Article Text

Abstract
Objective Elite youth soccer players have a relatively high risk for injuries and illnesses due to increased physical and psychosocial stress. The aim of this study is to investigate how measures to monitor stress and recovery, and its analysis, provide useful information for the prevention of injuries and illnesses in elite youth soccer players.
Methods 53 elite soccer players between 15 and 18 years of age participated in this study. To determine physical stress, soccer players registered training and match duration and session rating of perceived exertion for two competitive seasons by means of daily training logs. The Dutch version of the Recovery Stress Questionnaire for athletes (RESTQ-Sport) was administered monthly to assess the psychosocial stress–recovery state of players. The medical staff collected injury and illness data using the standardised Fédération Internationale de Football Association registration system. ORs and 95% CIs were calculated for injuries and illnesses using multinomial regression analyses. The independent measures were stress and recovery.
Results During the study period, 320 injuries and 82 illnesses occurred. Multinomial regression demonstrated that physical stress was related to both injury and illness (range OR 1.01 to 2.59). Psychosocial stress and recovery were related the occurrence of illness (range OR 0.56 to 2.27).
Conclusions Injuries are related to physical stress. Physical stress and psychosocial stress and recovery are important in relation to illness. Individual monitoring of stress and recovery may provide useful information to prevent soccer players from injuries and illnesses.
Statistics from Altmetric.com
Introduction
Several studies have examined intrinsic (person-related) and extrinsic (environment-related) risk factors for injuries in soccer players.1,–,9 A previous injury and age are known intrinsic risk factors. Extrinsic risk factors such as physical stress (ie, training and matches) and psychosocial stress also seem to increase the injury risk. Since these extrinsic factors can be modified, theoretical models have been developed to explain their influence.
The model of Kenttä and Hassmén10 describes the athletic balance, which consists of physical and psychosocial stress and recovery components. A disturbed balance between these factors contributes to the development of a local or general overload. Andersen and Williams11 explained the underlying mechanism between stress and the occurrence of traumatic injuries. They stated that when athletes experience stressful situations, psychosocial stress contributes to their stress response. The consequences are increases in muscle tension, narrowing of the visual field and increase in distractibility. These changes make athletes more susceptible to traumatic injury.11
Support for these models has been provided in the literature.1,–,9 However, the methodological designs of most of these studies are inadequate for the development of prevention strategies. In these studies, training frequency or life event stress was only investigated at the start of the season, and therefore, it was not possible to incorporate seasonal changes or to warn and guide soccer players at risk. For this purpose, research that monitors physical and psychosocial stress and recovery continuously is needed. Additionally, practical measures should be used.
So far, a few studies monitored training load longitudinally and investigated its relation with the occurrence of injuries.8 12,–,14 However, these studies have three limitations. First, none of these studies made a distinction between traumatic and overuse injuries. A separate analysis is important, since differences exist in the risk factors involved as well as in the mechanisms leading to a traumatic injury or overuse injury. Second, some studies only included injuries that led to time loss, while medical attention injuries should be included to gain a more realistic view of the medical problems.12 14 Finally, illness seems also to be related to the balance between stress and recovery. It is already known that moderate exercise may stimulate the immune system, but that heavy training actually results in immunosuppression and an increased susceptibility to infections.15,–,18 However, data on the psychosocial stress–recovery balance in relation to the occurrence of illnesses are lacking.
To our knowledge, no research that monitors the stress–recovery balance and investigates its relation with injuries and illnesses in soccer players has been published so far. In particular, evidence in elite youth players is lacking. These adolescents who strive to become professionals are particularly at risk of sustaining injuries and illnesses.6 15,–,19 Besides physical stress due to increased training load, psychosocial stress also plays an important role. These players often experience high pressure to succeed from both parents and coaches.20 21 The aim of this study is to investigate how measures to monitor stress and recovery, and its analysis provide useful information for the prevention of injuries and illnesses in elite youth soccer players.
Methods
Study design
A prospective longitudinal cohort design was used to monitor stress, recovery, injuries and illnesses during two competitive seasons in elite Dutch male soccer players from the ages of 15 to 18 years. The procedures were conducted in accordance with the ethical standards of the Central Committee on Research Involving Human Subjects.
