Article Text

Abstract
Background Ankle injury is common in football, but the circumstances surrounding them are not well characterised.
Aim To investigate the rates, especially time-trends, and circumstances of ankle injuries in male professional football.
Methods 27 European clubs with 1743 players were followed prospectively between 2001/2002 and 2011/2012. Time loss injuries and individual-player exposure during training sessions and matches were recorded. Injury rate was defined as the number of injuries/1000 h.
Results A total of 1080 ankle injuries were recorded (13% of all injuries) with lateral ligament ankle sprain being the most common injury subtype (51% of all ankle injuries). The rates of ankle injury and ankle sprain were 1/1000 h and 0.7/1000 h, respectively. The ankle sprain rate declined slightly over time during the 11-year study period (on average 3.1%/season) with a statistically significant seasonal trend (p=0.041). Foul play according to the referee was involved in 40% of the match-related ankle sprains. Syndesmotic sprains and ankle impingement were uncommon causes of time loss (3% each of all ankle injuries).
Conclusions Lateral ligament ankle sprain constituted half of all ankle injuries in male professional football, whereas ankle impingement syndromes were uncommon. The ankle sprain rate decreased slightly over time, but many ankle sprains were associated with foul play. Our data extend the body of literature that provides football policy makers with a foundation to review existing rules and their enforcement.
Statistics from Altmetric.com
Introduction
Ankle injuries account for 10–18% of all injuries in high-level football.1–8 Sprains constitute between 51% and 81% of all ankle injuries in these studies, and more than three-quarter of the ankle sprains affect the lateral ligaments.2 ,4 Many ankle sprains occur as a result of player contact,9–11 often with tackling and foul play involved,9 ,10 and a common football-specific injury mechanism with direct impact on the medial aspect of the lower leg by an opponent tackling before or at foot strike resulting in a forced inversion of the ankle joint has been described.10
The epidemiology of ankle sprains in football is fairly well described, but knowledge about other ankle injuries, such as fractures and impingement, on the overall injury burden and player availability is scarce. Previous studies suggest that the ankle sprain rate is lower nowadays than during the 1980s and 1990s,5 ,6 ,12–16 but long-term prospective studies that have investigated the development of ankle injuries over time are lacking. We investigated the rates, especially time-trends, and circumstances of ankle injuries in male professional football in Europe over 11 consecutive seasons.
Materials and methods
The current survey is a substudy of a prospective cohort study evaluating male professional football in Europe in collaboration with the Union of European Football Associations.8 A total of 27 clubs from 10 countries with 1743 players (a mean squad size of 28 players were followed over a varying number of seasons from 2001 to 2012 (160 club-seasons and 4375 player-seasons were included for analysis).17 The studied seasons were divided into preseason (July and August) and competitive season (September–May). The study design adheres to the consensus statement on injury definitions and data collection procedures in football,18 and the general methodology has been reported elsewhere.19 Supplementary online-only files 1 and 2 show the study design and the forms used and also the manual with practical instructions.
Inclusion criteria and definitions
All players belonging to the first team squads in each season were eligible for inclusion. Players who were transferred to other clubs or finished their contracts due to other reasons before the end of a season were included for as long as they participated. Injury was defined according to time loss (table 1), and players were considered injured until the club medical staff allowed full participation in training and availability for match selection.18 ,19 For the purpose of this study, the ankle (talocrural) region included the tibiotalar and the inferior tibiofibular joints as well as the surrounding stabilising connective soft tissue (ie, joint capsules and ligaments) of these joints and the overlying skin. Achilles tendon pathology was classified as lower leg injuries18 and, similarly, the pathology of other tendons passing from the lower leg to the foot was classified by the study group as lower leg or foot injuries depending on the injury location. Ankle sprains were classified as capsular, lateral (anterior talofibular, calcaneofibular and posterior talofibular ligaments), medial (deltoid ligament) and high (tibiofibular syndesmosis). Reinjuries were defined according to the concept of early recurrences.18
Operational definitions used in study
Data collection
A member of the medical or coaching staff registered individual player exposure in minutes during all club (first team, second team or youth team) and national team training sessions and matches. All injuries were recorded immediately after the event by a club medical officer. Injury cards and attendance records were sent to the study group once a month. The injury card was slightly modified during the study period in that all injuries had to be classified as contact or non-contact injuries starting from the 2004/2005 season and the minute of injury was recorded for all match injuries from the 2005/2006 season. Each injury was coded according to a modified version of the Orchard Sports Injury Classification System V.2.0.20
Statistical analyses
Continuous data for anthropometrics were presented as the mean with corresponding SD, and lay-off times were presented as both mean±SD and median with corresponding IQR. Injury rate (IR) was calculated as the number of injuries per 1000 h with corresponding 95% CI. Injury burden was calculated as the number of lay-off days per 1000 h. IRs were compared using a rate ratio (RR) and significance tested with z-statistics.21 The seasonal trend for ankle injuries in general and ankle sprains, expressed as the average annual percentage of change, was analysed using linear regression with log-transformed IRs as a dependent variable. A 2-year moving average (MA) approach, by summarising two consecutive seasons, was also used to smooth out large seasonal variation. Owing to a skewed distribution, differences in lay-off times were analysed using the Mann-Whitney U test for reinjuries and the Kruskal-Wallis test for ankle sprain categories. Injury occurrence between the six 15 min periods of a match was analysed using the one-sample proportional z test. All analyses were two-sided and the significance level was set at p<0.05.
