Article Text

Abstract
Background Very little data on the provision of imaging services at the summer Olympic Games have been published before. With 7.9 million Euros (£6.6 million, US$11 million) invested into setting up the imaging equipment at the purpose-built polyclinics for London 2012 summer Olympics, an ideal opportunity was presented to study the demand and distribution of workload on imaging services at the games.
Setting Imaging services within polyclinics, London 2012 summer Olympic Games.
Aims To analyse the demand and distribution of workload on radiology services at the London 2012 summer Olympic Games.
Methods Data on radiological investigations performed at London 2012 summer Olympic Games were retrieved from Radiology Information System-picture archiving communication system, ATOS medical encounter database and analysed.
Results 1711 diagnostic and interventional procedures were performed at the Stratford Polyclinic within the main games village. Of these 48.8% were MRI scans, 20.2% were diagnostic ultrasound examinations, 23.6% were plain radiographs, 2.9% were CT scans and interventional procedures accounted for 4.3%. Nearly 75% of imaging was performed on athletes while less than 5% of the services were utilised by the workforce. Demand on radiology services peaked during week 2 of the games.
Conclusions Imaging played a substantial role in providing medical services at the London 2012 summer Olympics.
- Olympics
- MRI
- Ultrasound
- Sporting injuries
- Post olympic reviews
Statistics from Altmetric.com
Introduction
London 2012 summer Olympic was a memorable sporting spectacle, bringing together over 10 568 athletes from 204 different countries with around 6000 team and International Olympic Committee (IOC) officials and 70 000 volunteer workforce. Dealing with injuries and illnesses in elite athletes at any major international sporting event can be challenging, as medical needs of an athlete in competition are different from training injuries. Quick and safe return to competition, to give injured athletes the best chance of competing in what is often their only Olympic competition remains an important influence on every stage of management. It has been reported that 11–14% of athletes sustain sports injuries at major international sporting events and further 7% face constitutional illness. In total, 35–56% of the injured athletes undergo loss of time from sport.1–5 The London Organising Committee of the Olympic and Paralympic Games (LOCOG) set up medical services within the games villages to provide readily accessible medical treatment, minimising time out and inconvenience for the athletes. Limited data on imaging services at previous Olympic Games have been published previously.6 ,7 We present comprehensive demographic data including volume and distribution of workload on radiology services at the London 2012 summer Olympics. Imaging data from Paralympic games do not form part of this study.
Methods
Data on radiological investigations performed at London 2012 summer Olympic Games were prospectively collected from integrated Radiology Information System-Picture Archiving Communication System (RIS-PACS; imaging software that enables radiologists to view scan images and issue reports) and ATOS database, the official electronic games management system and analysed. Each entry was checked to exclude duplicate entries. The list of accredited athletes for the competition was obtained from IOC. Data analysis included category and modality-wise breakdown of all radiological investigations and procedures, day-wise breakdown of work load on imaging services, continent-wise breakdown of per athlete utilisation of radiology resources and referral sources at London 2012 summer Olympics.
Imaging facilities
Medical and imaging services were provided through three purpose-built polyclinics, with the major one located within the main games village at Stratford. The other two polyclinics were located at Eton Dorney, the venue for rowing and Weymouth, which was the venue for sailing competitions. The polyclinic services opened 10 days before the start of the games and continued for 2 days after the closing ceremony.
Imaging facilities at Stratford polyclinic included a digital X-ray system (GE) for plain radiography, two ultrasound (US) scanning machines (GE Logiq E9 scanners). Discovery 750 HD 64 slice multidetector CT scanner (GE Medical, Milwaukee, Wisconsin, USA), Discovery MR750w 32 channel 3T and Optima MR450w wide bore 32 channel 1.5T wide bore MRI scanners (GE Medical). The CT and MRI scanners at Stratford games village were set up within portacabins outside the polyclinic. Eton Dorney and Weymouth polyclinics were equipped with one US scanner each (GE Logiq E9). Requests for plain radiography and cross-sectional imaging at these venues were sent to designated local radiology departments under a pay as you go contract. Handheld US devices were used by the team doctors as well as LOCOG medical team at field of play and during consultation, although data on such investigations have not been included in our study.
All imaging services were offered between 7:00 and 23:00, while out-of-hours services were restricted to plain radiography accessed via polyclinic casualty. Referrals for imaging were accepted directly from team physicians who were provided with temporary registration with the General Medical Council. Referrals were also received from sports medicine doctors, casualty doctors, general practitioners (GPs), physiotherapists, podiatrists within the polyclinic and from the venue medical doctors. Referrals were made through either printed or electronic request forms providing athletes details, clinical information and nature of investigation requested. Each request was processed and entered into the RIS-PACS software electronically.