Subjects
During the 2006–2007 and 2007–2008 competitive seasons, 53 players participated in this study. Twenty-four participated during two competitive seasons and 29 during one competitive season. These 29 players were selected, deselected or moved to a higher age category at the start of the second season. The teams competed at the highest national competition level in The Netherlands and belonged to the best 1% of players in their age category. The current third place on the Fédération Internationale de Football Association (FIFA) world football ranking illustrates that soccer is played at a high level in The Netherlands. At the start of each season, height, weight and body fat were determined (table 1).
Physical characteristics of the elite youth soccer players
Data collection
Injuries and illnesses
The members of the medical staff, a physician and two physical therapists, diagnosed and recorded injuries and illnesses during the two competitive seasons. Players had free access to the medical staff at all times. The definitions and data-collection procedures that were used, follow the recommendations of the consensus statement for soccer injury studies, that is the FIFA registration system.22 An injury was defined as: ‘Any physical complaint sustained by a player that results from a soccer match or soccer training, irrespective of the need for medical attention or time loss from soccer activities.’ Injuries were reported if a player was unable to take full part in future soccer training or match play (time loss). Additionally, injuries were reported if players received medical attention for more than 1 day but still were able to take full part in future soccer training or match play. Traumatic injuries were defined as injuries that resulted from a specific, identifiable event. Overuse injuries were defined as injuries caused by repeated microtrauma without a single identifiable event. In some cases, multiple injuries that resulted from the same activity were counted as one injury event.22 23 Injuries were classified according to the location, type, mechanism and severity of injury. The main groupings and categories for classifying the location and type of injury are represented in figures 1 and 2, respectively. The severity of injury was defined as the number of days that the injured player could not fully participate in team training or match play: slight (no absence from training and match), minimal (1–3 days), mild (4–7 days), moderate (8–28 days), severe (more than 28 days) and career-ending injuries.22 23 An illness was defined as a circumstance in which the subject—after consulting the medical staff—was withdrawn from training or match because he did not feel well and was limited or unable to perform athletic activities due to flu and common cold-related symptoms (eg, fever, muscle aching, diarrhoea, malaise).24 Illness was distinguished from overtraining based on the time to full recovery and the disappearance of flu- and cold-related signs and symptoms within a reasonable period of time.25 In case of prolonged symptoms, further clinical and additional blood and/or radiological examinations were performed to find an underlying cause. If no explanation was found and symptoms persisted, the subject was diagnosed to be overtrained instead of having an illness. Four players were diagnosed as having an early stage of overtraining and excluded from the analyses.

Injury locations and severity in elite youth soccer players. Injuries, number (percentage); 0, slight (no absence from training and match); 1, minimal (1–3 days); 2, mild (4–7 days); 3, moderate (8–28 days); 4, severe (>28 days).

Injury types in elite youth soccer players.
Measures to monitor stress and recovery
Physical stress
Physical stress was quantified in two different ways. First, the duration of training sessions and matches in minutes was used as an objective measure. For every week, the sum of the duration of training and matches over the preceding week was calculated. The total duration over the preceding week was divided by 60 to transform minutes into hours. Second, the rate of perceived exertion (RPE) was used to determine the internal training load.26 Each player was instructed to rate the global intensity of each training session using the original Borg 15-point scale by answering the simple question, ‘How was your workout?’ Session-RPE scores were obtained 30 min after completing the training session to ensure that the perceived effort was referred to the whole session rather than the most recent exercise intensity.26,–,28 When compared with heart rate and blood lactate concentration, this method has been shown to be a good indicator of global internal load in soccer.28 The product of the session-RPE and the duration of the training session were defined as the training session load.12 26 27 The weekly load was defined as the sum of the load of all training sessions over a 1-week period. If more than 25% of the RPE scores within a week were missing, participants were excluded from further analyses. Otherwise, the missing RPE score was replaced with the mean RPE score of the corresponding week. A zero was noted for days with no training. Monotony was calculated from the daily mean load divided by the SD of the daily mean load over a 1-week period. The strain was defined as the product of weekly load and monotony.12 26 27 The weekly load, monotony and strain over the preceding week prior to injury or illness were calculated. Similar to duration, weekly load and strain were divided by 60.
