Article Text

Abstract
Aim To analyse aerobic fitness and its relationship with sport participation, exercise training and habitual physical activity (HPA) during youth.
Methods Studies were located through computer searches of Medline, SPORT Discus and personal databases. Systematic reviews of time trends in aerobic fitness/performance, and exercise training and peak oxygen uptake (peak VO2) are reported.
Results Peak VO2 increases with age and maturation. Boys' peak VO2 is higher than girls'. Despite data showing a decrease in performance test estimates of aerobic fitness there is no compelling evidence to suggest that young people have low levels of peak VO2 or that it is declining over time. The primary time constant of the VO2 kinetics response to moderate and heavy intensity exercise slows with age and the VO2 kinetics response to heavy intensity exercise is faster in boys. There is a negative correlation between lactate threshold as a percentage of peak VO2 and age but differences related to maturation or sex remain to be proven. Young athletes have higher peak VO2, a faster primary time constant and accumulate less blood lactate at the same relative exercise intensity than their untrained peers. Young people can increase their peak VO2 through exercise training but a meaningful relationship between aerobic fitness and HPA has not been demonstrated.
Conclusions During youth the responses of the components of aerobic fitness vary in relation to age, maturation and sex. Exercise training will enhance aerobic fitness but a relationship between young people's current HPA and aerobic fitness remains to be proven.
Statistics from Altmetric.com
Introduction
The aims of this review are to analyse aerobic fitness during growth and maturation and to examine the relationships between aerobic fitness and participation in sport, exercise training and habitual physical activity (HPA) during youth. Studies for review were located through computer searches of Medline, SPORT Discus and personal databases. Systematic reviews of time trends in aerobic fitness/performance and exercise training and peak VO2 are reported.
Aerobic fitness
Aerobic fitness may be defined as the ability to deliver oxygen to the muscles and to utilise it to generate energy to support muscle activity during exercise. Peak oxygen uptake (peak VO2), the highest rate at which oxygen can be consumed during exercise, is recognised as the best single measure of young people's aerobic fitness.1 2 Peak VO2 limits the rate at which oxygen can be provided during exercise and a high peak VO2 is a prerequisite of elite performance in many sports but it does not describe all aspects of aerobic fitness. In several sports and in everyday life intermittent exercise and the ability to engage in rapid changes in exercise intensity are at least as important as peak VO2. Under these conditions, it is the transient kinetics of VO2 which best describe the relevant component of aerobic fitness.3 Furthermore, during sustained exercise lactate accumulates within the muscle and diffuses into the blood to provide an estimate of the relative aerobic and anaerobic contribution to the exercise. Blood lactate accumulation therefore provides a useful indicator of aerobic fitness with reference to the ability to sustain submaximal exercise.4
Peak oxygen uptake
Peak VO2 during youth has been extensively documented.5 6 Figure 1 represents ∼5000 peak VO2 (l/min) values of 8–16-year-olds. These data must be interpreted cautiously as they represent mean values from studies with volunteer samples of varying sizes. Nevertheless, the figure clearly shows an almost linear increase in boys' peak VO2 in relation to chronological age. Girls' data demonstrate a similar but less consistent trend with some cross-sectional studies suggesting a tendency to plateau at about 14 years of age. Regression equations generated from these data indicate that peak VO2 increases from 8 to 16 years by 150% and 80% in boys and girls respectively.6

Peak oxygen uptake in relation to chronological age. From Armstrong and Welsman6 with permission.