Twenty-seven musculoskeletal (MSK) radiologists, 56 radiographers, 23 radiographic assistants and four trained ultrasonographers were involved in providing radiology services at the games. All reporting MSK radiologists were FRCR trained and had at least 8 years working experience at the consultant level. The staff worked in two shifts every day, each shift lasting about 8 h. During the peak period, five MSK radiologists, five radiographers, four radiographic assistants and one ultrasonographer covered a shift. At Stratford, ultrasonographers performed non-MSK-US scans, and radiologists carried out MSK-US examinations. Radiologists conducted MSK-US scans at Eton Dorney and Weymouth at each site. A fellow in MSK radiology, sponsored by GE and Leeds Teaching Hospitals NHS Trust was based at Stratford polyclinic for the entire duration of precompetitions and competitions, involved in imaging data collection and supporting radiology services.
The turnaround time between receiving requests and performing the investigation for plain radiography and CT on an average was less than 2 h. Waiting period for MRI and US was variable. Even at peak demand, the turnaround was still on an average less than 24 h for these modalities. Printed report along with a copy of the scan images on the DVD format was issued within 1 h of the examination being performed in most cases. Conference rooms with projector facilities were available for team doctors intending to discuss the scan images with the radiologists in private. This service was in high demand from the team physicians and contributed positively towards making key decisions over athletes’ medical management postinjury.
Statistics
Data are presented as frequencies and proportions. Numerical data, except for resource utilisation per athlete, have been rounded off to nearest one decimal. Given the extremely small values, resource utilisation per athlete was worked up to the nearest third decimal for greater accuracy.
Results
Imaging at Stratford polyclinic within the main games village
Volume of workload handled
A total of 1711 radiological investigations and interventional procedures were performed at the Stratford polyclinic. See table 1 for individual modality breakdown.
Breakdown of all radiological investigations performed at Stratford Polyclinic, based on modality
Of the 1711 investigations, 1283 (75%) investigations were performed on athletes, 347 (20.3%) on team and IOC officials and 81 (4.7%) investigations were performed on the volunteer workforce (table 2; figure 1).
Breakdown of all radiological investigations at Stratford Polyclinic, based on modality and category

Percentage breakdown of radiological investigations.
Radiological investigations in athletes
In total, 1283 radiological investigations were performed on 825 athletes, of which over 35% of the investigations were performed on track and field athletes. The next highest number of investigations was performed in Hockey (6.2%), closely followed by handball, basketball, judo and weightlifting (table 3).
Distribution of radiological investigations on athletes at Stratford polyclinic, based on sport
Of the 825 athletes imaged, 430 (52.1%) were men and 395 (47.9%) were women. Given that 5892 (55.8%) of the total athlete population were men and 4675 (44.2%) women, only marginal variation in ratio of imaged to total athletes is observed for each gender. This ratio is 0.13 for female athletes as compared with 0.11 for male athletes. Age-wise breakdown of investigations in athletes is shown in figure 2.
