Article Text

Abstract
Background There are many injection therapies for lateral epicondylalgia but there has been no previous comprehensive comparison, based on the Bayesian method.
Methods The MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) databases were searched for appropriate literature. The outcome measurement was the pain score. Direct comparisons were performed using the pairwise meta-analysis, and network meta-analysis, based on a Bayesian model, was used to calculate the results of all of the potentially possible comparisons and rank probabilities. A sensitivity analysis was performed by excluding low-quality studies. The inconsistency of the model was assessed by means of the node-splitting method. Metaregression was used to assess the relationship between the sample size and the treatment effect.
Results All of the injection treatments showed a trend towards better effects than placebo. Additionally, the peppering technique did not add additional benefits when combined with other treatments. No significant changes were observed by excluding low-quality studies in the sensitivity analysis. No significant inconsistencies were found according to the inconsistency analysis, and metaregression revealed that the sample size was not associated with the treatment effects.
Conclusions Some commonly used injection therapies can be considered treatment candidates for lateral epicondylalgia, such as botulinum toxin, platelet-rich plasma and autologous blood injection, but corticosteroid is not recommended. Hyaluronate injection and prolotherapy might be more effective, but their superiority must be confirmed by more research. The peppering technique is not helpful in injection therapies.
- Tennis elbow
- Treatment
- Randomised controlled trial
- Review
- Meta-analysis
Statistics from Altmetric.com
Introduction
Lateral epicondylalgia is a common symptom in general clinical practice.1 It is usually considered a self-limiting condition, resolving in approximately 6–12 months regardless of clinical interventions.2 However, for some patients, the symptoms can last for 2 years or longer.3
Conservative treatment includes exercise therapy and joint mobilisation4 as well as pharmaceutical therapies. This review focuses on injection therapy. The most commonly used substance for injection is corticosteroid (CS), which has been used for 60 years.5 Recently developed injection therapies include autologous blood (AB), botulinum toxin A (BT), glycosaminoglycan polysulfate (GSGPS), hyaluronic acid (HYA), prolotherapy (PRO) and autologous platelet-rich plasma (PRP). There have been studies of the ‘peppering technique (PEP)’6 ,7 which refers to entering the skin at one point, followed by multiple redirections of the needle used for injection to perforate the tendon with an even distribution.8 However, there is no consensus regarding which treatments are the most effective.
In recent years, many randomised controlled trials (RCTs) have compared these treatments and systematic reviews and meta-analyses have been published.9 ,10 However, owing to the limitations of RCTs, most of these systematic reviews and meta-analyses could only compare two treatments at a time. To overcome this limitation, network meta-analysis, which is also called multiple-treatment meta-analysis, has been developed to compare different treatments, even if they have never been directly compared.
In a previous network meta-analysis,11 the author compared the treatment effects of different injection therapies for lateral epicondylalgia using a novel method called the ‘single-effect model’. This model was based on the hypothesis that a study had a single variance for every treatment effect. This single variance consisted of different variances corresponding to treatments in the study. This variance could obviously reduce the complexity of the statistics and make comprehensive comparisons possible using traditional statistical methods. However, this hypothesis ignored that the variance of each treatment in a study might be quite different, and this difference could be interpreted as an important characteristic of a certain treatment. Owing to this limitation and many new RCTs being published since, we conducted a new network meta-analysis. In this Bayesian network meta-analysis, we aimed to provide some useful information about comparisons of different injection therapies for lateral epicondylalgia.
Materials and methods
Eligibility criteria
RCTs were considered eligible if they met all of the following criteria: (1) adults (older than 18 years); (2) diagnosed with lateral epicondylalgia but not caused by significant trauma or other systemic diseases; (3) at least two injection therapies for lateral epicondylalgia evaluated, including placebo (PLA) or a ‘wait and see’ strategy; and (4) results of pain relief or functional recovery reported.
Search strategy
The MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) databases were searched from the start of each database to 6 August 2014. MEDLINE and EMBASE were searched together via http://www.embase.com (Elsevier, the Netherlands). The search was based on the following keywords: tendinitis, tendinopathy, tendon injury, epicondylalgia, epicondylitis, tennis elbow, common extensor origin and lateral/external elbow pain with the limitation of RCT (box 1). To avoid the potential omission of novel injection methods, no other limits were applied. In addition, every available review related to the treatment of lateral epicondylalgia was scanned manually for any possible additional studies. No language limits were placed on the searches.