The few longitudinal studies available reflect the cross-sectional data with some studies indicating large age-related increases in boys' peak VO2 between 13 and 15 years. Girls' data are less consistent but in accord with cross-sectional findings they indicate a progressive rise from 8 to 13 years with a gradual levelling-off in peak VO2 from age 14 years. Longitudinal data indicate that boys' peak VO2 almost doubles from 11 to 17 years with girls' values increasing by ∼ 50% over the same age range.5
Peak VO2 is strongly correlated with body mass and this is conventionally controlled for by simply dividing peak VO2 (ml/min) by body mass (kg) and expressing it as the simple ratio ml/kg/min. When peak VO2 is expressed in this manner a different picture emerges with boys' peak VO2 remaining remarkably consistent from 6 to 18 years at ∼ 48 ml/kg/min with girls' values showing a decline from ∼ 45 to 35 ml/kg/min.5 6 The reporting of peak VO2 in ratio with body mass is of interest in the context of sports where body mass is moved or health where the movement of body mass is required for normal locomotion but it has clouded the physiological understanding of peak VO2 during growth and maturation.7 8
Numerous studies have showed that ratio scaling can lead to inappropriate interpretation of physiological variables.9 Using multi-level modelling, longitudinal studies of both trained10 and untrained11 youth have demonstrated that, in addition to chronological age, both growth and maturation positively and independently influence peak VO2. With body mass appropriately controlled for, boys' peak VO2 increases through childhood and adolescence into young adulthood. Girls' peak VO2 increases at least into puberty and possibly into young adulthood.8 In addition, maturation is associated with increases in peak VO2 above those explained by body size, body composition, and chronological age.12 13 These changes, although in conflict with the conventional interpretation of peak VO2, are wholly consistent with both the underlying physiological processes and improvements in sport performance in relation to growth and maturation.14 15
Girls' peak VO2 (l/min) values are about 10% lower than those of boys during childhood and the sex difference reaches ∼ 35% by age 16 years.5 6 There are no consistent data to support sex differences in maximal heart rate but the balance of evidence suggests that maximal stroke index is higher in boys than in girls although there are conflicting data on whether this is due to cardiac size or function.16 17 Data on maximal arterial-venous oxygen difference are sparse and equivocal with no persuasive evidence to support sex-related differences during childhood.5 Sex differences in peak VO2 during adolescence have been attributed to differences in HPA. Boys are generally more active than girls but HPA patterns show that both sexes rarely experience the intensity and duration of activity associated with increases in peak VO2.18
Physiological explanations for sex differences in peak VO2 during adolescence include boys' greater muscle mass and blood haemoglobin concentration. Muscle mass increases through childhood and adolescence in both sexes but although boys generally have greater muscle mass than girls in childhood marked sex differences do not become apparent until the adolescent growth spurt. From 5 to 16 years of age, boys' relative muscle mass increases from about 42–54% of body mass. Girls experience a less dramatic adolescent growth spurt than boys and from age 5–13 years muscle mass increases from about 40–45% of body mass. In relative terms it then declines due to girls' increase in body fat during adolescence. Boys' greater muscle mass not only facilitates the utilisation of oxygen by the muscles but also supplements the venous return to the heart and therefore augments stroke volume through the peripheral muscle pump. Muscle mass appears to be the dominant influence in the increase in peak VO2 through adolescence.5