Results
A total of 8029 injuries were recorded during 1 057 201 exposure hours (888 249 training and 168 952 match). There were 1080 ankle injuries (427 training and 653 match), thus constituting 13% of all injuries. The overall ankle IR was 1/1000 h (table 2), which means that a professional football club with a 25-player squad will suffer around seven ankle injuries in each season. Ankle sprain was the single most common injury type (table 2), constituting 68% of all ankle injuries and 9% of all injuries. The overall ankle sprain rate was 0.7/1000 h (table 2), and a professional 25-player squad will thus suffer an average of four to five ankle sprains in each season. The MA approach indicated an average annual IR decrease of 1.7% for ankle injuries in general, but the seasonal trend in the regression model was not significant (R2=0.12, b=−0.011, 95% CI −0.034 to 0.012, p=0.30). Similarly, an average annual IR decrease of 3.1% for ankle sprains was indicated in the MA approach (figure 1), with a statistically significant seasonal trend in the regression model (R2=0.39, b=−0.030, 95% CI −0.059 to −0.002, p=0.041).
Frequency, injury rate and injury recurrence of all ankle injury types in male professional football
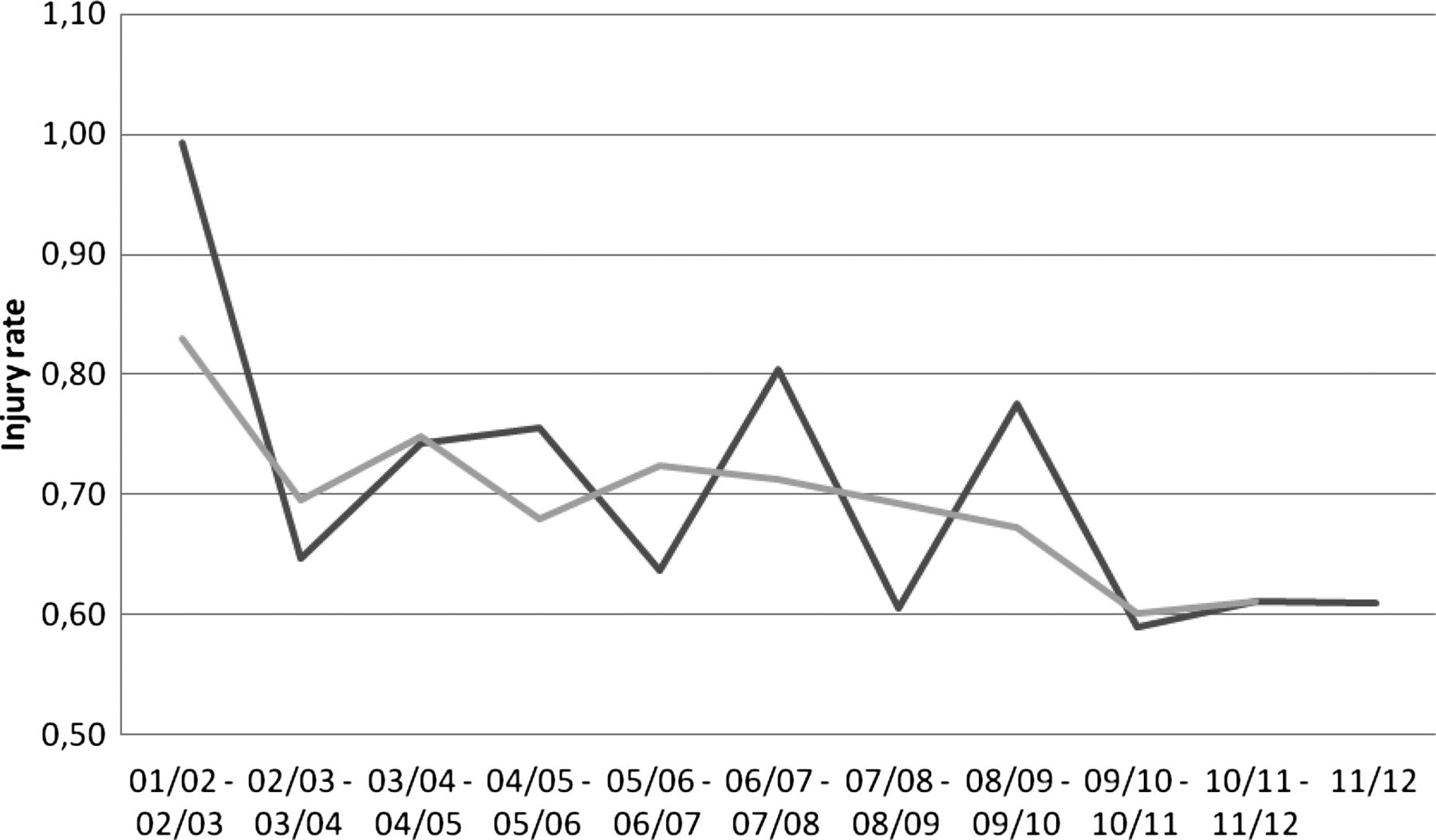
Injury rates for ankle sprain per season. Injury rate is expressed as the number of injuries per 1000 h. The dark grey line shows the 2-year moving average injury rate calculated as the sum of two consecutive seasons.