Search strategy for http://www.embase.com (step by step)
#1 ‘tendinitis’/exp OR ‘tendinitis’
#2 ‘tendon injury’ OR ‘tendon injury’/exp
#3 tend?nit* OR tend?nos* OR tend?nopath*
#4 #1 OR #2 OR #3
#5 ‘elbow’ OR ‘elbow’/exp OR elbow*
#6 #4 AND #5
#7 ‘epicondylalgia’ OR ‘epicondylalgia’/exp
#8 ‘epicondylitis’ OR ‘epicondylitis’/exp
#9 ‘pain’ OR ‘pain’/exp OR pain* AND (‘elbow’ OR elbow* OR ‘elbow’/exp) AND (‘lateral’ OR ‘external’)
#10 ‘tennis elbow’ OR ‘tennis elbow’/exp
#11 ‘common extensor origin’
#12 #6 OR #7 OR #8 OR #9 OR #10 OR #11
#13 random*:ab,ti OR factorial*:ab,ti OR crossover*:ab,ti OR placebo*:ab,ti OR control*:ab,ti OR trial:ab,ti OR group*:ab,ti OR ‘crossover procedure’/exp OR ‘single blind procedure’/exp OR ‘double blind procedure’/exp OR ‘randomised controlled trial’/exp
#14 #12 AND #13
Study selection
Two reviewers (WD and X-BL) independently screened the titles and abstracts of all of the retrieved studies for any potentially eligible trials, and the full texts were obtained and scrutinised if necessary. The discrepancies were assessed and discussed by WD and X-BL, and a third reviewer (Z-LW) was consulted if necessary.
Data extraction
All of the relevant data from the included studies were extracted by two reviewers (WD and X-BL) independently. Then the extracted data were checked by WD. The discrepancies were referred to a third reviewer (F-LK). The extracted information included authors, publication year, follow-up (in weeks), the name of the interventions, the number of patients and treatment outcomes. Change in pain score was used as the outcome measurement, including the visual analogue scale (VAS), the Numerical Rating Scale (NRS), a Likert scale or a pain score subscale for other outcome measurements. The values of these pain scores were adjusted to the range of 0–10 if necessary, with 0 indicating no pain and 10 indicating the worst imaginable pain. The changes in the pain scores were calculated, and a negative value represented pain relief. Studies were excluded in this stage if their results were reported as neither mean±SD (SE) nor other forms which could be converted to it.
Small differences in treatment details, such as dosages or schedules, were omitted. If there was more than one follow-up duration reported, the time point that was nearest to 6 months (26 weeks) was adopted. ‘PEP’ was considered an independent treatment that could be added to other injections. All of the included treatment names and their abbreviations are shown in box 2.
Abbreviations of treatment names
AB, autologous blood
BT, botulinum toxin
CS, corticosteroid
GSGPS, glycosaminoglycan polysulfate
HYA, hyaluronate
PEP, peppering technique
PLA, placebo and ‘wait and see’
PRO, prolotherapy
PRP, platelet-rich plasma
The Cochrane Risk of Bias Tool of Revman (Review Manager, V.5.2; Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration) was then utilised to assess the quality of the RCTs included.
Statistical analysis
The results are all presented as the weighted mean differences (WMDs) with corresponding 95% CIs. If the null value (0) was not included in the 95% CI, a statistically significant difference was considered to be detected.
First, pairwise meta-analysis was performed using a random-effects model. The results for all direct comparisons are reported. This process was performed using STATA software (V.12.0; Stata Corporation, College Station, Texas, USA).