Blood haemoglobin concentration is correlated with peak VO2 in both sexes.19 There are no significant sex differences in haemoglobin concentration in childhood but during puberty the effect of testosterone on red blood cell production stimulates noticeable increases in boys' haemoglobin concentration which reach values ∼10% higher than those of girls by late puberty. It is reasonable to expect that boys' superior oxygen-carrying capacity may augment sex differences in peak VO2. However, the transport and dissociation of oxygen from haemoglobin during exercise is complex and sex differences in maximal arterial-venous oxygen difference during youth remain to be proven.5
Oxygen uptake kinetics
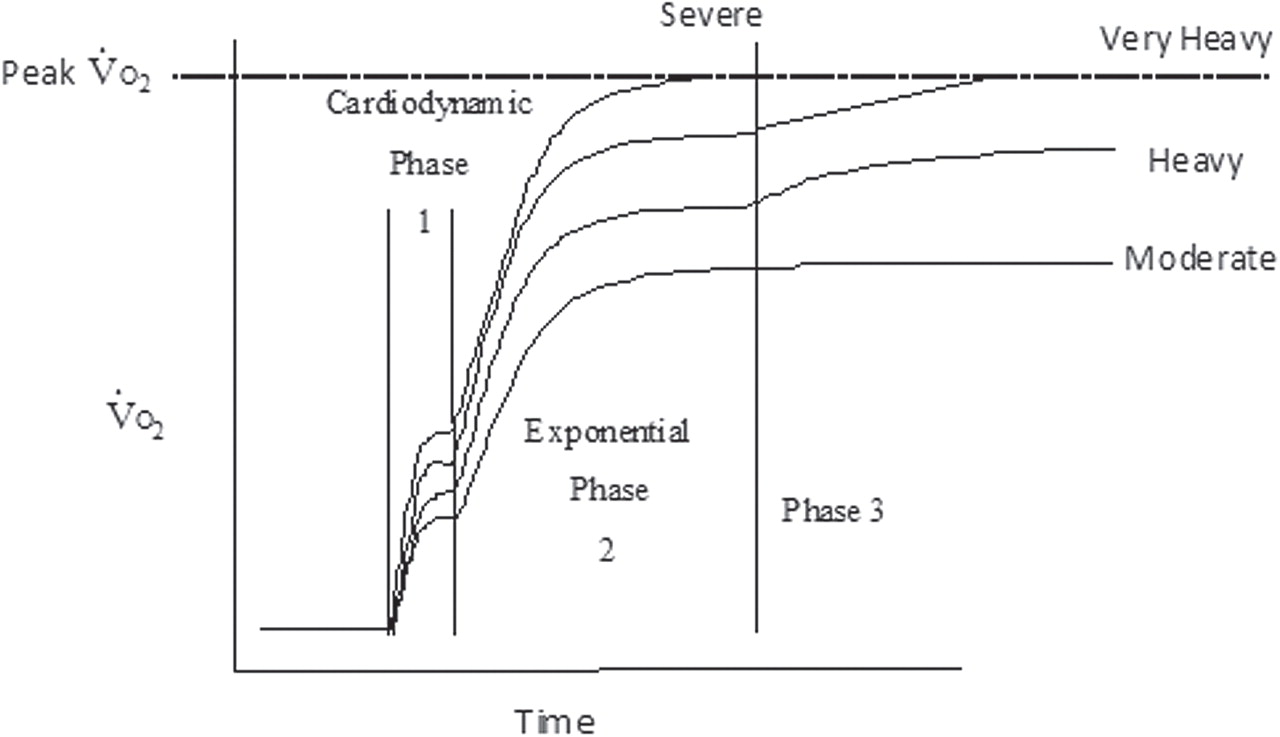
The VO2 kinetic response to step changes in exercise intensity is described in figure 2 and can be defined in relation to a number of exercise domains. Rigorously determined and analysed data with young people, however, are only available in the moderate (ie, below the lactate threshold (TLAC) and heavy (ie, above the TLAC but below the maximal lactate steady state (MLSS) or critical power) intensity exercise domains.3

The three phases of the response to a step change in exercise in four different exercise intensity domains. From Fawkner and Armstrong3 with permission.
At the onset of a step transition from rest to moderate intensity exercise there is an almost immediate increase in VO2 measured at the mouth. This cardio-dynamic phase (Phase I) lasts about 15 s in children and is associated with an increase in cardiac output, which occurs before the arrival at the lungs of venous blood from the exercising muscles. Phase I is independent of muscle VO2. The cardio-dynamic phase is followed by an exponential increase in VO2 (Phase II, the primary component) that drives VO2 to a steady-state value (Phase III) within about 2 min with an oxygen cost of about 10 ml/min/Watt above that found at rest (or more usually during exercise tests, unloaded pedalling). The principal variable of interest is the time constant (τ) of the VO2 primary component which reflects, within about 10%, the kinetics of VO2 at the muscles.20 21 The shorter the τ the smaller the anaerobic contribution to the step change in exercise intensity. During a step change to heavy intensity exercise the Phase II oxygen cost is similar to that observed with moderate intensity exercise. However, the oxygen cost increases over time as a slow component is superimposed and the achievement of a steady-state is delayed by 10–15 min. The mechanisms underlying the slow component remain speculative but appear to be a function of muscle fibre distribution, motor unit recruitment and the matching of oxygen delivery to active muscle fibres.22 23
Boys have a faster τ than girls during the transition from rest to heavy exercise24 but VO2 kinetic responses to a step change to moderate intensity exercise are independent of sex.25 The τ of the Phase II exponential rise in VO2 during youth has been showed to be age-dependent during step changes to both moderate25 and heavy26 27 intensity exercise. A longitudinal study of the VO2 kinetics of heavy intensity exercise reported a slowing of the VO2 primary component τ and a reduction in the Phase II oxygen cost in both boys and girls, who were prepubertal at the onset of the study.26 A slow component was demonstrated on both occasions contributing about 10% of the final VO2 on the first occasion and 15% of the final VO2 on the second occasion. These findings have been replicated with 13–16-year-old boys27 and are consistent with the presence of an age-dependent influence on muscles' potential for oxygen utilisation. Any independent effects of maturation remain to be explored.
