Article Text

Abstract
Objective To evaluate the time to return to playing following acute Achilles tendon rupture (ATR) and surgical repair in professional male football (soccer) players.
Methods Professional male football (soccer) players who sustained an ATR and underwent surgical repair were identified through internet-based injury reports from January 2008 to August 2018. Only League 1 and 2 players with injuries who had at least 1 year of follow-up from the search date were included. Injury history and time to return to play were retrieved from the public platform transfermarkt.com. For athletes who competed for at least two seasons after returning to play, re-ruptures and number of matches played were reported.
Results 118 athletes (mean age 27.2±7.2 years) were included. 113 (96%) returned to unrestricted practice after a mean of 199±53 days, with faster recovery in players involved in national teams. Return to competition was after a mean of 274±114 days. In the 76 athletes with at least two seasons of follow-up, 14 (18%) did not compete at the pre-injury level during the two seasons following the index injury. Six players (8%) sustained a re-rupture within the first two seasons after return to play; four re-ruptures were in footballers who returned to play <180 days after injury. Age >30 years and re-ruptures had higher odds ratios of not returning to the same level of play.
Conclusions 96% of professional male football players who underwent surgery to repair an ATR returned to unrestricted practice and then competition after an average time of 7 and 9 months, respectively. However, 18% did not return to the same level of play within the two seasons following their return, with a higher risk in those experiencing a re-rupture.
- Achilles tendon rupture
- football (soccer)
- professional
- performance
- return to play
- return to sport
Statistics from Altmetric.com
Introduction
Achilles tendon rupture (ATR) is an injury that commonly occurs during sport participation1 2 and, for the professional athlete, it can be career ending.3 In the general population the clinical outcomes following ATR have been extensively investigated in surgical and non-surgical cases.4–7 In this general population cohort, the return to sporting participation, summarised in systematic reviews and meta-analyses,8 it was found that 80% of 6506 patients were able to perform sport activity after ATR.
There are very limited data with which to advise professional football (soccer) players.9–11 One study of surgical treatment in 36 athletes (25 football players) reported that 91% resumed their preoperative sport activity level,9 but the results for the football cohort were not reported separately. Gajhede-Knudse et al 10 reported a mean lay-off time of 161±65 days after Achilles tendon injuries in nine professional UEFA football (soccer) players, and Franchini et al 11 described return to sport after surgical treatment of ATR in a single case report of a Serie A Elite football (soccer) player. The athlete was able to recover unrestricted sport activity after 25 weeks (175 days), participate in an official match after 27 weeks (189 days) and completed an entire match after 30 weeks (210 days).
Football attracts detailed media attention and public websites can provide robust data.12 13 Data from the public website transfermarkt have been used to assess the return to sport and performance after anterior cruciate ligament (ACL) injuries,14 15 fractures16 and femoro-acetabular impingement17 in professional football (soccer) players. Walden and colleagues,18 in their milestone 15-year UEFA study on return to sport after ACL injury, included data from the website transfermarkt and the club's official website. The reliability of the data from transfermarkt has been validated by other online reference sources without the use of official medical reports.19
We aimed to analyse the time to return to training and match participation following ATR in professional footballers and the occurrence of complications including the re-rupture rate.
Methods
Study sample and data extraction
Professional male football (soccer) players who sustained an Achilles tendon tear and underwent surgical repair were evaluated. The players were identified through internet-based injury reports, player profiles/biographies and press releases as reported by Jack et al.12 Two independent investigators (GR and AG) manually conducted the search during August 2018, screening the google.com website using the keywords 'Achilles Tendon Rupture' and 'Transfermarkt'. All the players were considered eligible if they were found to have an ATR and repair in the last 10 years (between 2008 and 2018), as reported from online sources, and if they were enrolled in a professional football (soccer) team at the time of the injury.
Athletes were excluded from the study if they met at least one of the following exclusion criteria:
Participated in other than First or Second League of National Leagues.
Less than 1 year elapsed from injury to the date of search.