Then the direct comparison evidence was integrated, and a network was constructed. A random-effects model, based on a Bayesian framework, was used to analyse the efficacy of all of the treatments simultaneously.12 The network meta-analysis was performed using Markov chain Monte Carlo (MCMC) methods in WinBUGS software (Bayesian inference Using Gibbs Sampling for Windows, V.1.4.3; Imperial College and MRC, UK). Four chains were run using non-informative priors. There were 40 000 iterations in each chain. The first 10 000 iterations were discarded because they were considered burn-in iterations, indicating that they might be affected by the arbitrary initial value. Subsequently, the values in which we were interested were collected with a thinning interval of 10, indicating that 1 sample was collected every 10 iterations, and 3000 samples were collected in each chain. Finally, the average value of 12 000 samples from all four chains was calculated as the final result. Final convergence was an important judgement for the reliability of the results in MCMC, and it was assessed using the Brooks-Gelman-Rubin method.13 In this process, a potential scale reduction factor (PSRF) was calculated by comparing within-chain and between-chain variances. If its value was 1 or very close to 1, approximate convergence was reached. Then the probabilities that a certain treatment was the best, the second best, the third best and so on were calculated. The Surface Under the Cumulative RAnking (SUCRA) method was used. The SUCRA value was presented as the percentage of the area under the curve. It ranged from 0% to 100%, where 100% reflected the best treatment effect, and 0% reflected the worst treatment effect without any uncertainty.14
Inconsistency analysis
If there was a ‘loop’ (eg, A-B-C) in the network, each comparison in the loop (eg, A-B) might have an indirect result from other comparisons (eg, A-C and C-B), as well as the direct result, and there might be some difference between these two results. The inconsistency of the model was assessed by means of the node-splitting method,15 which concerned the difference between the results from direct and indirect comparisons. If the p value was smaller than 0.05, an inconsistency was considered to be detected. The node-splitting models were generated by GeMTC software (V.0.14.3; open source software for mixed treatment comparison model generation). The models were then imported into WinBUGS, and the same parameters as described above were used.
Sensitivity analysis and metaregression
Finally, a sensitivity analysis was conducted by excluding low-quality studies. The rank probabilities were recalculated. If no significant difference could be found, the results were considered to be credible.
Additionally, a metaregression was performed to assess the relationship between the sample size and the treatment effect. A single interaction term was used as the covariate, as recommended by the UK's National Institute for Health and Care Excellence.16 The deviance information criterion (DIC) was used as a measurement of model fit.17 A lower value of the DIC suggested a more parsimonious model. At the same time, a regression coefficient with its 95% CI was also calculated. If there was a significant reduction in DIC, or the null value was not included in the range of the 95% CI of the regression coefficient, the covariate was considered to be associated with the result.
Results
Eligible studies
The search strategy retrieved 1636 related records. The titles and abstracts were screened carefully. Subsequently, the full texts of 169 potentially eligible articles were obtained. We discarded 142 of these articles due to the reason listed in figure 1. Finally, 27 RCTs met the inclusion criteria and were included in the quantitative synthesis procedure.6 ,8 ,18–42 A total of 1913 patients were involved. Table 1 presents the characteristics of the included trials.
Characteristics of the included studies

PRISMA 2009 flow diagram (RCT, randomised controlled trial).
The risk of bias for the included RCTs is shown in figure 2A, B (graph and summary). All of the studies were described as ‘randomised’. However, only 15 of them reported the randomisation details, and the allocations were only properly concealed in 11 of them. As clinical trials, blinding of performance seemed difficult. In the performance bias examination, only 11 of the studies were low risk, and 10 of them were high risk. Furthermore, the blinding of the outcome assessment was clearly described in only 9 of 27 studies.

Risk of bias graph and risk of bias summary.
Results of pairwise meta-analysis
All of the direct comparison evidence was imported into STATA. The WMDs with their corresponding 95% CIs were calculated using a random-effects model. Eighteen pairs of comparisons were performed. The null value was not included in the 95% CIs for seven pairs, which represented a statistically significant difference, and no significant differences were detected in the remaining 11 comparisons. The results are listed in the upper triangle of table 2, and statistically significant differences are shaded.
Results (WMDs, with 95% CIs) of the pairwise and network meta-analysis for pain score
Results of network meta-analysis
The treatment effects measured by changes in the pain score were then used to construct a comprehensive network. Figure 3 presents the relationships of these treatments; the size of the circle represents the number of patients, and the thickness of the line refers to the number of studies that included this comparison. Then the WMDs and 95% CIs of all of the possible comparisons (direct and indirect) were calculated. The PSRFs of all of the values were finally convergent to 1, and strong linearity was observed in graphical diagnostic plots of convergence, representing good convergence. The values of WMDs and their 95% CIs are listed in the lower triangle of table 2, and statistically significant differences are also shaded.
