Article Text

Abstract
Injury and illness surveillance, and epidemiological studies, are fundamental elements of concerted efforts to protect the health of the athlete. To encourage consistency in the definitions and methodology used, and to enable data across studies to be compared, research groups have published 11 sport-specific or setting-specific consensus statements on sports injury (and, eventually, illness) epidemiology to date. Our objective was to further strengthen consistency in data collection, injury definitions and research reporting through an updated set of recommendations for sports injury and illness studies, including a new Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist extension. The IOC invited a working group of international experts to review relevant literature and provide recommendations. The procedure included an open online survey, several stages of text drafting and consultation by working groups and a 3-day consensus meeting in October 2019. This statement includes recommendations for data collection and research reporting covering key components: defining and classifying health problems; severity of health problems; capturing and reporting athlete exposure; expressing risk; burden of health problems; study population characteristics and data collection methods. Based on these, we also developed a new reporting guideline as a STROBE Extension—the STROBE Sports Injury and Illness Surveillance (STROBE-SIIS). The IOC encourages ongoing in- and out-of-competition surveillance programmes and studies to describe injury and illness trends and patterns, understand their causes and develop measures to protect the health of the athlete. Implementation of the methods outlined in this statement will advance consistency in data collection and research reporting.
- consensus statement
- epidemiology
- injuries
- illness
- methodology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Injury and illness surveillance, and epidemiological studies are fundamental elements of concerted efforts to protect the health of the athlete. Carefully designed injury surveillance programmes, accurate data capture and careful analysis of data are building blocks for sports injury/illness prevention programmes. Important questions that sports injury and illness surveillance projects are designed to address include: What is the risk of an individual athlete sustaining an acute injury, developing an overuse injury or becoming ill in a given sport? Within a given sport, what is the typical pattern and severity of injuries and illnesses? How do injury rates in various sports compare? Do participant characteristics and factors within competition and training affect risk?
To encourage consistency in the definitions and methods used, and to enable data across studies to be compared, research teams have published 11 consensus papers on sports injury (and, eventually, illness) epidemiology. Most of them addressed specific sports—cricket,1 football,2 rugby union,3 rugby league,4 aquatic sports,5 tennis,6 athletics7 and horse racing.8 Two statements covered multisport events9 and mass-participation events (eg, marathon races).10
We now have more than a decade of experience with the existing recommendations. Sports epidemiology has advanced—with a new focus on overuse injuries and also on illnesses. Data collection and reporting methods have also advanced as data are being collected for routine surveillance or predefined observational or intervention studies in diverse settings, ranging from community to elite sports, from youth sports to the master’s level, in able-bodied and athletes with disabilities and in team sports and individual sports. In 2005, when the first of these sports injury surveillance consensus statements was developed, there were no agreed on research reporting methods (eg, the EQUATOR Network was just holding its inaugural meeting). Many important research epidemiological issues were not discussed in any of the previous sport-related consensus statements.
In 2019, the IOC convened an expert panel to update recommendations for the field of sports epidemiology—this consensus statement. We drew on recent methods developments and the experience of scientists working in the field of sports injury and illness surveillance. A specific goal was to further encourage consistency in data collection, injury definitions and research reporting (in line, where possible, with the EQUATOR network recommendations). Our aim was to provide hands-on guidance to researchers on how to plan and conduct data collection and how to report data. We anticipate that this sports-generic statement will be complemented by subsequent sport-specific statements with more detailed recommendations relevant for the sports and/or setting. We also extended the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist,11 the STROBE-Sport Injury and Illness Surveillance (STROBE-SIIS), to assist users in planning surveillance studies, and in writing papers based on injury/illness data.
Methods
This was an eight-stage process: (1) an online survey; (2) working groups reviewed the survey responses, available literature and drafted text; (3) all consensus group members reviewed the draft text; (4) the initial working groups revised their draft text; (5) a 3-day consensus meeting was held in Lausanne, Switzerland (9–11 October 2019); (6) new working groups revised the draft text; (7) an editorial group (RB, KC, BR, KMK) made final edits; (8) all authors reviewed and approved the final draft.
The IOC Medical and Scientific Department appointed RB to chair the consensus group. He selected a consensus group that included at least one author from previous consensus statements on sports injury epidemiology. Care was taken to include experts with research experience from diverse settings (sports types, age groups, performance levels) and with a variety of health problems as outcomes (eg, illness, not only acute injuries).
Online survey: the survey included 25 questions inviting free-text comments on aspects identified from previous consensus statements. The survey link was open to the public and was launched via email and Twitter on 1 February 2019 and closed on 15 March 2019. We received comments from 188 respondents, including 19 consensus group members. A report including all responses was distributed to the consensus group on 31 August 2019.
The consensus group was split into seven working groups. Each working group was responsible for a subset of the sections presented in this final document (eg, ‘classifying health problems’). For each section, the group reviewed the survey responses, examined available relevant literature (including previous consensus statements) and composed draft text with necessary background and proposed definitions and recommendations.