Presence of major injuries not related to sport that precluded the possibility of return to play (eg, vehicle accidents).
Initial injury was partial tear or re-rupture.
From the included players, data on anthropometrics, playing position (goalkeeper, defender, midfielder or forward), country, team and league of play (first or second division), competing with their national team at the international level at any time during their career, injury history and time of return to play were retrieved by a structured search from the publicly available media-based platform transfermarkt.com (Transfermarkt, Hamburg, Germany) by the same two investigators. Any discrepancies were resolved after critical review of controversial information. When the two investigators disagreed, the case was discussed and consensus reached. Data on the number of games played before and after ATR and the occurrence of re-ruptures were also collected in those athletes who played at least two seasons after official return to play. A recently published study20 reported the validity and accuracy of the injury-related data retrieved from transfermarkt.com with interobserver agreement of over 90% between reference sources and Transfermarkt.de and a Cohen’s kappa of 0.82 for cross-validation.20
Return to sport outcomes and Achilles tendon re-ruptures
The time to return to unrestricted practice was defined based on the number of days absent from sport as adopted from transfermarkt and reported by Schiffner et al.19 The time to return to competition was defined as the time from injury to the participation of at least 1 min of an official match, as reported in online sources.
We defined return to the previous level of play as a player playing for at least two entire seasons after the return to unrestricted training following ATR and at least five matches per season in the same division as before he suffered the index injury. We also measured Achilles tendon re-ruptures in players who played for two seasons.
Equity, diversity, inclusion (EDI)
Football is played by millions of women the world over and the British Journal of Sports Medicine encourages research that includes sex and gender-based analysis. When we examined the transfermarkt.com databases for ATR data in female professional players, only two players were found in the whole database and neither had sustained an ATR.