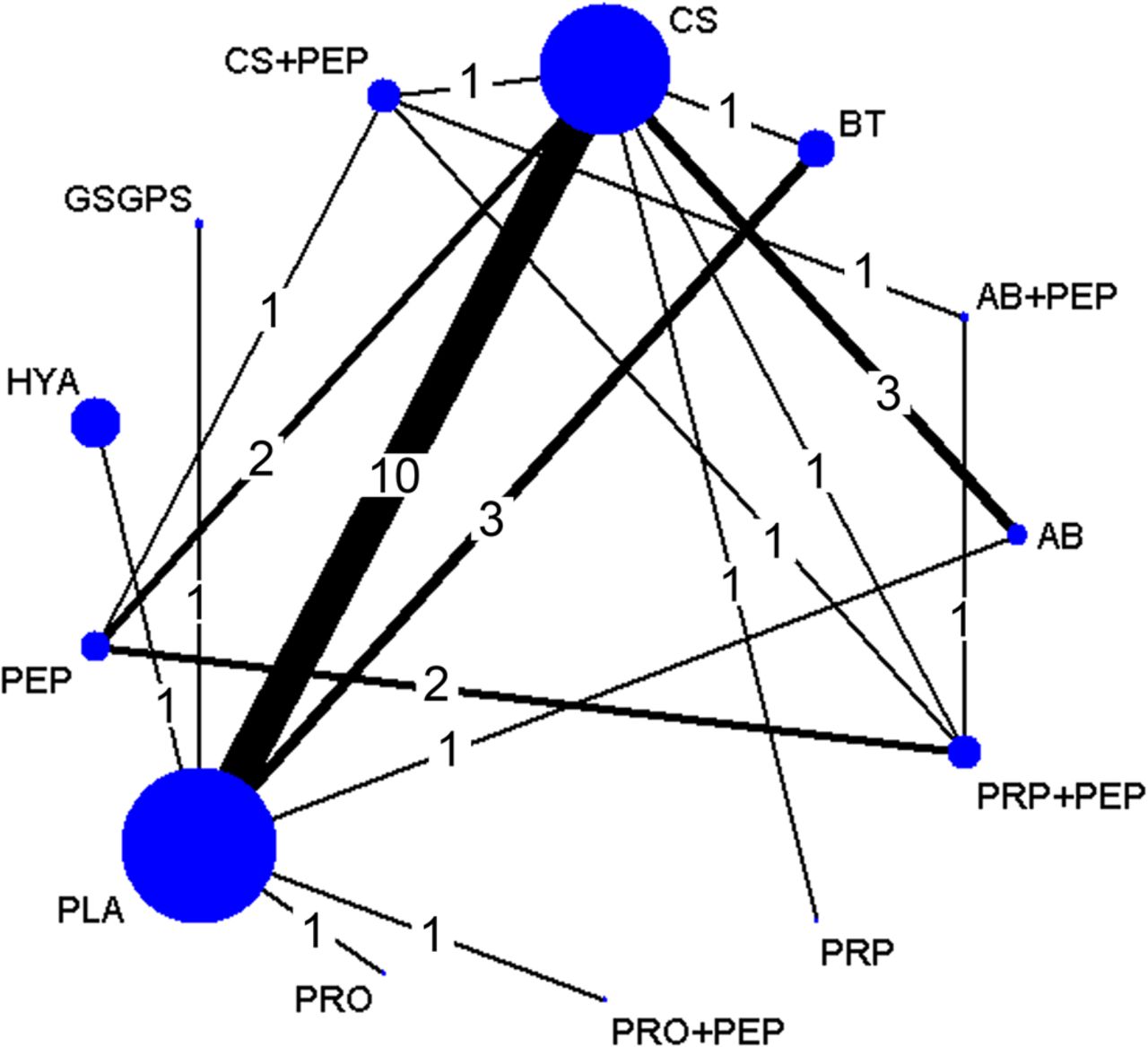
Network comparison of injection therapies for LE. Note: the size of the circle represents the number of patients; the thickness of the edge refers to the number of studies. AB, autologous blood; BT, botulinum toxin A; CS, corticosteroid; GSGPS, glycosaminoglycan polysulfate; HYA, hyaluronic acid; LE, lateral epicondylalgia; PLA, placebo; PEP, peppering technique; PRO, prolotherapy; PRP, platelet-rich plasma.
In terms of pain score, HYA showed superiority to all of the other treatments, most of which were confirmed by statistically significant differences, except for PRO. PRO, which was the second best treatment, also showed a better treatment effect than most of the other treatments, and statistically significant differences were found when it was compared with CS, PLA and CS+PEP. PRP+PEP was the third most effective treatment, but a statistically significant difference could only be found for the comparison of PRO to CS+PEP. Regarding the other treatments, PRO+PEP and AB+PEP also had better effects, while PLA, CS+PEP and PRP were the worst, but the WMDs of these comparisons all had wide 95% CIs, which did not support statistically significant differences.