RB created a complete draft which was shared online with the consensus group, asking all members to provide written comments/suggestions. Comments were made online and visible to all group members.
The working groups revised their sections based on input from other members of the consensus group.
At the in-person consensus meeting, attended by all consensus group members, the revised draft was discussed section by section, focusing on recommendations and definitions.
Seven new revision groups made up of those not responsible for drafting the original section under discussion were responsible for taking notes and revising the text. If necessary, items were voted on to achieve a majority.
The revised draft was edited for consistency and form by RB and reviewed with the rest of the editorial group (KC, BR, KMK).
Finally, the manuscript was distributed to the consensus group members for final approval.
Defining and classifying health problems
Terminology for health problems
WHO defines health as ‘a state of complete physical, mental and social well-being’ and not merely the absence of disease or infirmity.12 Extending this definition, Clarsen et al 13 defined an athletic health problem as any condition that reduces an athlete’s normal state of full health, irrespective of its consequences on the athlete’s sports participation or performance or whether the athlete sought medical attention. This constitutes an umbrella term that includes, but is not limited to, injury and illness.
Health problems can have several consequences. A health problem that results in an athlete receiving medical attention is referred to as a ‘medical attention’ health problem, and a health problem that results in a player being unable to complete the current or future training session or competition as a ‘time-loss’ health problems.1 3–5 7 14 As not all health problems limit an athlete’s ability to participate nor require medical attention, broader definitions (self-reported, symptom-based or performance-based) will capture more health problems. Figure 1 illustrates these differences.

Distribution of health problems by consequences (not to scale). Adapted from Clarsen and Bahr.84
Defining injury and illness
Previous consensus statements on injury and illness in sport have proposed largely consistent definitions for injury and illness.1 3 5–10 14 15 Differences in definition stem from the specific sport or context for which statements were developed. For this consensus statement, we define injury and illness as follows:
Injury is tissue damage or other derangement of normal physical function due to participation in sports, resulting from rapid or repetitive transfer of kinetic energy.
Illness is a complaint or disorder experienced by an athlete, not related to injury. Illnesses include health-related problems in physical (eg, influenza), mental (eg, depression) or social well-being, or removal or loss of vital elements (air, water, warmth).
We acknowledge that there is not always a clear distinction between injury and illness. The consensus was that for injury, the primary mode involves transfer of kinetic energy, but other types of injury, such as sunburn or drowning, may have a different aetiology.
These definitions are meant to be inclusive; they embrace a broad array of injury-related and illness-related health problems that may affect an athlete. Depending on the goal of the monitoring activity, data recording may be limited to specific health problems that constitute a narrower subset of the above definitions (ie, via an operational definition). If the surveillance programme has a narrow scope (eg, to capture only concussions in school rugby), data recording can be limited to the specific injury type of interest.
Relationship to sports activity
Health problems may result:
directly from participation in competition or from training in the fundamental skills of a sport (eg, players colliding in a match, overuse from repetitive training or transmission of a skin infection from contact with another player);
indirectly from participation in activities that related to competition or training in a sport, but not during competition or a training session (eg, slipping, falling and sustaining an injury when in the Olympic village, developing an illness following international travel to a competition or an illness deemed to be related to an increased training load over a few weeks);
from activities that are not at all related to participation in sport, that is, would occur in the absence of participation during competition or training in the fundamental skills of a sport (eg, car crash, sudden cardiac arrest at home).
Depending on the purposes of the study, researchers may want to report health problems in these categories separately.
Mode of onset
Traditionally, health problems have been classified into those that have a sudden onset and those that have a gradual onset. Sudden-onset health problems were considered to be those that resulted from a specific identifiable event (eg, a collision between an athlete and an object causing a fracture). Gradual-onset problems, on the other hand, were considered to be those that lack a definable sudden, precipitating event as the onset (eg, a tendinopathy induced by repetitive movement).
The term ‘overuse injury’ is commonly applied to gradual-onset injuries. However, this term is used inconsistently in the literature16 17 and most injury surveillance systems do not define ‘overuse injury’.16
Health problems may have elements of both sudden onset and gradual onset. For example, a long-distance runner with an intensive training regime may have insufficient recovery, resulting in cumulative stress-related changes to the bone, but presenting as an acute tibia fracture without prior pain. The dichotomy between sudden onset and gradual onset, which most methods of data capture are based on, means such important nuances may be missed. One option to address this problem would be to classify health problems based on the underlying pathology, whether this indicates a single or repetitive pathogenic mechanism, based on imaging studies (eg, MRI, ultrasound) or tissue biopsies. However, routine capture of such detail in a reliable manner within a surveillance system is challenging.
Mode of onset—injury
For injuries, classical epidemiology provides a solution for this issue by viewing health problems as the result of a series of interactions between agent, host and environment.18 19 Injury epidemiology adapted this model by defining kinetic energy as the ‘agent’ of injury.20–22
In this paradigm, following the definition above, injury results from a transfer of kinetic energy (agent) that damages tissue. Injury may result from a near-instantaneous exchange of large quantities of kinetic energy (eg, as in a collision between athletes), from the gradual accumulation of low-energy transfer over time (as in the bone stress injury example) or from a combination of both mechanisms (repetitive training regime resulting in tendon weakness that then manifests itself acutely as a tear from acceleration forces applied during a single jump). This model suggests mode of onset for injuries should be conceptualised as a continuum interplay of energy exposures.