When comparing preseason and competitive season (figure 2), there were no statistically significant differences in ankle IRs during training (0.51/1000 h vs 0.48/1000 h, RR 1.06, 95% CI 0.84 to 1.34, p=0.60) or match play (4.13/1000 h vs 3.81/1000 h, RR 1.08, 95% CI 0.88 to 1.33, p=0.45), as well as in ankle sprain rates during training (0.34/1000 h vs 0.33/1000 h, RR 1.05, 95% CI 0.79 to 1.38, p=0.76) or match play (2.86/1000 h vs 2.53/1000 h, RR 1.13, 95% CI 0.87 to 1.45, p=0.32).

Seasonal distribution of injury rates in male professional football. Injury rate is expressed as the number of injuries per 1000 h.
Three-quarter of the sprains affected the lateral ligaments, whereas only 5% were high syndesmotic injuries (table 2). More sprains occurred to the dominant leg (542/729), and the differences in IRs between the dominant and non-dominant ankles were statistically significant (0.51/1000 h vs 0.18/1000 h, RR 2.90, 95% CI 2.45 to 3.42, p<0.0001). The IRs for the different sprain categories were between 3 and 10 times higher during match play compared with training (table 3).
Match and training injury rates for the most common ankle injury types in male professional football with corresponding rate ratios
Second to joint and ligament injuries, contusions were most common and constituted approximately every sixth ankle injury, whereas only 18 fractures were reported (table 2). Ankle impingement syndromes were uncommon causes of time loss (table 2). The rate of posterior impingement was more than threefold higher than that of anterior impingement (0.024/1000 h vs 0.007/1000 h, RR 3.57, 95% CI 1.54 to 8.26, p=0.003). Most of the impingement syndromes affected the dominant ankle (5/7 in anterior and 16/25 in posterior).