Since PLA was the most commonly used treatment, the results of comparisons between PLA and other treatments were of particular concern. With regard to changes in pain score, all of the other treatments were better than PLA, but only HYA and PRO had statistically significant superiority. These results are presented in a forest plot (figure 4).
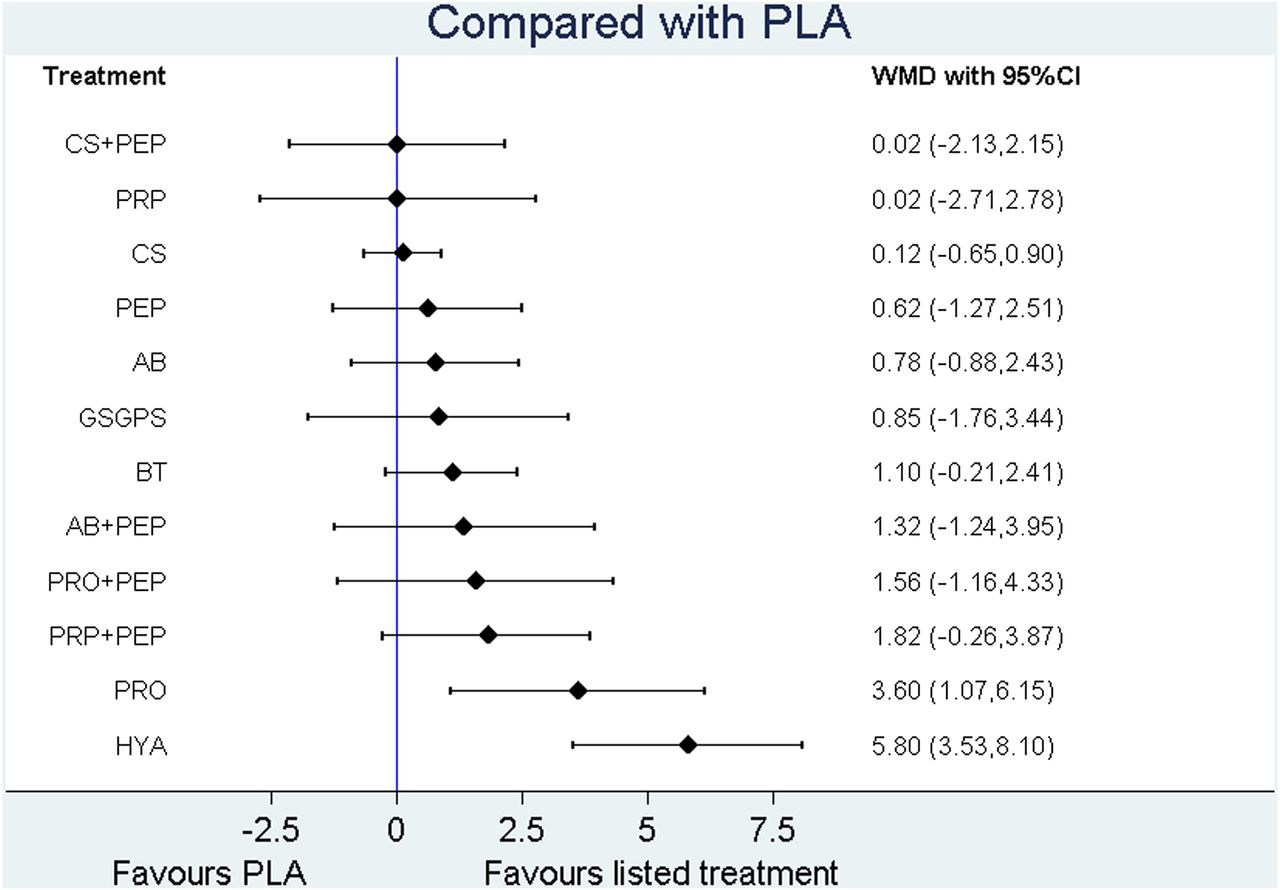
Plot of different treatments compared with PLA. AB, autologous blood; BT, botulinum toxin A; CS, corticosteroid; GSGPS, glycosaminoglycan polysulfate; HYA, hyaluronic acid; PLA, placebo; PEP, peppering technique; PRO, prolotherapy; PRP, platelet-rich plasma; WMD, weighted mean difference.