During youth peak VO2 is not related to the VO2 primary component τ during the transition to either moderate25 or heavy27 intensity exercise. This is not surprising as peak VO2 is largely dependent on oxygen delivery to the muscles whereas young people's VO2 kinetics in these exercise domains appear to be primarily related to oxygen utilisation by the muscles.3
Blood lactate accumulation
Blood lactate accumulation is a function of several dynamic processes including muscle production, muscle consumption, rate of diffusion from muscle into blood and rate of removal from blood. Blood lactate therefore cannot be assumed to have a direct relationship with rate of muscle production and values must be interpreted cautiously. At the onset of incremental exercise there are minimal changes in blood lactate with rate of diffusion from the muscle matched by rate of removal from the blood. As exercise intensity increases a point is reached where lactate rises rapidly with a steep rise to exhaustion. The first observable increase in lactate above resting level during incremental exercise is referred to as the TLAC. The highest exercise intensity that can be sustained without incurring a progressive accumulation of blood lactate is called the MLSS.4
There are no sex differences in blood lactate accumulation with exercise during youth. Children accumulate less blood lactate than adults during both submaximal and maximal exercise and there is a negative correlation between TLAC (as a percentage of peak VO2) and age. MLSS has generally been found to be negatively correlated with age but this finding has been challenged by a recent study.28 Despite some indications that both muscle29 and blood30 lactate responses are related to maturation, whether maturation independently influences blood lactate accumulation remains to be proven.
Time trends in aerobic fitness
There are no widely recognised recommendations for optimum levels of young people's aerobic fitness and no compelling evidence to suggest that the current generation of youth have low levels of peak VO2.5 Informed debate is, however, divided on whether the ‘aerobic fitness’ of children and adolescents has declined over time.31 32 There are many factors that make it difficult to draw confident conclusions regarding historical changes in aerobic fitness during youth. First, there is a paucity of scientific evidence available; second, most of the available scientific evidence has only made informal historical comparisons, with very occasional rigorous statistical treatment; and third, researchers have not always been clear on their definition of ‘aerobic fitness’ and how it is operationalised.
Using a systematic review and meta-analytical strategy one of us (GRT) reviewed 50 studies that examined historical changes (spanning a minimum of 5 years) in aerobic fitness (operationalised as mass-related peak VO2) or aerobic performance (operationalised as maximal field-based endurance running) of healthy (free from known disease or injury) young people aged 9–17 years. Aerobic fitness data were available for >4002 9–17 year olds from five countries between 1962 and 1994; aerobic performance data were available for >25 245 203 9–17 year olds from 28 countries between 1964 and 2008.