Psychosocial stress and recovery
The Dutch version of the Recovery Stress Questionnaire for athletes (RESTQ-Sport) was administered monthly to assess the psychosocial recovery–stress state of players. The RESTQ-Sport consists of 12 general and seven sport-specific scales with four questions per scale and one warm-up question. Each player was instructed to rate the 77 items on a Likert-type scale, with anchors of 0: never and 6: always, indicating how often he participated in recovery and stress-related activities during the last 4 weeks.29
In addition, the RESTQ-Sport scores were classified in general stress scores (Σ 7 general stress subscales), sport-specific stress scores (Σ 3 sport-specific stress subscales), general recovery scores (Σ 5 general recovery subscales) and sport-specific recovery scores (Σ 4 sport-specific recovery subscales). In case of missing data, the mean of a subscale was calculated when at least three out of four of the items were rated. This procedure was executed in 19 out of 586 questionnaires. High scores on the stress-associated scales reflect a frequency of stress activities, whereas high scores on the recovery-oriented scales represent a high frequency of recovery activities.29 Nederhof et al30 showed that the Dutch RESTQ-Sport had sufficient reliability and validity for use in sports practice and research.
Statistical analysis
The injury incidence was calculated as the number of injuries per 1000 match or training hours. The illness incidence was calculated as the number of illnesses per 1000 playing hours.31 Descriptive statistics (mean and SD) were calculated for the measures of stress and recovery (duration and training load/monotony/strain RESTQ subscales) of injured, ill and healthy players. Data were analysed using multinomial regression in SPSS 16.0 (SPSS, Chicago, Illinois). Dependent variable was coded as traumatic injury, overuse injury and illness. The healthy group was set as the reference category. ORs and 95% CIs were calculated for the independent measures of stress and recovery. Differences with a p value less than 0.05 were considered significant.
Results
Injuries and illnesses
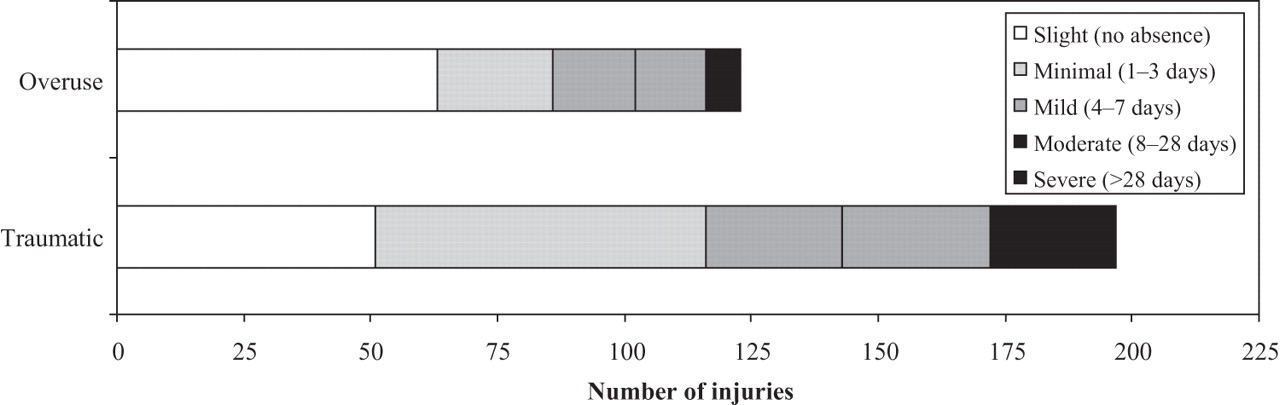
During the study period, 320 injuries and 82 illnesses occurred. Two-hundred and six (64%) were time-loss injuries and 114 (36%) medical attention injuries. The injury incidence was 37.55 per 1000 match hours (26.65 when analysing only time-loss injuries) and 11.14 per 1000 training hours (6.74 when only analysing time-loss injuries). The incidence of illnesses was 5.27 per 1000 playing hours. Most of the injuries were located in the lower extremities (85%) (figure 1). Muscle strain/rupture/tear/cramps (38%) were the most frequently occurring injury type (figure 2). Figure 3 presents the proportion and severity of traumatic and overuse injuries.

Injury mechanism and severity in elite youth soccer players. 0, slight (no absence from training and match); 1, minimal (1–3 days); 2, mild (4–7 days); 3, moderate (8–28 days); 4, severe (>28 days).