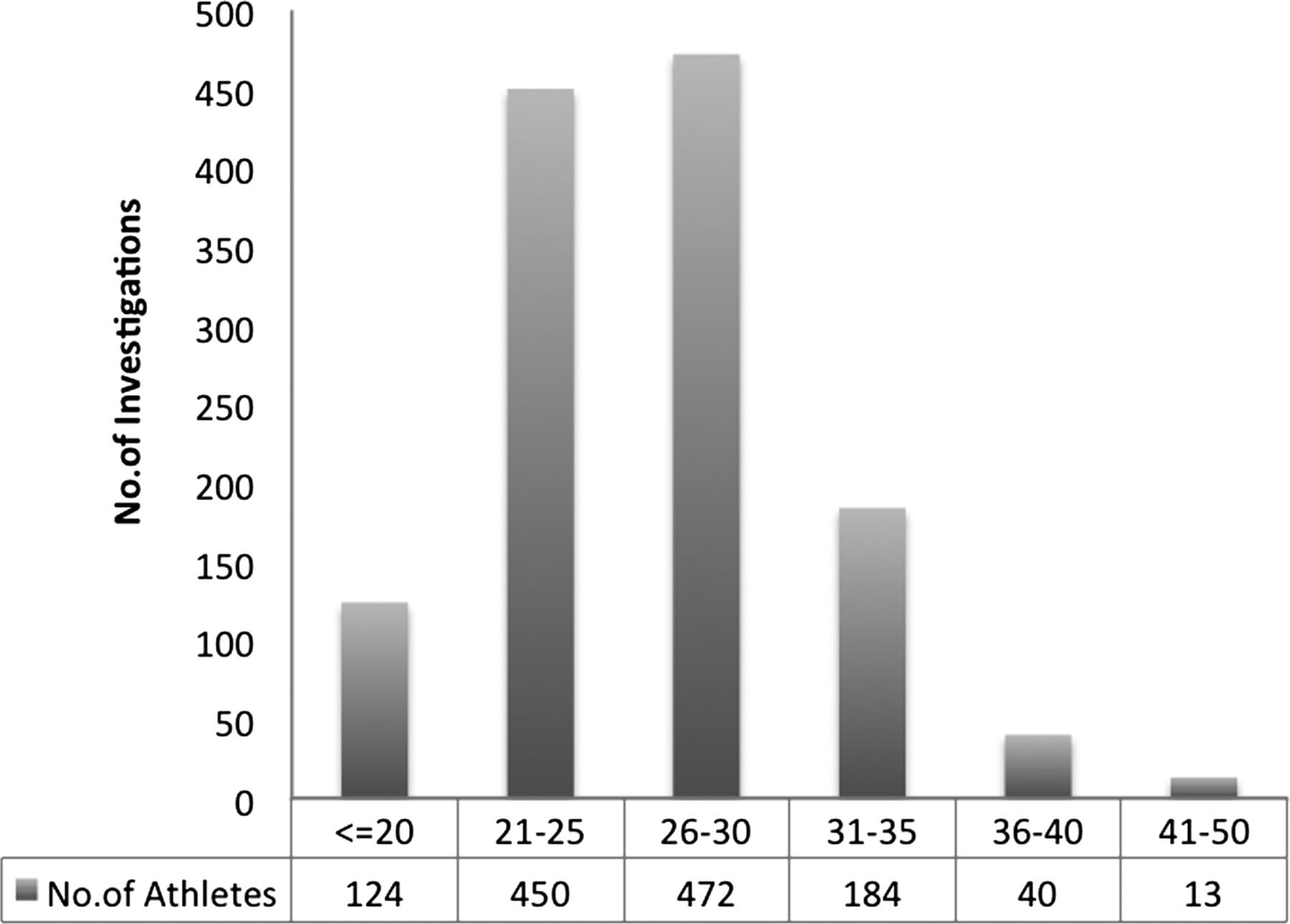
Distribution of radiological investigations based on age.
Distribution of workload at various stages of the competition
Imaging services were busiest during the second week of the competitions, when the games schedule was at its busiest with the maximal number of residents within the games village (table 4; figure 3). The workload started gently decreasing during the past few of days of service. In total, 81.4% of all investigations were performed during the actual competition and 18.2% precompetition. Limited services were provided for 2 days following the games, during which only seven (0.4%) investigations were performed selectively in cases where there was an element of urgency.
Breakdown of all radiological investigations performed during each day of the competitions

Line graph demonstrating the total number of investigations performed (all categories) on a weekly basis between 16 July 2012 and 12 August 2012 covering both precompetition and competition periods. The postcompetition days (13–14 August) have not been plotted, as the polyclinic was partially functional during this time and only seven examinations were performed in these 2 days.
Breakdown of investigation modalities
MRI
Of the 674 (66%) MRIs performed on athletes, 445 were on lower extremity, majority of which were knees, 112 (16.6%) on upper extremity and 104 (15.4%) were performed on spine (table 5). One MRCP for suspected biliary pathology, three MRI brains following head injuries were among other scans performed on athletes. Within team officials’ category, about 80% of the MRIs performed were on knees, spines and shoulders.
Summary of MRI procedures based on body area scanned
MRI was performed as a second-line investigation to US in 40 athletes. MRI demonstrated pathology in five cases where US was normal. Three of these were labral tears in hip and shoulder and the rest included subtle muscle tear and tear of the anterior talo-fibular ligament within the ankle joint, which was difficult to appreciate on US due to extensive soft-tissue swelling and joint effusion.
MR arthrography was hardly ever requested during the games. Acute traumatic dislocation of shoulders presented with joint effusion, which provided for adequate joint distension. Besides high-resolution images from 3T MRI to an extent reduced the need for arthrographic examinations of the joints.8 Gadolinium-enhanced MRI had to be used in only two cases for the entire duration of the games.