Mode of onset—Illness
Illnesses, like injuries, may be either associated with a specific precipitating event (eg, a player ingesting a toxin from food and suffering gastrointestinal illness that manifests within hours of exposure) or they may involve a progressive pathway that cannot be linked to a specific precipitating event (eg, progressive fatigue from increased training load). Similarly, the timescale for sudden-onset illness can be seconds and minutes (eg, acute anaphylaxis) or develop within hours after exposure to a pathogen or a toxin (eg, gastroenteritis) or even days or weeks (eg, upper respiratory tract infection).
The mode of onset for illnesses may also be related to a specific event, with or without some underlying subclinical pathology. For example, myalgic encephalomyelitis will typically present without a precipitating event, whereas influenza usually has a point source of exposure (although this may be difficult to trace). As with injuries, many illnesses reflect both underlying pathology and a sudden-onset event (eg, an athlete may be predisposed to bronchial hyper-reactivity, and this may present acutely as bronchoconstriction when exposed to air pollution at a venue).
Classifying mode of onset
We recommend that injury/illness surveillance discontinue use of sudden onset and gradual onset as a simple dichotomy and implement methods that capture relevant subtleties. We encourage researchers to develop and use measures that will help identify injuries and illnesses that involve mixed acute and repetitive mechanisms. Data collectors should consider whether a health problem results from a clear acute mechanism, clear repetitive mechanism or appears to include a mix of both elements (table 1). Examples 1 and 3 in table 1 reflect clear acute and repetitive aetiology, respectively, whereas example 2 represents a mixed aetiology.
Examples: assessment of mode of onset
Classifying the mechanism of injury
Mechanism of onset has typically been defined only in the context of sudden-onset injuries. Sudden-onset health problems can result from contact and non-contact mechanisms; this classification is discussed below and presented in table 2.
Examples: classification of contact as a mechanism for sudden-onset injury
Direct contact mechanisms directly lead to the health problem in an immediate and proximal manner.
Indirect contact mechanisms also stem from contact with other athletes or an object. The force is not applied directly to the injured area, but contributes to the causal chain leading to the health problem.23–26
Non-contact mechanisms are those that lead to health problems without any direct or indirect contact from another external source. Gradual-onset injuries, by their nature, are non-contact.
We anticipate that subsequent sport-specific consensus statements will provide more detailed subclassifications to address specific features of contact mechanisms (eg, subclassification of contact with objects, such as ball, bat, net, gate). Future sport-specific statements may also give specific recommendations on other categories for classification related to injury causation (eg, rule infringements, particular movements or other sport-specific features). The International Classification of Disease (ICD) External Causes Chapter27 and the International Classification of External Causes of Injury28 provide specific codes that might be useful.
Multiple events and health problems
One of the particular features of sports epidemiology, compared with other settings, is the relatively high chance that an athlete will sustain more than one health problem over the follow-up period. This is illustrated in figure 2.

Examples of hypothetical prospectively collected injury/illness data (adapted from Finch and Marshall).114 The X indicates when a period of surveillance is ended because the athlete left, unrelated to health problems, before the end of the study period; this is called censoring.
The relatively common occurrence of multiple health problems in a single individual poses challenges for the reporting and analysis of sports injury and illness data.29 In particular, note that the number of athletes in a study is unlikely to be the same as the number of reported health conditions and both should be stated. When reporting the frequency (or proportion) of specific diagnoses or other characteristics, it is important to state clearly whether this is expressed as the proportion of all athletes followed up or the proportion of all injured athletes or the proportion of all reported injuries.