Statistical analysis
Statistical analysis was performed using the statistical software MedCalc. Continuous variables were reported as mean±SD, while categorical variables were reported as number and percentage of the total. Continuous variables were compared using the independent sample t-test, while for categorical variables the χ2 test was used.
Survival analysis was used to evaluate 'time to event' outcomes such as time to return to play and return to competition, and the log-rank test was used to compare survival curves according to different categorical variables.
Logistic regression models were performed using not returning to sport, re-rupture and not returning to same activity level as main outcomes, and body mass index (BMI), role, age, division and national team participation as independent variables. ORs and 95% CIs were reported. The same variables were used to perform a survival Cox regression to assess significant variables in the time to return to play and time to competition, and multiple regression analysis was used to estimate their effect. Coefficient and SE were reported for this analysis. The t-test was used to compare continuous variables of two different subgroups, while the log rank test was used for comparison of survival curves of different levels of categorical variables. P values <0.05 were considered statistically significant.
Results
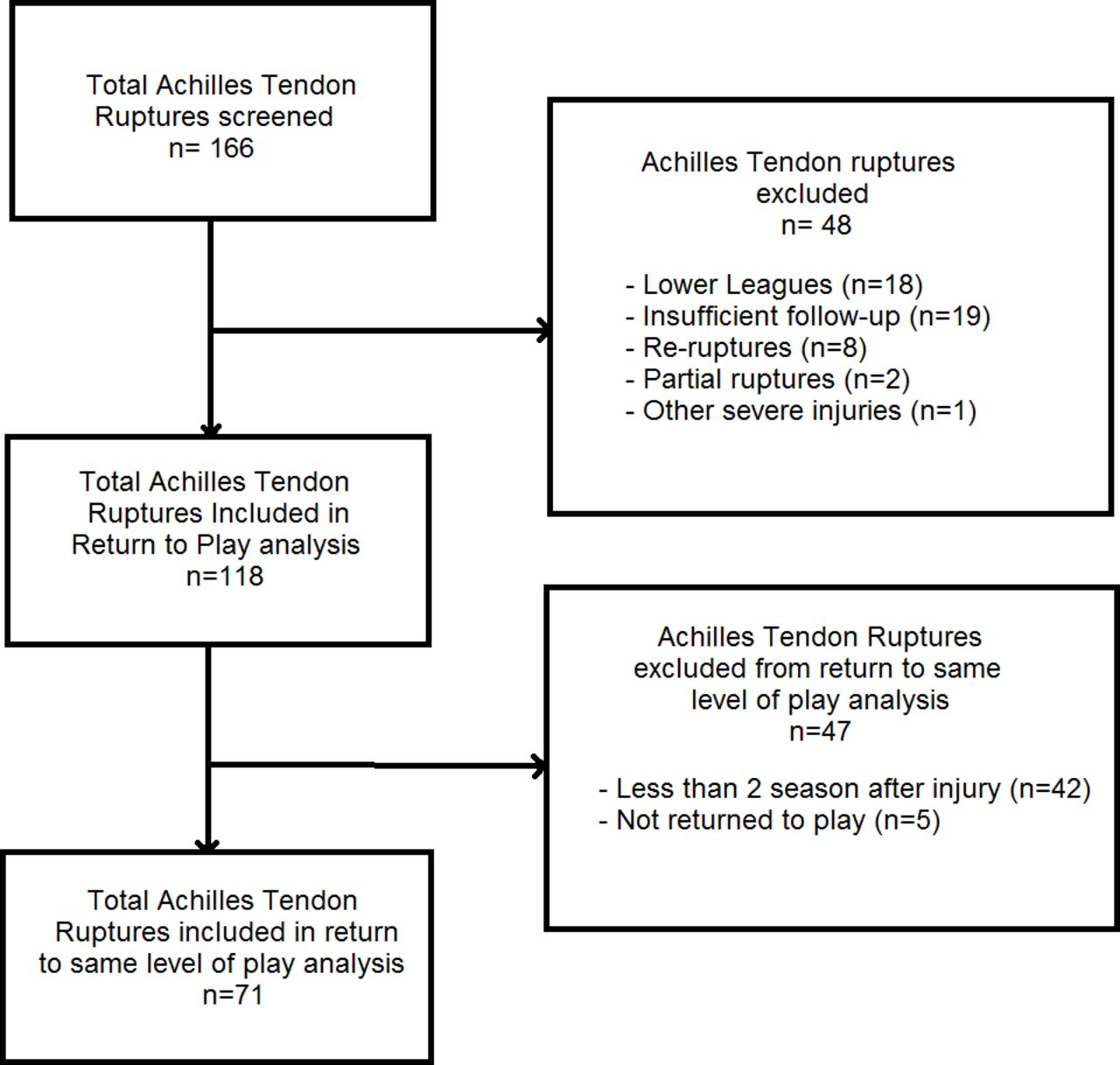
We identified 166 ATRs in professional male football players from our online screening process. A total of 48 athletes were excluded: 18 had participated in lower league football, 19 had ATR less than 1 year before database screening, 8 were re-ruptures, 2 were partial ATR and 1 had a severe accident unrelated to ATR precluding him to full return to play (figure 1). Therefore 118 athletes (9 goalkeepers, 45 defenders, 33 midfielders, 31 forwards) with a mean age at ATR of 27.2±7.2 years were included (table 1); the most represented nationalities were English and German (see online supplementary appendix 1). Eighty-eight players (75%) were participating in the top national league for their respective countries. These included the Premier League (11%), Serie A (7%) and German Bundesliga (5%). Sixty-six (56%) had played at the international level at some point in their career.
Supplemental material

Flowchart of patient inclusion.
