ideal body weight and living away from home are examples of stressors unique to preprofessional dancers.50 Patterson et al55 found that dancers often seem to experience injuries as much from psychological factors as physical. Quasi-experimental research supports this whereby young ballet dancers who learned imagery, self-talk, and relaxation techniques enhanced their psychological coping skills and as a result reduced their injury frequency and duration compared with dancers who did not experience these skills.46 Psychological skills can be considered modifiable and should be included in the development of future injury prevention programmes.
On the basis of a limited number of prospective cohort studies, it is also plausible that anthropometrics (ie, low BMI,48 low adiposity,25 large lower limb circumference29), irregular menses,29 ,48 and dance exposure (ie, high volume and level of dance training and high duration of previous training29 ,56) are potential risk factors. However, many of these risk factors are based on only one or two studies, warranting further investigation.
Consensus regarding specific risk factors for dance injury in preprofessional ballet and modern dancers could not be established because of the heterogeneity of factors investigated. For example, multiple studies investigated joint motion at the hip, yet the extensive variety of methods employed to explore this potential risk factor (ie, passive vs active, right/left vs total, inclusion of dance-specific positions) made comparisons difficult. Based on this systematic review, it is not possible to determine whether the inconclusive or conflicting evidence for most risk factors investigated was due to a lack of comparable studies or to the risk factors themselves.
Quality of evidence
On the basis of the DB assessment, incomplete description of participant characteristics and not accounting for participants lost to follow-up were common areas where studies consistently failed. Alleviation of such systematic errors include more in depth reporting of participant characteristics (ie, age, sex, style and level of dance training, average volume of training, a description of why some dancers participated in the study and others did not), as well as reporting characteristics for those participants who were lost to follow-up. By doing so, appropriate judgments can be made as to the direction and magnitude of potential selection bias that may impact results.
The use of invalid or unreliable measures was also common in the evaluating DB criterion. The internal validity of a study can be severely compromised if a measurement tool is invalid because it is not clear that the tool is measuring what it is supposed to measure. If a tool is unreliable, the degree of consistency in measures produced is also uncertain.57 Pilot testing of the measurement tool(s) and the assessor(s) would alleviate whether or not measures are deemed invalid or unreliable.
Owing to the widespread lack of power in the majority of the studies, it is possible that the limited significant findings of risk factors in the reviewed papers is related to insufficient sample sizes. An additional DB criterion that all 47 included studies did not meet was reporting adjustment for potential modification or confounding. This is of great concern because interpretations of all findings may be incorrect.58
Level of evidence
In the evaluation of research, a hierarchy of evidence exists that ranks specific study designs in order of decreasing internal validity.59 Based on this systematic review, the predominant study design was cross-sectional, whereby exposure and outcome data are measured at the same time. These designs are important as they may identify associations between the injury and risk factor(s), which informs the development of future cohort studies. They cannot however, confirm causal relationships.60 In addition, injury proportions, as reported by cross-sectional research, do not provide information about injury risk, the quantification of the relationship between risk factors and injuries, nor account for different levels of exposure to risk factor(s),60 negating the dynamic, multifactorial nature of dance injury altogether.61 To investigate risk factors for sport (dance) injuries most appropriately, Bahr and Holme19 suggest the use of higher level, analytic evidence: case–control studies, cohort studies or experimental studies. These designs address the single necessary Hill criterion for a variable of interest to be a causal factor in the exposure–outcome relationship: temporality.62
Further to the poor quality and low levels of evidence, inconsistencies in injury definition also contributed to the lack of evidence reported by included studies. Due to the range of definitions utilised, reviewers were unable to collate summary injury measures. As outcome and exposure data could not be pooled due to heterogeneity, an alternate qualitative classification of levels of evidence, best evidence synthesis,63 was considered. While the use of the best evidence synthesis model would not have changed the findings of this systematic review, all included studies would have been simply classified as either ‘Limited evidence’ (evidence provided by only one study with low quality) or ‘Conflicting evidence’ (inconsistent findings in multiple studies; <75% of the studies reported consistent findings). It was the authors’ intention to provide as much detail as possible in the evaluation of the levels of evidence to illustrate the breakdown of study designs and to explain the reason for hierarchy in scientific study.