Subsequent, recurrent and/or exacerbation of health problems
Was a subsequent health problem related to previous health problems? This is an important question in the field. To know whether health problems follow previous health problems requires both sets of problems to be classified correctly using consistent terminology. This exercise can provide greater insight into the etiological factors that underpin subsequent health problems.30
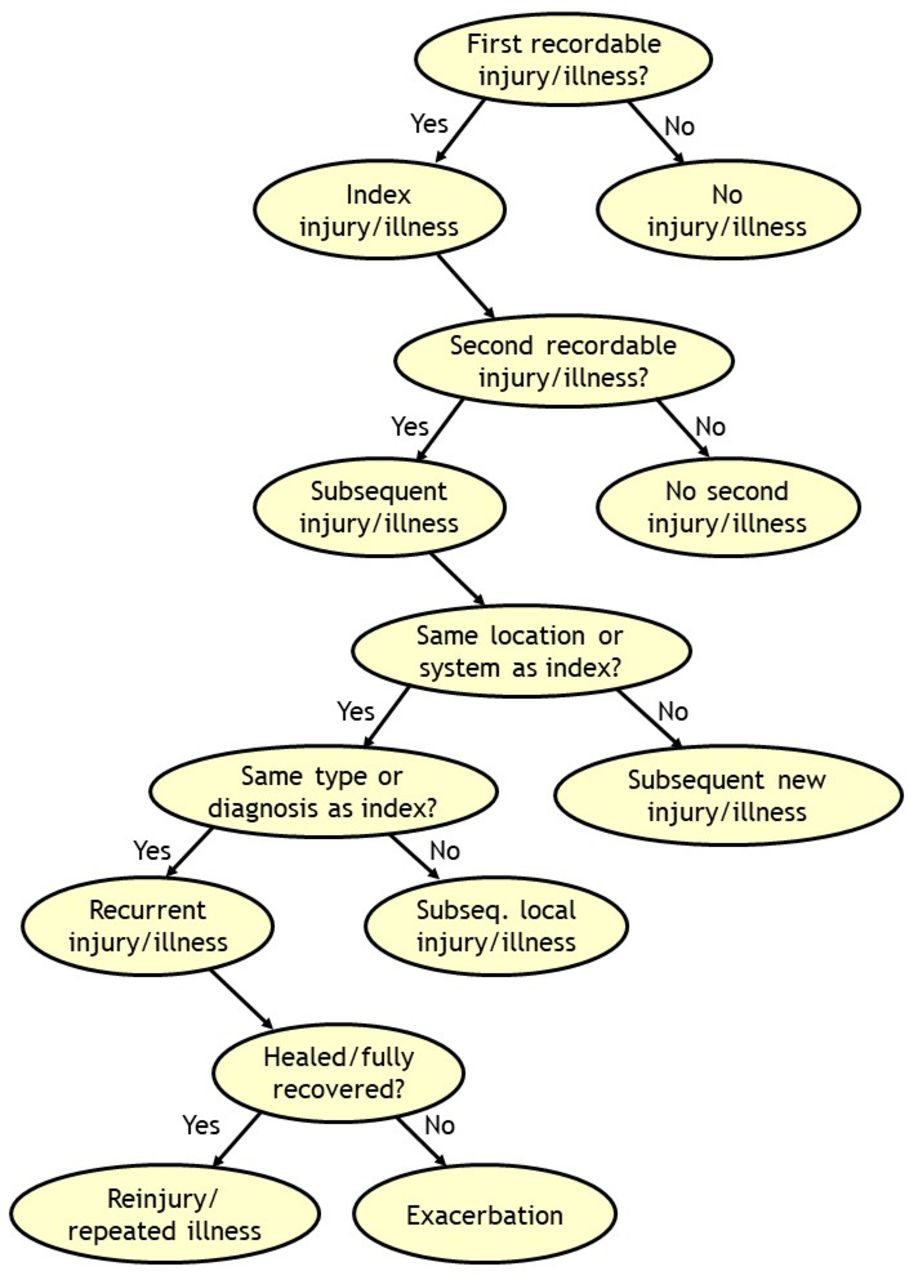
Hamilton et al 31 provided a useful framework to categorise subsequent injuries/illnesses and exacerbations in sport (figure 3). More recent frameworks incorporate extensive criteria30 32 33 that require judgement by trained clinicians, which may be beyond the scope and capacity of many surveillance protocols. When reporting frameworks become more complex, there is a greater risk of data errors.34 In general, we do not recommend complex frameworks but they can be considered for sophisticated data collection and analysis where appropriate expertise and resources exist.

Classification tree for subsequent health problems (adapted from Hamilton et al 31). Definitions: (1) index injury (illness)=the first recorded injury (illness), (2) subsequent injury (illness)=any injury (illness) occurring after the index injury (illness) ((i) subsequent injury to a different location than the index injury (subsequent illness involving a different system than the index illness); (ii) subsequent injury to the same location but of a different tissue type than the index injury (subsequent illness of involving the same system but of a different type/other diagnosis) or (iii) subsequent recurrent injury (illness)=subsequent injury to the same site and of the same type as the index injury (subsequent illness involving the same system and type as the index illness). Third, fourth or more health problems should be assessed relative to the initial index health problem and all other previous ones (eg, second and third health problem).
The recommended subsequent injury terminology, adapted from Hamilton et al,31 includes noting whether subsequent injuries: (i) affect the same site but other tissues (eg, knee but meniscus instead of ACL alone) or (ii) affect other sites. Subsequent illness terminology31 notes whether the subsequent illnesses is the same system (eg, respiratory) but other diagnosis (eg, bronchospasm as distinct from a viral illness) or to other systems. The relevant definitions are shown in figure 3. Note that an injury may be subsequent to an illness and vice versa (eg, bones stress injury following diagnosis of an eating disorder, depression following a lengthy recovery after revision ACL reconstruction).
Subsequent injuries to the same location and tissue as the index injury are recurrences if the index injury was healed/fully recovered; they are exacerbations if the index injury was not yet healed/fully recovered. Subsequent illnesses to the same system and type as the index illness are recurrences if the individual has fully recovered from the index illness, and exacerbations if the individual has not yet recovered from the index illness. Healed/fully recovered from injury (or illness) is defined as when the athlete is fully available for training and competition (see ‘Severity of health problems’ section).