Injury circumstances
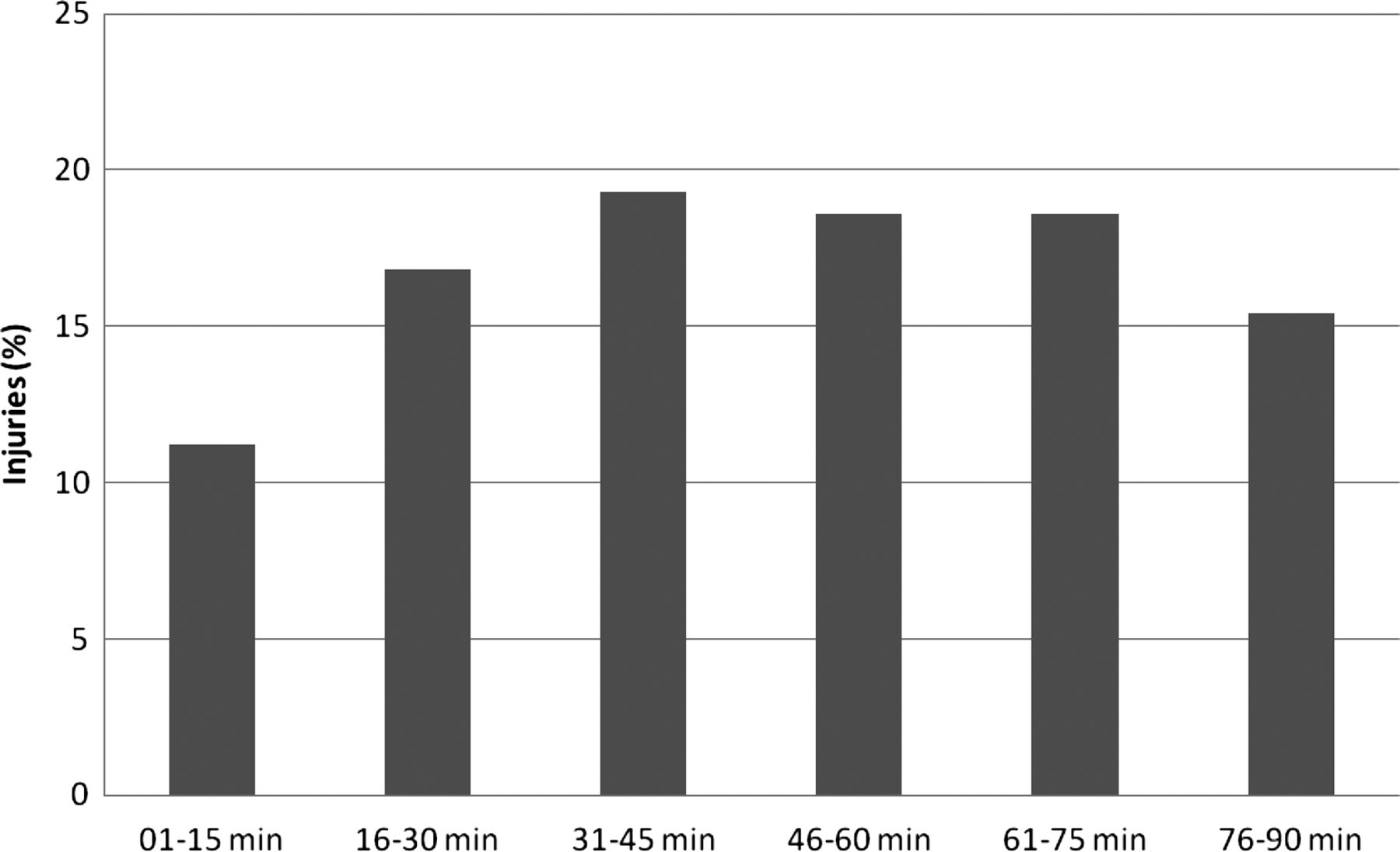
From season 2004/2005 and forward, 566 ankle sprains were classified according to contact or non-contact (six cases missing), with more than half of them being the result of player contact (58%). Foul play (own or opponent) was involved in 40% of the match-related ankle sprains, but few of these fouls were sanctioned with a yellow or red card (5.8%). Additionally, the minute of injury was reported for 285 ankle sprains occurring during match play from season 2005/2006 and forward (35 cases missing). Significantly fewer ankle sprains than expected occurred during the first 15 min of the first half (11.2% vs 16.7%, p=0.014), whereas no significant differences were detected for the rest of the 15 min periods (figure 3).

{kind=link}
{kind=link}
{kind=link}
Proportion of ankle sprains during the 15 min periods of match play in male professional football.
Injury severity
In total, 13% of the ankle injuries were severe (table 4). The average lay-off per ankle injury was 16±27 (median 8, IQR 15) days with the injury burden completely dominated by lateral ligament sprain (table 4). High ankle sprains had an average lay-off of 43±33 (median 34, IQR 37) days and this was significantly longer than the other three ankle sprain categories (p<0.0001). Finally, there were three avulsion fractures of the lateral malleolus causing a lay-off between 6 and 15 days, whereas all other ankle fractures were severe with an average lay-off of 103±45 (median 93, IQR 50) days.