Demographic characteristics of players
Return to unrestriced practice
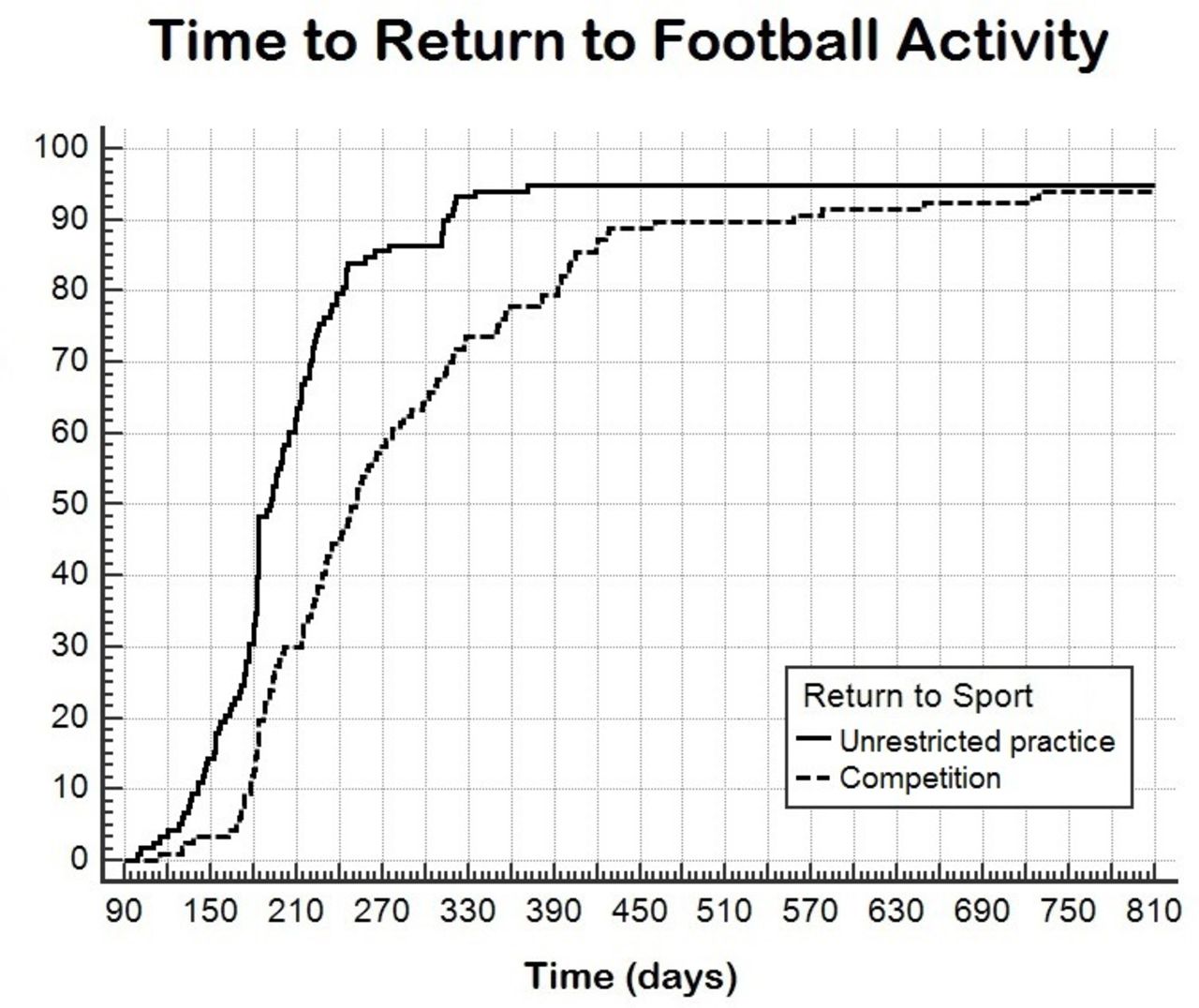
Overall, 113 players (96%) returned to unrestricted football practice after a mean of 199±53 days from injury (figure 2). Players who were classified as ‘international level’ returned to play a mean±SE of 32±11 days earlier than the other players in the cohort (p<0.005) (table 2 and figure 3). There were no differences between player positions and time to return to unrestricted practice (figure 4). Of the five players who did not return to football practice after ATR, four (aged 24, 31, 35 and 35 years) retired and one was released. No predictors for not returning to play were identified by logistic regression analysis (table 3).