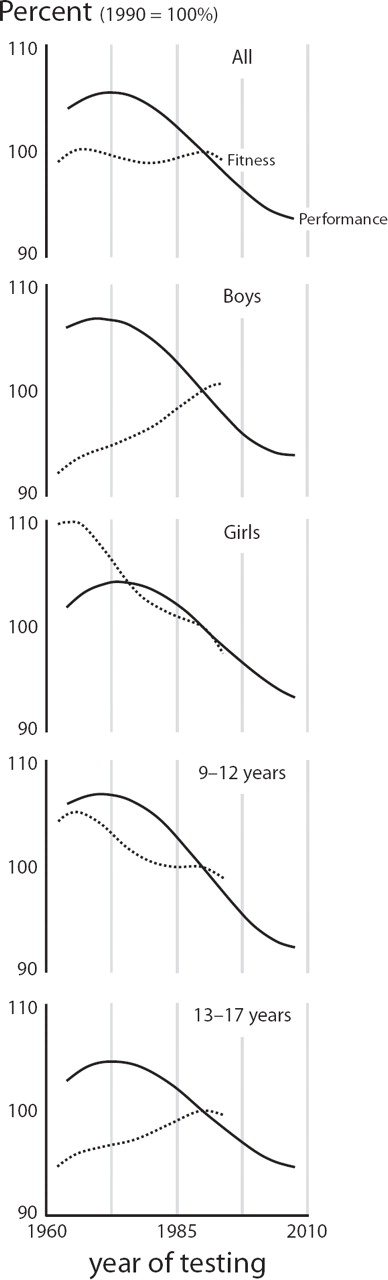
Overall, there has been a very small change in young people's aerobic fitness (mean change ±95% CI: –0.26 ±0.48% or –0.06 ±0.06SDs) (figure 3). Whereas there has been a large decline in young people's aerobic performance since 1975 (mean change ±95% CI: –13.34 ±0.45% or –0.99 ±0.03SDs) (figure 3). Changes in aerobic performance, but not aerobic fitness, were consistent for different sex, age and geographical groups (figure 3). As these results describe historical changes in mean values, it is not clear whether the changes have been uniform or skewed over time, although data suggest that the changes have been typically greater in the poorer performing or least fit children.33,–,37
{kind=link}
{kind=link}
{kind=link}
Worldwide patterns of change in aerobic fitness (dashed lines) and aerobic performance (solid lines) of 9–17 year olds over the periods 1962–1994 and 1964–2008, respectively. Data are presented separately for all children, boys, girls, 9–12 year olds, and 13–17 year olds. Data are standardised to 1990 = 100%, with higher values (>100%) indicating better fitness or performance.
So why has there been little change in aerobic fitness but large declines in aerobic performance? Unfortunately, our understanding of the reported changes in aerobic fitness is confounded by data from different ergometers (eg, cycle, treadmill), and data on relatively small, volunteer samples of young people who might have been athletically inclined. Furthermore, the reported changes in mass-related peak VO2 may reflect changes in the denominator (body mass in kg) rather than the numerator (peak VO2 in ml/min). Conversely, confidence in the decline in aerobic performance is high, because of large representative samples, broad geographical coverage and consistent findings. These changes are probably influenced by a network of social, behavioural, physical, biomechanical, and psychosocial factors as well as physiological variables.38 Causes of a decline over time in maximal aerobic performance are therefore not only a function of changes in peak VO2 but also changes in mechanical efficiency and fractional utilisation of oxygen with affective issues (eg, lack of motivation) and cognitive issues (eg, inability to judge pace) also important.39,–,41 Unfortunately, no historical change data are available for these factors. Performance is, however, affected by increased fat mass and there is convincing evidence of a worldwide increase in young people's body fatness in recent decades.42 43 Increases in fatness explain ∼30–70% of the decline in aerobic performance34 41 but other factors including reduced experience with maximal sustained efforts also play a role. Nevertheless, changes in maximal aerobic performance – the ability to run faster, play harder and play longer – are important for youth health and well-being and successful sport participation, irrespective of the underlying mechanisms.
There are no data on time trends in young people's VO2 kinetic response to changes in exercise intensity or blood lactate accumulation during submaximal exercise.
Aerobic fitness and sport
Peak oxygen uptake
Cross-sectional studies have reported that trained young athletes of both sexes have higher peak VO2 than their untrained peers44,–,46 and focused studies have reported higher peak VO2 than untrained youth in trained cyclists,47,–,49 cross-country skiers,50 swimmers51,–,54 and canoeists.50 Young male athletes tend to have higher peak VO2 than young female athletes and although this is probably due to the sex differences described earlier variations in training volume cannot be ruled out. Peak VO2 values of >50 ml/kg/min and >60 ml/kg/min for trained girls and boys respectively have been regularly observed. As almost all studies report cross-sectional data it is unknown whether differences in the peak VO2 of trained and untrained youth are due to initial selection for sport, subsequent training programmes or both.