Diagnostic US
A total of 347 diagnostic US examinations were performed on athletes, team officials and workforce combined, of which 284 (81.8%) were MSK and 63 (18.2%) were non-MSK/general examinations (table 6). The majority of the MSK-USs performed on athletes (66.9%) were for lower limb problems, while a much smaller percentage of scans performed on upper extremities (17.1%). Sonographic evaluation of Achilles tendon, ankles for ligament injuries and foot for evaluation of plantar fascia made up for a significant proportion of scans performed. Abdominal and pelvic US in athletes’ category and US for suspected deep vein thrombosis in the team officials’ category were the most commonly performed general US investigations. Torted ovary in an athlete requiring partial oophorectomy was among the acute emergencies diagnosed on US.
Diagnostic US procedures breakdown
Diagnostic CT
Fifty diagnostic CTs were performed in total, 42 of which were performed on athletes (table 7). Seventeen of the diagnostic CTs were performed as second-line investigations following MRI examinations in athletes. Thirteen of these were to evaluate stress fractures, suspected on MRI and 12 of these were positive on CT. The other indication for performing CT following MRI was to confirm avulsion fractures suspected on MRI.
Diagnostic CT procedures breakdown
Plain radiography
Of the total 405 plain radiographic examinations, 252 (62.2%) were performed on athletes (table 8). Plain X-ray of the foot was the most commonly requested investigation among athletes, accounting for 31 (12.3%) examinations. X-rays of knees (21.3%) were performed in highest number, followed by chest X-rays (17.6%) within the team officials’ category. Plain radiographs performed on workforce accounted for 11.1% of all plain X-ray examinations performed. This figure is considerably higher in comparison to other modalities (1.7% for MRI and 5.2% for US), suggesting that plain films were more utilised for imaging workforce.
Plain films breakdown
Imaging-guided intervention
Imaging-guided interventional procedures were carried out following clinico-radiological discussion of the athletes’ medical problem. This was in most cases preceded by diagnostic evaluation of the affected body part. A total of 74 imaging-guided interventional procedures were performed (tables 9 and 10). Most of the imaging-guided injections in extremities were performed under US guidance, while spinal intervention was exclusively performed under CT guidance.
CT-guided procedures breakdown
Ultrasound-guided procedures breakdown
Within upper extremity, US-guided intrabursal injection of shoulder was the most commonly performed procedure, while local anaesthetic and corticosteroid injections for indications such as tendinopathy, tenosynovitis were most commonly performed procedures on the lower extremities. Platelet-rich plasma, dextrose injections and intra-articular hyaluronic acid injections were among the interventional procedures performed under US guidance. No direct complications following interventional procedures were reported during the games.
Referral sources
Majority of the referrals for imaging in both athletes and team officials were received from National Olympic Committee (NOC) team doctors, accounting for 62% and 49% of the referrals, respectively. Seventeen per cent of imaging referrals within team officials’ category originated from GPs as compared with 0.6% in athletes, which suggests that general medical illnesses were more commonly encountered in this group. Within workforce category, most of the imaging referrals came through casualty doctors and GPs, accounting for 82% of referrals in this group.
Imaging at Eton Dorney and Weymouth
Compared with Stratford, far less imaging was handled at other sites, due to fewer sporting events and competing athletes. Forty-seven US examinations were performed at Weymouth polyclinic, of which 22 (46.8%) were performed on athletes, 20 (42.6%) on workforce and 5 (10.6%) on team officials. At Eton Dorney 18 US examinations were performed in total, of which 14 (78%) were on workforce and a mere 4 (22%) examinations were on actual athletes. Significantly a higher percentage of scans was performed on workforce at both Weymouth and Eton Dorney sites, compared with the Stratford.
Continent-wise breakdown of radiological investigations and resource utilisation per athlete
Resource utilisation per registered athlete at the games was highest for Africa at 0.294 as compared with an overall average of 0.169 (figure 4). Notably, about 70% of all examinations performed on African athletes were on the lower extremities and nearly 50% of those scanned competed in track and field events. About 50% of all radiological procedures performed in this group were MRI scans. Given that only four athletes represented Independent Olympic Athletes and only one radiological investigation performed, not much can be deduced in this category.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall resource utilisation per athlete based on the continent.