Rank probability
The rank probabilities of each treatment are presented in figure 5. For each treatment, the rank probabilities had a sum of 1. A large portion of a ‘superior rank’, such as rank 1, represented better effects, while a large portion of an ‘inferior rank’, such as rank 13, represented worse effects. The superiority to inferiority was translated into a grey scale, so the darkness of each bar represents the treatment effect, the darker the better.

Rank probability Note: (1) Different grey scales represent different ranks: rank 1 is the best, while rank 13 is the worst. (2) Each treatment has a sum of 1.0 for all of its possible rank probabilities. (3) The darkness of each bar represents the effectiveness of corresponding treatment, the darker the better. AB, autologous blood; BT, botulinum toxin A; CS, corticosteroid; GSGPS, glycosaminoglycan polysulfate; HYA, hyaluronic acid; PLA, placebo; PEP, peppering technique; PRO, prolotherapy; PRP, platelet-rich plasma.
The SUCRA plot was based on the cumulative probability of each treatment, with a large probability of ‘superior rank’ giving a high starting point to the curve. Figure 6 presents these curves and area percentages under the curves (the larger the better).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative rank probability. Note: The area under the curve represents the cumulative rank probability of each treatment (the larger the better). AB, autologous blood; BT, botulinum toxin A; CS, corticosteroid; GSGPS, glycosaminoglycan polysulfate; HYA, hyaluronic acid; PLA, placebo; PEP, peppering technique; PRO, prolotherapy; PRP, platelet-rich plasma.
Inconsistency analysis
In terms of pain score, 11 nodes were split, and the p values varied from 0.15 to 0.98, which meant that no statistically significant inconsistencies were detected.
Sensitivity analysis and metaregression
On excluding the low-quality study,27 the rank probabilities changed slightly. PRO+PEP and AB+PEP, which ranked 4 and 5, respectively, changed positions. However, the differences between them were very small in both conditions.
With metaregression, no significant difference in DIC (100.5 and 100.6) was found by taking the effects of the covariate (the sample size of the study) into consideration, and the 95% CI of the regression coefficient was −0.72 to 1.99, indicating that the covariate was not associated with the treatment effect.
Discussion
Advantages and strengths
This was the first Bayesian network meta-analysis that included all available injection treatment strategies for lateral epicondylalgia. This method overcomes the significant shortcomings of conventional meta-analysis, which cannot compare every treatment with every other treatment. Compared with a former network meta-analysis of injection treatments for lateral epicondylalgia,11 the different variances for each treatment were taken into consideration, in better conformity with the real condition. Additionally, PEP was considered as an independent treatment, so its treatment effects could be evaluated through a series of comparisons.
Only RCTs were included in our review. Although the randomisation procedures were not well described, and the blinding was insufficient in some of the studies, there was no evidence of publication bias in the quality test performed using the risk of bias tool in RevMan. Furthermore, inconsistency analysis and sensitivity analysis, as well as the metaregression, were performed to assess the reliability of the model. The outcomes of these additional procedures all support our confidence in the results.
Key clinical implications
In terms of pain score, the results for pairwise meta-analysis and network meta-analysis had good accordance, but pairwise meta-analysis found more statistical differences than network meta-analysis. In 18 pairs of comparisons with direct comparable evidence for pairwise meta-analysis, 14 of them had similar statistical interpretations for network meta-analysis. For the remaining four pairs of comparisons, statistically significant differences were all found in pairwise meta-analysis but not in network meta-analysis.
Although CS injection is the most commonly used injection therapy,43 our data suggest it is a suboptimal choice whether or not it is combined with PEP. This finding might have partly occurred because the extracted data in our review were the results of the follow-up closest to 6 months (26 weeks), which is usually considered an intermediate term. In some other systematic reviews,44 ,45 similar results were reported, but at the same time, better performance for CS injection over the short term (less than 12 weeks) was also confirmed. This finding implies that the effects of the CS might have been underestimated.