Stress and recovery
Table 2 presents descriptive statistics for the measures of stress and recovery. It displays the mean sum of the duration of training and matches, and the mean sum of the training load, monotony and strain of injured, ill and healthy players. Furthermore, it displays the general and sport-specific stress and recovery scores for these groups.
Stress and recovery in young elite soccer players
Relation between physical stress and traumatic injuries, overuse injuries and illnesses
Physical stress was related to traumatic injuries, since the weekly duration, training load, monotony and strain over the preceding week were significantly higher for players with a traumatic injury compared with healthy players (table 3). No significant differences were found in physical stress between players suffering from an overuse injury compared with healthy players. The weekly duration over the preceding week was significantly higher for ill players than for healthy players. Figure 4 shows an example in which the weekly duration is plotted together with medical problems experienced by a player.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Example of a temporal linkage between weekly duration and traumatic injuries, overuse injuries and illnesses. The horizontal line is set at 8.7 h (mean+1 SD of the healthy group) as a threshold. It suggests a relation with part of the medical problems experienced by the player. Note, for example, the preceding spike before illness.
Multinomial regression of physical stress; ORs and 95% CIs for the three groups: traumatic, overuse and illness
Relation between psychosocial stress and recovery, traumatic injuries, overuse injuries and illnesses
The analysis of the RESTQ-Sport showed no clear relation between specific components of stress and recovery and the occurrence of injuries (table 4). Subscale fitness/injury was significantly higher for players with a traumatic injury as well as for players with an overuse injury compared with healthy players. Ill players reported significantly more general stress than healthy players in six out of seven subscales, with emotional stress having the highest OR and fatigue the lowest OR. Furthermore, they perceived significantly less social recovery, general well-being and sleep quality. Finally, on the sport-specific components of the RESTQ-Sport, ill players reported significantly more disturbed breaks and emotional exhaustion, and felt less fit and less in shape.
Multinomial regression of psychosocial stress and recovery; ORs and 95% CIs for the three groups: traumatic injury, overuse injury and illness
Discussion
The present prospective study demonstrated that physical stress plays an important role in relation to the occurrence of both injuries and illnesses. In addition, psychosocial stress and recovery are important in relation to illness. The methodological approach used in this study provides new insights for a prevention strategy, since players were monitored with daily training-logs and monthly questionnaires for two competitive seasons. In this way, monitoring stress and recovery can possibly warn and guide soccer players who are at risk for injuries and illnesses.
Regarding the injury incidence, we used the recently proposed FIFA registration system, which makes a comparison with previous literature interesting.22 For time-loss injuries, our match injury incidence is comparable with other studies, but our training injury incidence is slightly higher. This might be explained by a difference in injury definition. For example, Le Gall et al19 reported an injury incidence of 11.2 injuries per 1000 match hours and 3.9 injuries per 1000 training hours in a 10-season study in elite French youth soccer players. However, they only recorded injuries that prevented the player from participation for more than 48 h, whereas in our study all injuries resulting in being unable to take full part in future training or match play were recorded as time-loss injuries.
As proposed in the FIFA registration system, we additionally registered injuries of players that needed medical attention but still were able to take full part in future training or match play. These mild injuries explain that the overall injury rate in our study is relatively high. Comparable results were found for the location, type and mechanism of injury.3 6 19 An illness incidence of youth elite soccer players has not been previously reported in literature, but turned out to be a large part of the reported medical problems (20%).
The relation between physical stress and the occurrence of injuries and illnesses found in this study is in accordance with previous literature.12,–,14 24 26 However, these studies differ in type of sport, performance level and gender. Gabbett13 14 found that high training intensity (session-RPE), training duration and training load were related to injuries in subelite rugby-league players, who participated in two or three organised field-training sessions per week. Additionally, Anderson et al12 reported that a high total weekly training load in female collegiate basketball players was related to weekly injuries. In our study, the difference between traumatic and overuse injuries was added. This difference may be interesting, because differences exist in the risk factors involved as well as in the mechanisms leading to a traumatic injury or overuse injury.8 In our study, physical stress seems to be important in relation to the occurrence of traumatic injuries. The difference in OR between monotony and strain is explained by the fact that the OR depends on the unit used in the continuous variable. For every unit increase, the odds of a player being injured increases. Monotony is expressed as a rather small number and consequently has a large OR. In other words, an increase of one unit will have a large effect. One unit strain has a smaller effect, but this is compensated by the fact that extra strain goes together with many units. For overuse injuries, no differences in physical stress were found. However, it is known that an overuse injury is caused by repetitive stress without sufficient time to undergo the natural reparative process.32 Based on the framework of Kenttä and Hassmén, physical stress and recovery are assumed to be most important in relation to overuse injuries.10 A possible explanation might be that a 1-week period prior to an overuse injury is too short to find a relevant relation. Our finding that illness is related to a disturbed balance between stress and recovery is also in accordance with findings in the literature. Foster26 and Putlur et al24 both found a positive relation between training and illness in competitive athletes and female collegiate soccer players, respectively. It should be noted that in our study we used the original Borg scale instead of the category ratio scale (10-point scale). To avoid the association with marks on school exams, we decided to use the original scale. Although this does not effect the results of our study, a comparison with studies that use the category ratio scale should be done with caution.