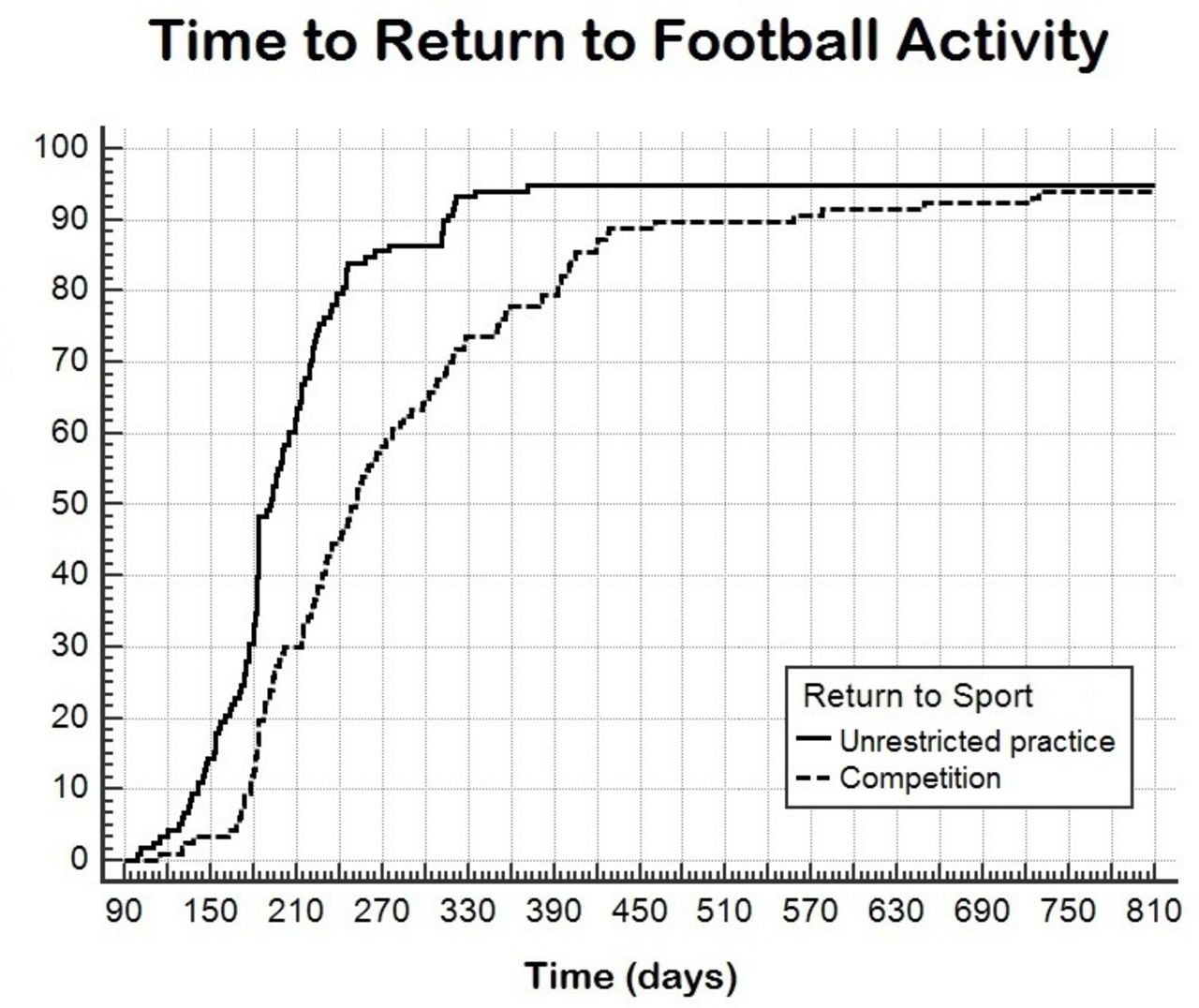
Progression of return to unrestricted practice (continuous line) and return to competition match (dotted line) after Achilles tendon rupture (ATR).