AB and PRP injections are also widely used in clinical practice. In some studies,8 ,18 ,24 ,26 ,37 these therapies were combined with PEP, which was expected to add additional benefits by providing a greater blood supply.46 In our study, AB and PRP injections, as well as the therapies derived from them, all had positive WMDs when compared with PLA, and PRP injection ranked third of all of the treatments, but there were no statistically significant differences between these injections and PLA due to wide 95% CIs. This result was also supported by some previous systematic reviews.47–50
Another common choice for injection therapy for lateral epicondylalgia is BT, which can inhibit the release of neurotransmitters at the neuromuscular junctions,51 thus relaxing the muscles and relieving pain. In a previous systematic review,52 the author reported that BT was better than PLA for lateral epicondylalgia, and this view was also supported by the pairwise meta-analysis results in our study. In network meta-analysis, although the WMD remained similar to that in the pairwise meta-analysis, the range of its 95% CI became wider and then covered the null value. This change was due to the presence of indirectly compared evidence. Hence, no statistically significant differences were found between BT and PLA.
There are also some other treatments for lateral epicondylalgia, such as hyaluronate injection, PRO and GSGPS injection. These are not very popular in clinical practice and there are few studies focused on them. However, some of them had the best treatment effects according to our review, that is, hyaluronate injection had the best effect, and PRO has the second best. Moreover, when they were compared with PLA, statistically significant differences could be observed. However, it is noteworthy that their superiority was supported only by a single study.
There was no support in our review for PEP. In the pain score network, there were four combined treatments that included PEP, and all of them had counterparts without PEP. For PRP injection and AB injection, combination with PEP could yield positive WMDs when compared with when they were used alone, but for PRO and CS injection, it seemed not to. Moreover, none of these comparisons had a 95% CI beyond the null value, indicating that no statistically significant differences could be observed.
Limitations
We discuss five limitations. First, there were many different measurements for pain score. Although these different measurements were adjusted to a 0–10 scale, ultimately some slight differences might still have existed.
Second, many comprehensive scoring systems are available for evaluating elbow function, such as the disabilities of the arm shoulder and hand (DASH)/Quick-DASH, the patient-rated tennis elbow evaluation and the patient-related forearm evaluation questionnaire, and they are used in different studies. Since they have different evaluation criteria, it is not feasible to convert them into a unified measurement by arithmetical calculation, so no comprehensive scoring system was used as a measurement in our review. These two limitations could be resolved if a general agreement on the outcome measurements for lateral epicondylalgia treatments were implemented in the future.
Third, all of the studies were classified into different treatment groups according to the substances used for injection; however, the treatment schedules and dosages varied in different studies, and these differences were ignored in our review.
Fourth, some treatments only appeared in a single study, including hyaluronate injection and PRO which showed significantly better effects, and more RCTs that focus on these treatments are expected in the future to make these results more convincing.
Fifth, the follow-up varied substantially, and although we adopted the time point that was nearest to 6 months (26 weeks), we should still be aware that this difference might affect the results. Finally, the qualities of the included studies were quite different. Some studies contained high numbers of patients with adequate randomisation, but others only had low numbers of participants or weak blinding or allocation. After enough high-quality studies are available, this limitation might be solved by a further systematic review that only contains them.
Conclusions
Our review focused on injectable treatments, which form only part of the clinician's options when treating lateral epicondylalgia.53 For patients with lateral epicondylalgia, regarding the intermediate-term effects (6 months/26 weeks), some commonly used injection therapies can be considered treatment candidates, such as BT, PRP and AB injection. CS injection is not recommended. Hyaluronate injection and PRO might be more effective, but their superiority must be confirmed by more evidence.
What are the new findings?
Hyaluronate injection and prolotherapy are the most effective treatments according to our review, but more evidence for their superiority is still needed.
Some commonly used injection therapies can be considered treatment candidates, such as botulinum toxin, platelet-rich plasma and autologous blood injection, but corticosteroid injection is not recommended.
The peppering technique might not add additional benefit to the treatment effects of injection therapies.
How might it impact on clinical practice in the future?
More attention should be paid to hyaluronate injection and prolotherapy.
The peppering technique should not be recommended.
Botulinum toxin, platelet-rich plasma and autologous blood injection are better choices than corticosteroid injection.
References
Footnotes
WD and HG contributed equally.
Contributors WD, KK, HG and CB conceived and designed the study. WD and X-BL performed the literature searches. WD, X-BL, Z-LW and F-LK performed the literature review and data extraction. WD and Z-CJ analysed the data. WD and KK wrote the first draft of the manuscript. WD, KK, HG and CP contributed to the writing of the manuscript. WD, HG, KK and KW revised the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.