Recommendations
Exposure to multiple risk factors for injury in dance can be considered repetitive, under changing and dynamic conditions throughout dance participation.61 As such, future epidemiological studies examining risk of injury in young dancers should be prospective and exposure and outcome data should be collected at regular intervals. In a recursive model for sport (dance) injury risk, Meeuwisse et al61 also suggest that researchers capture risk factor data during an aetiologically relevant time period, looking back from the time of injury, in addition to looking forward from the beginning of the season. The calculation of injury prevalence and injury incidence will enable a more complete picture of the true magnitude of dance injuries. Further, an understanding of the implications of different operational definitions of injury and how they relate to specific research questions needs to be made.64
Validity and reliability studies need to be conducted prior to research. A focus on the specific risk factors found to be significant from higher levels of evidence will improve the direction of future research. It is also highly recommended that in future research the use of multivariate regression modelling be considered such that potential effect modification and confounding can be addressed in injury risk factor analysis.
Limitations
Despite a comprehensive search strategy and rigorous approach to study selection, it is possible that relevant studies were excluded; particularly as only English language studies were evaluated and only general MeSH terms and text words pertaining to ‘injury’ and ‘risk factors’ were searched. Systematic reviews are also subject to the same limitations present in each of the included studies. Considering that most studies were observational and not experimental, the appropriateness of the DB criteria to evaluate the quality of evidence is questionable, as the aim of the DB checklist includes the appraisal of experimental research. In total, 43 of the 47 studies did not have the opportunity to achieve a full score. The findings from this systematic review may not be generalisable beyond female dancers due to the limited inclusion of male participants in the studies reviewed.
Owing to heterogeneity (ie, definition of injury, measurement of risk factors), a meta-analysis was not possible. Many studies examined multiple risk factors within one study sample without controlling for potential confounders, impacting the accuracy of results. Moreover, these studies did not examine the presence of two or more risk factors in combination, limiting assessment of potential interaction of risk factors that may be associated with musculoskeletal injuries in young dancers. The lack of rigour in the design and analysis of data impacts the interpretations of results, subsequently limiting conclusions drawn from this systematic review.
Strengths
To the best of our knowledge, this is the first systematic review to utilise critical appraisal in the examination of risk factors for musculoskeletal injury specific to preprofessional ballet and modern dancers. A comprehensive, transparent and reproducible approach was followed. The extraction and comparison of specific characteristics from included studies, along with the evaluation of both the quality and level of evidence, contribute greatly to the direction and rigour of future research.
Summary
Because of a lack of high-quality studies, consensus regarding risk factors for dance injury remains difficult. There is some level 2 evidence to suggest that previous injury and insufficient psychological coping strategies are associated with increased risk of musculoskeletal injury in preprofessional ballet and modern dancers. To assist in the development of best practices for preparticipation screening and subsequent injury prevention, there is a need for high-quality studies that examine the relationship between risk factors and injury in dance.
What are new findings?
There is some level 2 evidence to suggest that previous injury and insufficient coping psychological strategies are associated with increased risk of musculoskeletal injury in preprofessional ballet and modern dancers.
Future epidemiological studies on preprofessional dancers need to be prospective, operationalise injury definitions, collect exposure and outcome data at regular intervals and employ multivariate regression modelling.
How might it impact on clinical practice in the future?
Due to the lack of high-quality studies and the heterogeneity of risk factors assessed, a consensus regarding risk factors for musculoskeletal injury in preprofessional dancers remains a challenge. At this time, recommendations for musculoskeletal injury risk screening for this population in a clinical setting is limited to the inclusion of preparticipation evaluation of injury history.
Acknowledgments
The authors would like to acknowledge Alix Hayden, Faculty of Kinesiology Librarian at the University of Calgary.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
- Data supplement 3 - Online supplement
- Data supplement 4 - Online supplement
Footnotes
Twitter Follow Jackie Whittaker at @jwhittak_physio
Contributors All authors were responsible for the conception and design of the study. SJK extracted data from the included studies, while SJK and JLW independently reviewed the literature. SJK was the primary author in preparing the manuscript, however all authors contributed to the interpretation of the findings and critical manuscript revision prior to submission.
Funding The Sport Injury Prevention Research Centre is supported by an International Olympic Committee Research Centre Award. SJK is funded by a Talisman Energy Research Fund in Healthy Living and Optimising Health Outcomes. CAE holds a Chair in Pediatric Rehabilitation Alberta Children's Hospital Foundation.
Disclaimer The sponsors had no involvement with respect to design, data collection, analyses, interpretation, writing or submission of this systematic review.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.