Severity, lay-off and injury burden for the most common ankle injury types in male professional football
Reinjuries
In total, 11% of all ankle injuries and 10% of ankle sprains were classified as reinjuries (table 2). No significant difference in average lay-off was seen between recurrent sprains and other sprains (15±19 (median 9, IQR 13) vs 15±21 (median 8, IQR 15 days), p=0.87).
Discussion
The principal finding of this study was that 40% of the match-related ankle sprains occurred as a result of foul play. Other important findings were that almost every 10th football injury was an ankle sprain and that the ankle sprain rate showed a statistically significant decreasing trend over the 11-season study period. Finally, ankle impingement was an uncommon cause of time loss during the seasons studied, especially the anterior impingement.
Ankle injury epidemiology
In a large-scale review of 227 studies on 70 different sports22 football was a high-risk sport for ankle injury, particularly ankle sprain. We found that 68% of all ankle injuries were sprains and this finding extends the previous literature.1–8 Historically, ankle sprain used to be the most common football injury and studies from male high-level football conducted during the 1980s and 1990s reported overall ankle sprain rates as 1.8/1000 h and 1.3/1000 h, respectively.12 ,13 In more recent studies conducted from 1999 and later, however, the ankle sprain rate has been considerably lower (0.5–0.8/1000 h).5 ,6 ,14–16 The overall ankle sprain rate in the current study was 0.7/1000 h, and it thus seems that the current ankle sprain rate is lower than that historically attributed. Interestingly, there was a trend of a further decline over time with an average annual decrease in the ankle sprain rate of 3%.
The most plausible explanation to the lower ankle sprain rate nowadays and the declining trend is successful implementation of strategies in the clubs such as balance board training and taping/bracing for preventing recurrent ankle sprains,23–26 although no such player data were collected in this study. Another contributing factor could be that more training now than before is devoted to ‘low-risk’ activities such as recovery sessions, resistance training and physical conditioning, making the overall ankle sprain rates lower.
Foul play was involved in 40% of the match play ankle sprains. This finding is in line with the results in a previous systematic video analysis study of Norwegian and Icelandic elite football where many ankle sprains were shown to result from late tackles, sometimes even intentional fouls, without penalty to the offending player.10 We therefore call for stricter enforcement of the existing rules or introduction of new rules such as timed suspensions to be able to prevent these frequent contact-related injuries that theoretically would be very difficult to prevent with balance training or ankle support.
Ankle sprain frequency at different stages of matches
In two studies on male professional and amateur football, ankle sprains were more frequent in the last thirds of both halves,4 ,11 without formal statistics, whereas no such trend was detected in the current study.
No worries for footballer's ankle?
Although given increasing attention in recent years,27 ,28 anterior and posterior ankle impingement syndromes were quite infrequent in this study and constituted only 3% of all ankle injuries. Considering that anterior ankle impingement historically was called ‘footballer's ankle’,29 ,30 the posterior impingement rate was, somewhat surprisingly, more than threefold higher in the current study. The problem with ankle impingement is, however, most probably underestimated due to the use of a time loss injury definition,31 and players might be able to play despite their symptoms and are perhaps not referred to definitive treatment until the season is over. As only 4 of the 32 impingement injuries in the current study were categorised as severe, most of them were obviously managed non-surgically in this setting.
Interestingly, almost two-thirds of the impingements occurred to the preferred kicking leg (dominant ankle) in the current study. It has previously been shown that a typical ankle injury mechanism in football is a forced plantar flexion where the injured player hit an opponent's foot when attempting to shoot or clear the ball, and this anterior capsular traction mechanism was suggested to contribute to the development of ‘footballer's ankle’.10 However, since the anterior joint capsule attachments are more proximal and distal to the sites where the talotibial spurs originate, this theory has been questioned.30 It is noteworthy that a forced plantar flexion not only leads to an anterior traction force, but also to a forceful compression of the bony and soft tissues on the posterior part of the ankle.27 Thus, the previously described injury mechanism for ‘footballer's ankle’ could therefore be a more common cause of posterior ankle impingement. This notion is supported by the fact that posterior impingement was significantly more common in the current study than anterior impingement.
Injury severity
In total, 87% of the ankle sprains had a lay-off of less than 4 weeks, which is in line with a recent study from Swedish elite football where this figure was 83%.7 The mean lay-off per ankle sprain was, however, 15 days in the current study compared with only 8 days in that study. This apparent discrepancy could possibly reflect a ‘better safe than quick’ treatment algorithm that is supported by the fact that the ankle sprain reinjury frequency was low (10%).