To illustrate how to classify subsequent injury, consider athlete ‘A’ who, following an ACL rupture and surgical reconstruction, presents late in the rehabilitation period, before return to play, with swelling and pain in the knee after a slip and fall injury resulting in a graft tear. This injury would be classified as an exacerbation of the index injury. In contrast, athlete ‘B’ rehabilitated successfully after an ACL reconstruction and returned to play; that player presents with pain and swelling in the same knee. If the diagnosis is a torn ACL graft, this would be classified as a recurrent injury. If the diagnosis is a meniscal tear (ACL graft intact), this is a local subsequent injury.
To illustrate how to classify subsequent illness, consider athlete ‘C’ who has withdrawn from sports participation due to an upper respiratory tract infection caused by influenza type A virus, which then progresses to a lower respiratory tract infection resulting in a diagnosis of viral pneumonia. As athlete ‘C’ is diagnosed with pneumonia before recovery and return to play, the diagnosis of pneumonia is an exacerbation of a recurrent illness. In contrast, athlete ‘D’, following full recovery from the upper respiratory tract infection and return to play, is diagnosed with pneumonia; this illness is a subsequent new illness.
Time to recurrence or exacerbation should be recorded in days (see ‘Severity of health problems’ section).
A minimum list of data items recommended when collecting information on subsequent injury or illness is shown in table 3.
Recommendations for key data items that should be collected and reported on in surveillance systems to enable multiple and subsequent injuries/illnesses to be monitored (modified from Finch and Fortington115)
Classifying sports injury and illness diagnoses
Injury and illness classification systems are used in sports medicine to:
Accurately classify and group diagnoses for research or reporting, allowing easy grouping into parent classifications for summary, so that injury and illness trends can be monitored over time or injury or illness incidence or prevalence can be compared between groups (eg, different teams, leagues, sports, sexes), potentially leading to risk factor and preventive studies.
Create databases from which cases can be extracted for research on particular or specific types of injuries and illnesses.
In the late 1980s, clinicians and researchers were using the ninth edition of the ICD.27 The ICD system is an important international standard, yet even the 11th edition, released in 2018, lacks some classifications important in sports injury and illness surveillance. Hamstring strain and exercise-associated postural hypotension are two examples.35–37 We encourage developers to include more sports medicine diagnoses in future revisions of the ICD.
In the early 1990s, in Canada and Australia, two alternate diagnostic coding systems were developed specifically for sports medicine and these have flourished into the most widely used systems in sports injury surveillance in the world today. Their ‘open access’ nature has allowed other researchers to use them free of charge (with acknowledgement). These diagnostic coding systems are the Sport Medicine Diagnostic Coding System (SMDCS) and the Orchard Sports Injury Classification System (OSICS). Both are based on initial codes to represent body area and further codes to represent injury type or pathology.
One advantage of these coding systems is that they are less cumbersome to apply than ICD codes, especially when built into electronic systems with drop-down menus taking advantage of the body area and tissue-type/pathology-type categories. The full ICD-11 coding system includes 55 000 codes, of which the majority are not relevant in sports medicine, compared with 750–1500 codes for versions of the SMDCS and OSICS.
When reporting aggregate injury data, we recommend using the categories for body areas (table 4) and tissue types and pathologies (table 5) outlined below. Table 6 illustrates how injury data can be reported using these categories. In addition, categories for organ system/region (table 7) and aetiology (table 8) are presented below for illnesses.
Recommended categories of body regions and areas for injuries
Recommended categories of tissue and pathology types for injuries
Data on the injury pattern and burden of specific match injuries among professional rugby teams in New Zealand (2005–2018, unpublished data).
Recommended categories of organ system/region for illnesses
Recommended categories for aetiology of illnesses
When recording injuries or illnesses, the diagnosis should be recorded in as much detail as possible given the information available and the expertise of the individual reporting. Acknowledging that some studies will rely on athlete self-report, or proxy report by parents, coaches or other non-medically trained staff, this consensus group also suggest categories to guide reporting of illnesses (table 9). When injury data are reported by athletes or non-medical staff, we recommend that reporting is limited to body area, as their reporting of tissue type and pathology is unreliable.38
Recommended categories of illness symptom clusters for athlete self-report or non-medical data reporters
To facilitate reporting based on diagnostic codes, a companion paper has been written with a supplemental Excel data file that provides a full list of revised SMDCS and OSIICS (Orchard Sports Injury and Illness Classification System) codes, along with a translation between both systems and the ICD system.39
Injuries—body area categories
Wherever possible, we tried to define body areas anatomically as either joints or segments. However, we made exceptions based on common clinical presentations in sport where needed. For example, hip/groin is an area we have defined, which is a combination of joint and part of a segment, and therefore not a singular anatomical region.