Progression of return to unrestricted practice and return to competition stratified based on participation of players at the international level (green line) or non-participation at the international level (blue line). Participation at the international level showed a faster return to unrestricted practice (log rank test p=0.0107) but no difference in return to competition (logrank test p=0.9203).

Progression of return to unrestricted practice and return to competition stratified based on players' role defined as goalkeeper (red line), defender (blue line), midfielder (yellow line) and forward (green line). The various roles showed a progression of return to unrestricted practice (log rank test p=0.3663) and return to competition (log rank test p=1.0000).
Multiple regression for time to return to unrestricted practice
Logistic regression for not returning to unrestricted practice
Return to competition
Except for one player who re-ruptured his Achilles tendon during training, all players who returned to training (previous section) participated in official competitions after ATR. The mean time from ATR to return to competition was 274±114 days, after a mean of 76±106 days from unrestricted return to play. No predictors were identified by Cox regression and multiple regression analysis (table 4).
Multiple regression for time to return to competition
Re-ruptures
Of the 71 athletes who played in at least two full seasons after return to play, six (8%) had a re-rupture. In five players the re-injury occurred during the first 3 months after return to unrestricted practice: one player during training without participating in an official match, one player during the first match after ATR, two players during their second and fifth appearances, and one 3 months after returning to unrestricted activity and 219 days after the primary ATR. Of these five early re-ruptures (within 3 months from return to unrestricted practice), four occurred in players with return to training <180 days and return to competition <200 days since ATR. However, no predictors of re-ruptures were identified by logistic regression analysis (table 5). A higher risk was noted for players participating in Second Division leagues (p=0.04).
Logistic regression for re-rupture
Another two re-ruptures were identified but were not included in the analysis because they occurred beyond the first two seasons after the players returned to training. Of the eight players who sustained a re-rupture, four made comebacks playing professionally but not at the previous level (mean age 26.2±3.3 years) and four retired (mean age 31.8±2.8 years).
Return to same level of activity
Overall, nine of the 71 players (13%) were not able to return to the same pre-injury level: three (4%) returned to play football in fourth division or at non-professional level, three (4%) retired a few years after ATR after playing a limited number of matches (<5) per season, and the other three players (4%) retired after re-rupture occurred within the first two seasons after return to play. If the five players who did not return to play after the primary rupture are also included, a total of 14/76 players (18%) were not able to return to the same pre-injury level of activity. Age >30 years at ATR had a significant OR of 4.46 (p=0.03) for not returning to the same level of play, while sustaining a re-rupture within the first two seasons had a significant OR of 6.37 (p=0.05) (table 6) (figure 5).

ORs of return to unrestricted practice, return to same pre-injury level of play and re-rupture for each of the independent variables: non-significant ORs are shown in blue and significant ORs are shown in red.
Logistic regression for not returning to same level of play
The number of matches played two seasons (p=0.10) and one season (p=0.25) before the ATR was similar for the players who returned to the same level of play and those who did not (figure 6). Also, the number of matches played the first season (p<0.01) and the second season (p<0.01) after return to play were significantly higher in those who fully resumed their level of play. In the 63 players who returned to the same level of play, the number of matches played in the first season after return to play was lower than the season before ATR (p<0.01) while the number of matches played in the second season after return to play was similar (p=0.06).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histograms of matches played during the two seasons before Achilles tendon rupture (ATR) (dark and light red) and the two seasons after return to play (dark and light blue), divided according to the players' ability or not to return to the same pre-injury level.
Discussion
Our study shows that 96% of male professional football (soccer) players returned to unrestricted practice after suffering an index ATR and having surgical treatment. Return to training and return to at least some participation in an official competition occurred after a mean of around 200 and 280 days (7 and 9 months), respectively.