Interestingly, almost two-thirds of the high ankle sprains were severe and these injuries were associated with a substantially longer lay-off than both the lateral and medial ligament sprains. The athletic literature in this field is scarce, but in a review of 1344 ankle sprains occurring in West Point cadets, only 10 high ankle sprains were identified, but, in line with the current study, these injuries required a considerably longer time to return to full activity compared with grade III lateral ligament sprains (mean 55 vs 28 days).32
Methodological considerations
The prospective design with rigorous data check-up and the 11-season study period to avoid the influence of occasional extreme seasons are some important strengths of the present study together with the large and homogeneous sample of professional footballers. However, this study also has some important limitations. First, no treatment details were requested on the general injury card, and additionally, no substudy specific injury card was sent to the clubs as for some of our previous substudies.33 ,34 It would have been interesting to collect surgical data for the ankle fractures and impingement syndromes, but it would probably be of minor value for ankle sprains since the need for ligament surgery in professional football has been shown to be minimal.4 Second, no information about the use of any preventive training such as balance board training and coach-directed limitation of player-contact during training sessions or the use of any protective equipment such as bracing and taping was recorded, and these aspects therefore need to be addressed in future studies. Third, only one diagnosis was recorded for each injury case in the database (the main diagnosis). In cases with multiple injuries sustained in the same event (eg, a severe ankle ligament sprain with concomitant mild cartilage abnormalities on imaging), only the most significant injury is captured in the injury surveillance. Fourth, all tendon injuries were excluded from the definition of ankle injury, and it could be argued that, for example, posterior tibial and peroneal tendon injuries located posterior to the malleoli should be included among the ankle injuries. The exact location of the tendon pathology was, however, not requested on the injury card and the tendon injuries were therefore excluded from the ankle injury definition. Fifth, the participating clubs were not provided with any specific diagnostic or return-to-play criteria in our study manual, and it is therefore possible that the reported subclassifications, lay-off times and reinjury frequency varied between clubs due to the different diagnostics and treatment algorithms. Sixth, no reliable history of previous injury was collected at player inclusion, and it was therefore not possible to compare the ankle sprain rates between uninjured players and players with prior ankle sprain. It is, however, well known that players with previous ankle sprain during the career or the preceding season have approximately 2–3 times higher rate of future ankle sprain.12–15 Finally, the design of the injury card during the first seasons of the study did not include information about the match minute of the injury and whether it resulted from contact or not.
Clinical and policy implications—call for action
In conclusion, lateral ligament ankle sprains constituted half of all ankle injuries in male professional football, whereas the anterior and posterior ankle impingement syndromes were infrequent. The ankle sprain rate showed a statistically significant decreasing trend over the 11-season study period, and although the reasons for this cannot be ascertained from our study design, it is consistent with a decreasing trend for ligament injuries in general.17 Many match-related ankle sprains were, however, associated with foul play and this finding might warrant a discussion in the international governing bodies about stricter rule enforcement.
What this study adds
-
The ankle sprain rate in male professional football has decreased significantly over the past decade.
-
Foul play was involved in more than half of the ankle sprains associated with player contact.
-
Ankle impingement syndromes, especially the anterior ‘footballer's ankle’, were uncommon causes of time loss.
How might it impact on clinical practice?
Ankle sprains are common and constitute more than half of all ankle injuries in professional football. The decreasing trend in the ankle sprain rate since 2001/2002, as shown in this study, gives indirect evidence that injury prevention strategies have been successful. These findings might therefore serve as a motivator among players, coaches, medical practitioners and stakeholders for continuous preventive efforts in the sport.
Acknowledgments
The authors would like to thank the participating clubs (coaching and technical staff, medical teams and players) for their participation in the study. Henrik Magnusson, MSc, is also acknowledged for statistical advice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
-
Contributors MW, MH and JE were responsible for the conception and design of the study. All authors have been involved in the data collection over the study period. MW and the statistical advisor conducted the analyses which were planned and checked with the coauthors. All authors contributed to the interpretation of findings and had full access to all data. MW wrote the first draft of the paper which was critically revised by MH and JE. The final manuscript has been approved by all authors. MW is the study guarantor.
-
Funding This study was funded by grants from the Union of European Football Associations (UEFA), Swedish National Centre for Research in Sports, and Praktikertjänst AB.
-
Competing interests JE is the first vice chairman of the UEFA Medical Committee.
-
Ethics approval The study design was approved by the UEFA Medical Committee and the UEFA Football Development Division.
-
Provenance and peer review Not commissioned; externally reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com