The RESTQ subscales of stress and recovery showed no clear relation with the occurrence of injuries in this study, except for subscale fitness/injury, which was significantly higher for injured players compared with healthy players. In relation to illness, several stress- and recovery-related items appeared to be important. This is in line with literature that showed that the infection risk is increased when a player is exposed to other stressors to the immune system, including lack of sleep or severe psychosocial stress.17 18 Based on the model of Andersen and Williams11 regarding the underlying mechanism of sports injuries, a relation between psychosocial stress and recovery and the occurrence of injuries was expected. A possible explanation for the fact that no clear relation between specific components of stress and recovery and the occurrence of injury was found in this study may be that the RESTQ-Sport was administered monthly. Perhaps the questionnaire must be administered more frequently to monitor changes in the recovery-stress state of players accurately.
In this study, multinomial regression was used to test whether there were any differences in stress and recovery between players suffering from an injury or illness compared with healthy players. To take into account the fact that players were repeatedly measured, our first analysis was based on random effects models. However, it turned out that interindividual differences were comparable with intraindividual differences. This implies that no extra information was obtained by using these rather complicated models. Also, the generalised estimating equations approach (an alternative method for taking into account correlated measures) did not reveal results other than multinomial regression. Therefore, we chose to present the results of the multinomial regression approach for the sake of simplicity. Since (de)selection of players at the transition of the first season to the second was predominantly based on shifting to a higher age category, we assumed that the data are missing at random and not related to the main outcome. The homogeneity of the group is supported by the fact that players belonged to the best 1% in their age category, and no significant differences were present in their physical characteristics.
Further studies that prospectively monitor stress and recovery and injury and illness for more than two competitive seasons in several elite youth soccer teams are required to investigate the specific relations of traumatic and overuse injuries. In these studies, the analyses of stress and recovery measures should be combined to investigate the relation between the balance of these components and the occurrence of injury and illness. The final goal should be to develop a system that indicates the injury or illness risk of an individual player based on the balance between his personal stress and recovery scores. In this study, we monitored measures of stress and recovery to develop a prevention strategy. From this point forward, research is needed that evaluates if this intervention will lead to a reduction in injuries and illnesses.
Based on the results of this study, trainers, coaches and medical staff may consider monitoring the duration of training and matches and the psychosocial recovery–stress state, and possibly also the training load, monotony and strain of each player. Because of the large variations between players, the individual differences over time are most important in relation to injury or illness prevention. Therefore, trainers need to gain feedback on individual basis to identify when a player has an increased injury or illness risk. If necessary, they can possibly adapt the training schedule or use interventions in which players are learnt to better cope with stress or enhance recovery-related activities.
What is already known on this topic
A disturbed stress–recovery balance is a well-known risk factor for the occurrence of injuries and illnesses.
What this study adds
We prospectively monitored stress and recovery and incidence of medical problems in elite youth soccer players by means of daily logs and monthly questionnaires. These measures of stress and recovery may play a role in a prevention strategy for injuries and illnesses in elite youth soccer players.
Acknowledgments
The authors would like to thank the medical staff, coaches and athletes for their participation. They also thank Richard Dik and Wouter Bonke for their contribution to the data collection.
References
Footnotes
-
Funding This study was financially supported by The Netherlands Organisation for Health Research and Development (ZonMw), grant no 7502.0006.
-
Ethics approval Ethics approval was provided by the Dutch Central Committee on Research Involving Human Subjects.
-
Provenance and peer review Not commissioned; externally peer reviewed.