When one injury event results in more than one injury, the individual diagnoses should be recorded and classified separately. However, for injury incidence and prevalence reporting purposes this will be counted as one injury, and severity should be reported as the severity of the principal (most severe) injury (see below for further explanation).
Injuries—tissue-type and pathology-type categories
Using consensus methodology, we compared the ‘injury-type’ codes from the OSICS and SMDCS systems to arrive at definitions of injury types. We constructed this table to be a single table reflecting ‘injury types’ (as per OSICS) but split two columns into ‘tissue’ (as the broad area) and then ‘pathology’ type more specifically. This reflects the original approach taken in the SMDCS.
Recommendations: reporting injury characteristics
Injury characteristics are often reported in one table by region, one by injury type or both. Cross-tabulations depicting data by region and injury type, that is, combining the two into one table, often become large and unwieldy. It can leave many cells empty or with very few cases (which can then compromise confidentiality), unless the dataset is unusually large. Such tables often also provide insufficient information for research focused on specific areas or sports. For example, in a sport where knee sprains dominate, it may be desirable to report subgroups of these (eg, ACL, medial collateral ligament) at greater detail.
In many cases, a better reporting option is to combine region and type and diagnosis in one table such as in the example shown in table 6, where some categories have been collapsed at the level of body region (bold), some regions have been split further into injury types (subheader) and some even at the level of specific diagnosis (italics). It is expected that subsequent consensus statements on specific sports will provide recommendations on suitable, standard formats for each sport, to facilitate direct comparison of data on key injury types from studies on the same sport.
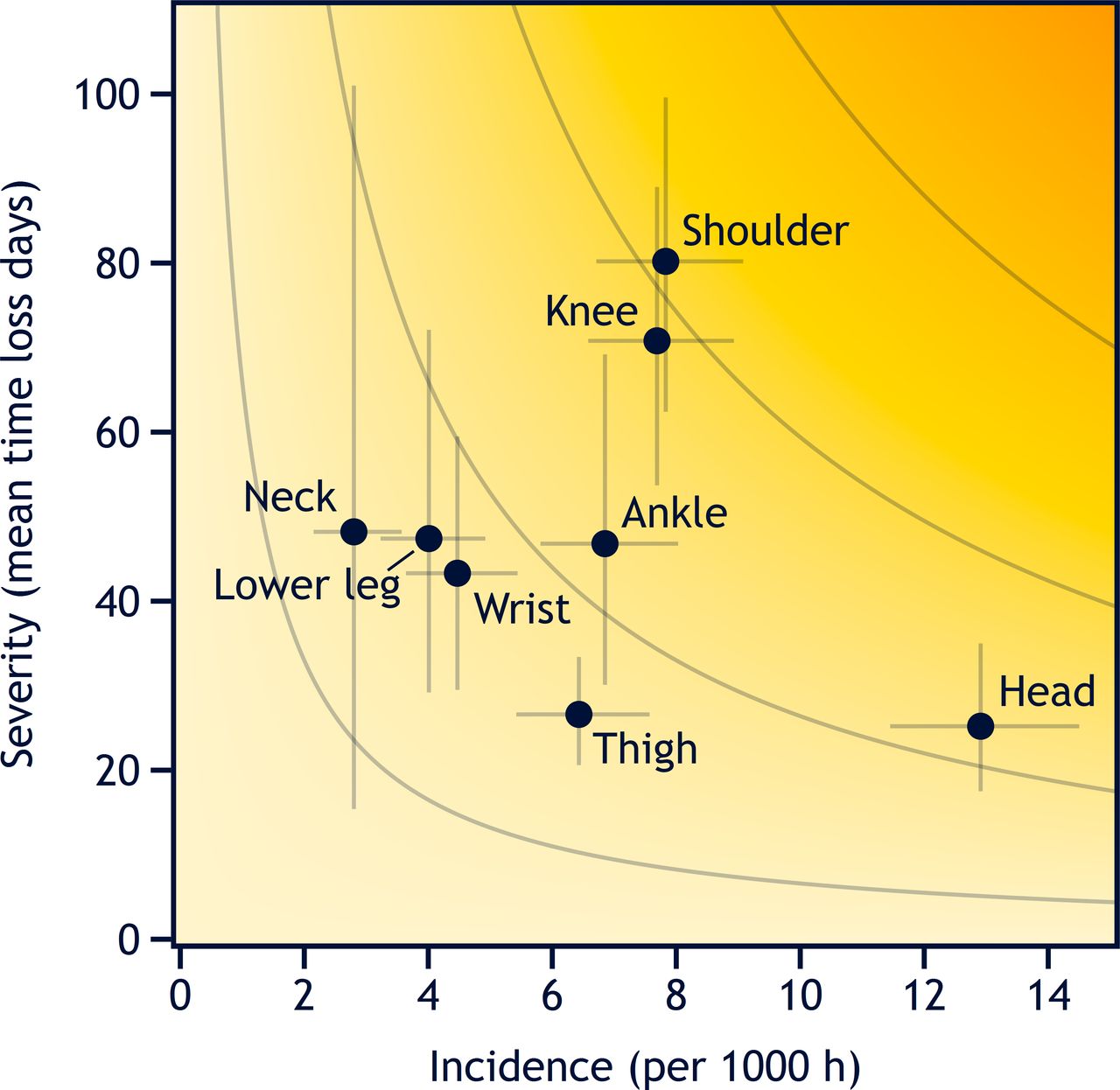
Risk matrix based on the duration of time loss illustrating the burden of match injuries among professional rugby teams in New Zealand between 2005 and 2018 (unpublished data). The darker the yellow, the greater the burden. The curved grey lines represent point with equal burden. The vertical and horizontal error bars represent 95% CIs. See also table 6, illustrating the same dataset in more detail.