There is no compelling evidence to suggest that either maximal heart rate or maximal arterial-venous oxygen difference change with training during youth and the higher peak VO2 of young athletes appears to be a function of enhanced stroke volume.46 47 The practical difficulties of determining young people's stroke volume during exercise mean that data should be treated with caution.55 However, the literature is consistent in reporting higher stroke volumes56,–,58 and stroke indices47 57 in trained children and adolescents compared with their untrained peers. A single prospective study has supported these findings by observing significant increases in both boys' (+15%) and girls' (+11%) stroke volumes following a 13 week endurance training programme, with no changes noted in control groups.59
There are marked inconsistencies in studies exploring the underlying mechanisms of enhanced stroke volumes with training and they are confounded by uncontrolled variables such as age, maturity, training volume and years of training. It appears reasonable to suggest that training may enhance stroke volume through a more effective peripheral muscle pump and/or plasma volume expansion increasing venous return but empirical support of this hypothesis is not available. Data on training-induced changes in cardiac dimensions are equivocal with some studies reporting larger left ventricular dimensions at rest47 59 and at maximal exercise47 in trained youth and others observing no differences in left ventricular size and mass.44 60 Most60 61 but not all46 studies have reported no differences between trained and untrained youth in ventricular wall thickness. Prospective data on young people are sparse and inconsistent with some studies observing no significant training-induced changes in cardiac dimensions62 63 and others reporting significant increases with training.59 61 Estimates of shortening fraction and ejection fraction at rest have been observed to be similar in trained and untrained children47 61 but trained children have been reported to increase their shortening fraction more than untrained children during maximal exercise.64
Oxygen uptake kinetics
In adults, training results in a shorter VO2 primary component τ and a smaller VO2 slow component but no prospective data on young people are available. Two studies from the same research group compared the VO2 kinetics of trained prepubertal swimmers to untrained children.65 66 Both studies determined VO2 kinetics during cycle ergometry and reported no differences in the VO2 primary component τ during the transition to exercise either above or below the TLAC. No significant change in the VO2 slow component was observed during exercise above the TLAC. The responses to exercise above TLAC were confirmed in a similar study that compared the cycle ergometer-determined VO2 kinetic responses to a step change to heavy exercise of a group of 11-year-old girl swimmers with an untrained control group.67 However, when the girls' VO2 kinetics was determined during arm (rather than leg) ergometry the swimmers exhibited a significantly shorter VO2 primary component τ than the control group, thus supporting the specificity of training on VO2 kinetics. There were no significant differences in arm cranking peak VO2 between the two groups suggesting that training-induced changes in VO2 kinetics are not related to changes in peak VO2. As heart rate kinetics was also not related to VO2 kinetics, it was suggested that the mechanism underpinning the faster VO2 kinetics in the swimmers was enhanced oxygen utilisation by the muscles.