Underscoring the serious nature of ATR is our novel finding, since 18% of this sample of professional players were unable to return to play at the previous level within two seasons of the injury. We also found that 8% of athletes who returned to play sustained an Achilles tendon re-rupture, with half of them retiring from their football playing careers. This is the first study to evaluate such outcomes in professional football (soccer) players. Our study population is the widest series of sport-specific athletes evaluated after ATR, despite using only publically available internet sources. The results of the present study, even though obtained differently from standard prospective follow-up studies, offer interesting insights for clinicians, athletes and coaches as we share prognosis data that should influence expectations after ATR in professional football (soccer) players.
Return to unrestricted practice
According to the online data, 96% of football players who sustained an ATR returned to unrestricted activity and were available for official competitions. This result is similar to that reported in the study on UEFA players10, where no sporting retirements were reported in the nine cases of ATR included. Also, a return to the pre-injury sport level of 91% was reported in a series of 36 professional athletes, 25 of whom were football players.9 A systematic review of 108 studies and 6506 patients reported a rate of return to play of 80%,8 lower than that found in the present study. This could be due to the variability of patients, definitions of return to sport and the larger proportion of recreational sport athletes in the systemetic review.
Regarding the time required to return to unrestricted activity, the average of 200 days is higher than the 161 days of the nine players in the UEFA cohort.10 This could be due to the different level of play of the included athletes. We identified participation in the national team as a predictor of faster recovery. It is reasonable to assume that these elite athletes have access to top-level care and have stronger motivations to recover, so the higher level of footall could infer a shorter return to play. However, on average, a lay-off from the team of 6–7 months should be considered a reasonable expectation for professional players after ATR. From our data we are unable to assess the role of test batteries, workload and psychology in the timing of return to sport, as suggested by Ardern and colleagues21 22 in the 2016 Bern Return to Sport Consensus statement.
Return to competition
All the players who returned to the team were able to participate in an official match, except for one player who had a tendon re-rupture. However, the return to competition occurred on average around 9 months after the injury and more than 2 months after returning to join the team. In the intervening period the players were involved with their respective squads and engaged in non-competitive games. This result shows that recovering the physical and mental fitness to compete in official matches is a slow process following ATR.
Cox regression and multivariate analysis did not identify any factors associated with the time to return to competition. Therefore, it is possible that other variables such as the summer season break and possible change of team could have affected the return to competition, even if not accounted for in the present analysis.
Return to same level of activity
When considering the athletes who returned to play two seasons after ATR, only 82% were able to perform at a level comparable to their pre-injury status. We defined this outcome as the ability to play at least five matches in a first or second National Division. We used this definition as we wanted to determine whether the player engaged in continuous participation in official competitions in a league similar to the pre-injury status, thus assessing the ability to continue to compete at a high level. Our definition did not take into account the possible passage from a more prestigious and ranked team to a lower level team, nor the sport-specific performance in terms of minutes played, scores, assists or the market value of the player. It is therefore possible that the percentage reported in this study could be lower if more specific performance-based definitions are used, as suggested in other sports3 12 13 or for other football injuries.14
A recent study with a similar design found that only 68% of National Basketball Association (NBA) players and 65.5% of National Football League (NFL) players returned to sport, defined as professional involvement in at least one game for at least two consecutive seasons.13 These results are lower than the 82% of professional footballers, even considering a less strict definition of return to sport (1 vs 5 matches). This difference is probably because of the different technical and physical tasks required in the two sports and also sport-specific physical characteristics of the athletes participating in them. It is possible that calf strength asymmetry, which affects athletes after ATR,11 20 23–25 is likely to compromise the physical demands required for basketball and American Football which include repetitive jumping, short sprints and the stop/start nature of the games, rather than the tasks required in football (soccer). Cultural differences in these sports may also play a role.
In our study, footballers aged >30 years and those who sustained a re-rupture were more likely not to return to the pre-injury level. Extreme care should therefore be used to prevent Achilles re-injuries for the benefit of the athlete’s health and career, while realistic expectations of not returning to the desired performance should be considered in athletes experiencing ATR in their 30s.