Illness—categories for organ system and aetiology
Illness consensus categories are presented in tables 7 and 8. These are more detailed than the original versions of the SMDCS and OSICS. Our tables diverge from the ICD categorisation format, in which body systems and pathology types are grouped together. We believe that it is important to recognise that an illness, like an injury, affects both a body system and has a specific pathological type. A respiratory infection does not need to be considered either only as a respiratory condition or an infection, it is certainly both. Our recommended illness systems are similar to many of those in the ICD, but we have merged some systems, such as the upper respiratory system and nose/throat.
The professional background of those who report health data will influence the final data quality (see ‘Data collection methods’ section).40 When athletes themselves (or non-clinical recorders like coaching staff) are asked to capture illness data, they should be encouraged to record symptoms rather than attempt a diagnosis. Table 9 lists symptom clusters that are characteristic of various systems. We caution that this table requires additional validation and may be modified in future. Mapping symptoms to bodily systems sacrifices some accuracy; however, in circumstances where expert recorders are unavailable, it is better to have general systems diagnosis data than no data at all.
Recommendations: reporting illness characteristics
As was the case when we discussed reporting of injury data, we recommend against illness data being reported as cross-tabulations of organ system by aetiology type. A better option is to combine system/region and aetiology in one table, as in the example on injuries shown in table 6. Depending on the illness pattern of the sport/setting, some region categories may be collapsed, others split further into aetiology type and even to the level of specific diagnosis (where available), to highlight the most significant illnesses. We expect that subsequent sport-specific consensus statements will recommend useful standard formats for each sport.
Severity of health problems
The severity of health problems in sport can be described using various criteria.41–43 These include the duration of the period for which an athlete is unable to train/play (called ‘time loss’), the athlete’s self-reported consequences (various patient-rated measures of both health and sports performance), the clinical extent of illness/injury and societal cost (economic evaluation). When considering which severity criterion to use, investigators should consider the strengths and limitations of each approach related to the objectives of their study or surveillance programme.
Time loss from training and competition
The most widely used severity measure in sports medicine is the duration of time loss. It was recommended in previous consensus statements,3 5–8 44 and is relatively simple to capture, even when data collectors are non-expert—coaches, parents or athletes themselves.
When using this approach, we recommend that investigators record severity as the number of days that the athlete is unavailable for training and competition, from the date of onset until the athlete is fully available for training and competition.
The number of time-loss days should be counted from the day after the onset that the athlete is unable to participate (day 1), through the day before the athlete is fully available for training and competition. Therefore, cases where an athlete does not complete a particular competition or training session, but returns on the same or following day, should be recorded as 0 days of time loss (see table 10 for examples). We note that in some cases, time loss does not follow immediately after the health problem occurred and may be delayed and/or intermittent (table 10).
Practical examples of how to calculate time loss
When athletes recover from health problems during periods with no planned training or competition (eg, during an end-of-season break), investigators should record the end date as when the athlete normally would have been ready for full training and competition participation.
When aggregating data across athletes, report severity as the total number of time-loss days, together with median and quartiles. Means and SD should be interpreted with care, given that the distribution of time loss days is likely to be right-skewed.
When reporting data separately in severity categories, we recommend using the following time bins: 0, 1–7 days, 8–28 days,>28 days.
If one injury event results in multiple injuries, injury severity should be based on the injury leading to the longest time loss (eg, if a downhill skier crashes and suffers two injuries, a concussion which takes 10 days to resolve and a tibia fracture which takes 120 days, time loss for the event is 120 days).
Health problems contracted during multiday events
After athletes have left an event, it may be difficult to obtain accurate follow-up information on their condition and return to play. For cases that were not closed by a date of return to play at the time of the end of the event we recommend that:
If the researcher can liaise with team medical staff and record the actual date of return to play, this information should be captured. Collecting actual dates is recommended.
If this is not possible, then team medical staff should be asked to provide an estimate of when the athlete is expected to return to play. In such case, this information should be clearly labelled as an estimated severity.
If this is not possible, then event medical staff should record the date that the athlete leaves the tournament, that is, the last date on which the athlete was seen with the unclosed health problem. In such case, the information should clearly be labelled as a right-censored injury duration (a statistical term for situations in which only a portion of the time loss can be observed).