A similar study by the same research group but with 14-year-old pubertal girls reported significantly faster VO2 kinetics in trained girls during both upper and lower body ergometry. The authors attributed the contrasting results in prepubertal and pubertal girls to both a greater stage of maturation and a longer training history in the pubertal girls. Furthermore, they suggested that, in contrast to their conclusion with prepubertal girls, the faster VO2 kinetics in the trained pubertal girls was influenced by both central and peripheral factors.68
The only other published study on the topic to date examined the cycle ergometer-determined VO2 kinetic responses of 15-year-old boys from a Premier League football academy to the transition from rest to moderate intensity exercise and compared them to an age-matched control group. The footballers demonstrated a significantly faster VO2 primary component τ than the control group. The authors postulated that the faster VO2 kinetics of the footballers were due to increases in both oxygen delivery and oxygen utilisation.69
Blood lactate accumulation
The assessment and interpretation of blood lactate accumulation is challenging and the role, in children and adolescents, of a potential reduction in lactate diffusion from the muscles to the blood and/or an enhanced lactate clearance from the blood remains to be investigated. Nevertheless, data consistently demonstrate that young athletes accumulate less blood lactate than untrained youth at the same relative exercise intensity.4
It has been reported that TLAC in trained youngsters occurs at a higher percentage of peak VO2 than in untrained youth.70 71 The running speed corresponding to a blood lactate accumulation of 4 mM has been observed to increase following training.72 73 Intervention studies have reported high intensity74 75 but not low intensity58 76 training to result in a decrease in blood lactate accumulation during subsequent submaximal exercise. No study has specifically examined the potential mechanisms underlying training-induced reductions in young people's blood lactate accumulation during subsequent submaximal exercise but data from studies of adults suggest that an increase in oxidative capacity is the primary mechanism.77
Aerobic fitness and exercise training
The only component of young people's aerobic fitness on which there are sufficient data to estimate a dose-response relationship with exercise training is peak VO2. In a systematic review of the literature one of us (NA) located 69 published training studies and identified 21 investigations which had rigorously examined the effect of structured exercise training on young people's peak VO2 (table 1). It was concluded that there is a small but significant inverse relationship between baseline (pretraining) peak VO2 and training–induced changes but no relationship between baseline HPA and peak VO2 responses to training. An appropriate 12 week training programme will induce, on average, an 8–9% increase in peak VO2 which is independent of sex, age and maturation. Greater increases in peak VO2 are likely with longer periods of training but further research is required to evaluate the strength of the genetic contribution to responses to training.78
Peak oxygen uptake and exercise training
The recommendations of the International Olympic Committee consensus statement on ‘Training the elite young athlete’79 are based on the interpretation of these data (table 2).
Exercise prescription for improvement of peak oxygen uptake
Aerobic fitness and HPA
Studies stretching back over 35 years have analysed the peak VO2 of children and adolescents in relation to their HPA and consistently shown no meaningful relationship between the two variables.80 81 All located studies which objectively estimated HPA and directly measured peak VO2 are tabulated in chronological order in table 3. It could be argued that pre-1990 studies82,–,85 did not monitor HPA long enough for it to be representative of normal physical activity (PA) behaviour but as data are sparse all studies have been included for completeness.
Habitual physical activity and peak oxygen uptake in youth
A longitudinal study of over 200 children used multilevel modelling to examine HPA, from the ages of 11–13 years. Peak VO2 was investigated as an additional explanatory variable of HPA but once age, gender and maturity had been controlled a non-significant parameter estimate was obtained.86 The Amsterdam Growth and Health Study reported that a 30% increase in HPA score over a 15-year period was associated with a 2–5% increase in VO2 max and concluded that, ‘no clear relation can be proved between PA and VO2 max in free living males and females’ (p. 163).87 Other studies have failed to observe a meaningful relationship between children's HPA and blood lactate indices of aerobic fitness.88 89 HPA has not been investigated in relation to VO2 kinetics.
Conclusions
Peak VO2 during childhood and adolescence is well-documented but other aspects of aerobic fitness during youth are less well-understood. There is no compelling evidence to suggest that low levels of peak VO2 are common and data indicate that youth peak VO2 has remained stable over several decades. However, young people's maximal aerobic performance involving the transport of body mass is important for health and well-being and successful sport participation and this has markedly declined over the last 35 years. Young athletes have higher peak VO2, faster τ during step changes in exercise intensity and accumulate less blood lactate during submaximal exercise than their untrained peers. Sufficient dose-response data are available to design exercise training programmes to improve the peak VO2 of both trained and untrained children and adolescents. However, data on the effects of different exercise training programmes on blood lactate accumulation are sparse and in the case of VO2 kinetics non-existent. Young people rarely experience HPA of sufficient intensity and duration to enhance peak VO2 and there appears to be no meaningful relationship between peak VO2 and HPA. More research focusing on the mechanisms driving exercise-induced changes in aspects of aerobic fitness during growth and maturation is needed.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.