Discussion
Imaging was well utilised by the athletes throughout the games. US was used for diagnosing muscle tears and injuries to superficial tendons, ligaments and plantar fascia. MRI was used for diagnosing subtle muscle tear which was difficult to visualise on US and for defining complete extent and morphology of high-grade muscle tears. Suspected pathology to soft tissue such as menisci, labrum, deep tendons and ligaments, spine, sacroiliac joints and anatomical areas difficult to assess on US were also investigated with MRI. MRI was performed as second-line investigation to US in few cases, for further evaluation of pathology identified on US or when US findings were inconclusive. MSK-US accounted for 80% of all US examinations performed at London summer Olympics, as compared with only 30% in Beijing.
The incidence of stress fractures in track and field athletes alone is 21.1%, with majority occurring within the tibia.9 CT is useful in diagnosing bone stress fractures9–11 and served as a second-line investigation for evaluation of bone stress response seen on MRI. Diagnosing such injuries with accuracy gave athletes better information on true extent of risk involved in competing with the injury, thereby helping them make better informed choices. Avulsion fractures difficult to appreciate on plain films were also diagnosed on CT.
The major indication for plain film imaging in athletes was to exclude fractures following acute trauma, although a significant number of chest and knee radiographs were performed, particularly in team officials’ category, for general illnesses and chronic pain, respectively.
Injuries to lower extremities were more commonly imaged than any other body part, accounting for nearly 66% of all MRIs and USs performed in athletes. This matches the results from previous studies on injury surveillance conducted on elite athletes at major international sporting events.3 ,5 ,12 ,13 Nearly 35% of imaging performed on athletes was in track and field category. Our data on sport-wise breakdown of imaging in athletes (table 3) match the distribution of injuries in various sports reported at Beijing 2008.2
Events and schedules on the day influenced the nature of requests for radiological investigations. This is based on the fact that sport-specific injuries occurred more commonly on days such events were being held in the sporting arena. For example, elbow injuries, peaked during judo and weightlifting events, the two Olympic sports most commonly prone for elbow injuries. Similarly the bulk of the imaging requests for suspected plantar fascia, Achilles tendon pathology and muscle tears within lower limbs coincided with the period when track and field events were scheduled.
Continent-wise breakdown of utilisation of radiology resources suggest that Africa has the highest ratio of per athlete consumption of imaging resources. If similar trends are observed consistently and lack of access to adequate imaging facilities is an attributing factor, this information should be fed back to the respective NOCs for review of existing medical infrastructure and access to imaging facilities.
Limitations
While all efforts were made to ensure accuracy, the manual entry of radiological investigation type on the RIS system makes this liable for an element of human error. Team Officials category includes investigations performed on both team and IOC officials. It was a deliberate attempt not to classify these groups as this was interchangeably used during entry into the ATOS and RIS systems and hence classification could invite an element of error.
Access to information on imaging services offered at field of play, participating teams’ medical set-ups and imaging performed outside the polyclinics was not available on the ATOS medical encounter system and hence not included.
Conclusion
The demand for MRI services, which accounted for nearly 50% of all radiological examinations, justified setting up two MRI scanners within the main games village polyclinic. Despite having two MRI scanners and two US units within the main games village, demand for these services was continuous and at times extremely busy. Both US-guided extremity and CT-guided spinal intervention were in demand from the athletes and having such facilities on site can contribute to quick and effective management of athletes medical problems, where indicated. Recording use of portable US imaging on field and during consultation by sports physicians as separate investigations into the main ATOS medical encounter system at future events can provide easy access to this information. Such information can contribute positively towards data analysis.
What are the new findings?
-
Breakdown of imaging demographic data and volume of workload on radiology services at various stages of 2012 summer Olympics.
-
Use of imaging services including diagnostic and interventional procedures by athletes, team officials and work force.
-
Per athlete utilisation of imaging resources based on the continent.
How might it impact on clinical practice in the near future?
-
The data are a guide for anticipating demand on imaging services and when used in conjunction with the existing injury and illness surveillance data, serve useful lessons towards planning imaging infrastructure tailored to the needs and demands of the events at similar international sporting events.
Acknowledgments
Mr Torbjørn Soligard, Medical & Scientific Department, IOC for official data on registered athletes at London 2012 summer Olympics.
References
Footnotes
-
Contributors SB participated in conception and design, analysis and interpretation of data and drafting the article. RB and LE participated in conception and design; revising it critically for important intellectual content. POC is the guarantor, participated in conception and design; revisingit critically for important intellectual content.
-
Funding GE, sponsor at the Olympic Games, cofunded with Leeds Teaching Hospitals an imaging fellow (FRCR qualified radiologist), who was responsible for data collection and analysis at the games.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com