Finally, we note that footballers who successfully returned to play were able to participate in a number of matches similar to pre-injury status only the second season after returning to play. Therefore, the return to full performance after ATR represents a continuum that could take longer than 2 years.
The promising insights from the present findings should be confirmed in future studies aimed at prospectively evaluating well-defined and distinct outcomes such as return to play, return to the same level and return to performance.26 27
Re-ruptures
The 8% re-rupture rate reported in the present study is slightly higher than the rate of 4–6% reported in the general population after surgical Achilles repair.4 7 We speculate that this results from the demands placed on a player returning to play professional football. Interestingly, a higher re-rupture risk was reported in players participating in Second Leagues. Since Fanchini et al 11 reported the involvement of one physiotherapist, one athletic trainer, two team doctors and one surgeon consultant, plus expensive technologies such as GPS for the recovery of one Italian First Division player after ATR, it is possible that lower divisions are not able to guarantee such expensive and demanding standards. Moreover, several of the re-ruptures occurred during early rehabilitation or early return to sport, highlighting the risk of re-injury in the case of possible incomplete recovery, inadequate rehabilitation or overestimation of readiness. Half of the players who sustained a re-rupture finally retired from professional football. This event seriously threatens players' careers and our small numbers suggest it may be a career-ending injury in older athletes.
Study limitations
The main limitations of the study relate to the novel study design. We did not review the medical charts and we did not examine any of the patients in this study. As a result, we cannot comment on the type of surgery performed or the rehabilitation protocols which the players followed. However, we consider transfermarkt.com to be free from ascertainment bias, since the treating physicians are not involved in the collection of data and analysis of the results.
We acknowledge the possibility of other bias such as incorrect medical data (see below) as this is provided by non-medical journalists and cannot be ratified because of privacy regulations. There may be errors in how those who provide the data to transfermarkt define return to full training, the inability for our team to clean data and possible under-registration of ATR (eg, if coded as a calf strain). However, the use of the same source to gather the data (eg, transfermarkt) and the application of consistent definitions of return to sport would be helpful to compare the burden of different injuries and sports.
Another important limitation is represented by the sparse data bias, since the results of logistic regression analyses produced large OR estimates and 95% CIs. This is due to the small numbers in the study for several variables, so ORs should be interpreted with caution. Moreover, the limited numbers of events regarding inability to return to play and re-rupture could be responsible for the lack of siginifcant predictors in the multivariate analysis, which could have been underpowered.
Conclusions
Almost every professional football (soccer) player was able to return to unrestricted practice and competition after a mean of 7–9 months; complete recovery to full and continuous match participation could be delayed for up to two seasons. Only 82% of players were still competing at a similar pre-injury level during the two following seasons. Older players (aged >30 years) who ruptured their Achilles tendon were more likely to retire than younger players (aged 27) who sustained the injury. Our data will allow physicians and athletes to base their shared decision-making discussions around more reliable ATR prognosis data. This should help to set reliable expectations after the injury.
What are the new findings?
96% of professional male footballers returned to play after Achilles tendon rupture and repair.
On average, players returned to sport fully and participated in official competitions at around 7–9 months; international level athletes had faster recovery rates.
Re-ruptures occurred in 8% of footballers, especially in those who returned to play before 6 months.
In those aged >30 years of age or who suffer a re-rupture, Achilles tendon rupture (or re-rupture) is a potentially career-ending injury.
How might it impact on clinical practice in the future?
Our data provide clinicans, coaches and atheletes with a realistic prognosis associated with Achilles tendon rupture in professional footballers. Our results suggest caution in return to sport within 6 months of Achilles tendon repair surgery because of the relatively high number of re-rupture cases in this group.
References
Footnotes
Contributors AG conceived the study design. GR and AG performed the search. AG and MM performed the data analysis. AG and RA wrote the manuscript. KS and PDH crticially reviewed the manuscript and performed language editing. SZ supervised all the phases of the development of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.