Limitations of using time loss to measure severity
Time loss generally reflects injury severity but has limitations. First, the demarcation between the end of time loss and the resumption of ‘normal training and competition’ is not necessarily a clear line in the sand. In some sports, athletes may be able to participate before an injury or illness has fully resolved, for example, by adapting technique, accepting a lower performance level or playing a different role in a team (eg, a ballet dancer working at the barre but not dancing on the floor or doing any jumps). Participation before an injury or illness is fully resolved would tend to ‘underestimate’ the absolute severity of the injury if one considered full healing as the gold standard. Conversely, athletes may choose not to resume their ‘normal’ training and competition for an extended period after an injury or illness has clinically resolved to allow them to regain full fitness (eg, a professional football player after ACL reconstruction). This would overestimate the severity of the condition.
Second, a time-loss-based severity measure underestimates the severity of those health problems that limit a player’s performance but do not stop the person playing. Many gradual-onset injuries fit that bill (eg, patellar tendinopathy). Similarly, when athletes have a recurrent or chronic illness, such as asthma or inflammatory arthritis, they may have a relatively low time loss (from training, competition), but they may be markedly affected in training content and intensity.45–47
Third, time loss is inappropriate to describe the most severe types of health problems such as those leading to retirement from sport, permanent disability or death because the time loss data from those injuries is right-censored.
Athlete-reported symptoms and consequences
There are tools to measure injury and illness symptoms that directly address the second limitation of time loss discussed earlier, underestimating the effect of ongoing pain and symptoms that are below the time-loss threshold. A tool such as the Oslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H) complements time-loss measures of severity, as it also captures symptoms and functional consequences of injury and illness. This purpose-built instrument was devised in 201345 and updated in 2020,13 and has played an increasing role in sports injury and illness surveillance, especially in sports and settings where overuse injuries and illnesses represent a substantial burden on health and performance.48
The tool (which can be delivered via a mobile app) invites athletes to record reduced sports participation, training modifications, performance reductions and symptoms.45 Based on the response to these questions, researchers can calculate a severity score ranging from 0 to 100 at specific time points. These can be aggregated (summed as the area under the curve) to monitor injury and illness over time (figure 4). This is called the cumulative severity score. A limitation of this method is that severity score is an arbitrary number and it has not been thoroughly validated as a proxy for injury severity.

Example of severity scores being used to track the severity of three ‘typical’ health problems. Each black dot represents the weekly severity score. The area in orange represents a gradual-onset injury (cumulative severity score (the sum of weekly scores, the area under the curve): 1820), the black area represents a short-duration illness (100) and the dark red area represents an acute medial collateral ligament injury (362).45
Recording the severity of health problems based on clinical assessment
Investigators may also report the severity of health problems based on clinical outcomes such as the need for hospitalisation or surgery,10 42 retirement from sport, permanent disability, or death.10 49
Degree and urgency of medical attention
The severity of an injury or illness can also be recorded based on the degree and urgency of medical attention received by the athlete. This approach is best suited to recording acute conditions, and it is often used in mass-participation events and community sport settings.42 50 51 An example using this approach is provided by Schwellnus et al 10 in their statement on mass community-based endurance sports event.
Permanent disability and death
All conditions leading to permanent disability or death that occur during the period of data collection should be reported separately. There are some specific definitions accepted in the field:
Catastrophic injury refers to a confirmed spinal cord or traumatic brain injury resulting in permanent functional disability (using American Spinal Injury Association (ASIA scale)52 and assessed at 12 months). This does not include injuries resulting in transient neurological deficits such as burners/stingers, paraesthesias, transient quadriplegia or cases of concussion where there is full recovery. The term catastrophic events has also been extended to include non-injury events that are life-threatening, such as sport-related sudden cardiac arrest and exertional heatstroke53; more detailed recommendations on this issue are provided in the consensus statement on mass community-based endurance sports events.10
Fatality: any athlete fatality related to training or competition. When fatalities occur months or years after the event, researchers should justify the relationship to training/competition.49 54
As such cases often receive media attention, we remind investigators to consider privacy issues. Special considerations apply to approaching, consenting and collecting data from families who have sustained a major loss.
Other severity measures
Depending on the sport setting and the purpose of data collection, investigators may also quantify severity in other ways.41 Function, performance and patient-reported outcome measures may be used to capture severity. Specific examples include:
Functional measures, for example, International Classification of Functioning, Disability and Health.55
Sports-related performance measures, for example, balance, strength and endurance. We include athletes reporting retirement from sport in this category.
Patient-reported outcome measures, for example, ACL Quality of Life questionnaire,56 Knee injury and Osteoarthritis Outcome Score57 and Sport Concussion Assessment Tool.58
Capturing and reporting athlete exposure
Assessing exposure is fundamental to quantifying injury and illness risk in sport.42 59 There are many ways to quantify athletic exposure and no single measure will suit all surveillance settings and research questions. The choice of exposure measures is heavily influenced by sport-specific and contextual factors, as well as which types of health problems are of interest. Therefore, it is often necessary to record exposure in several ways.
Tracking exposure for injury analyses
For injuries, exposure is generally quantified as the time during which athletes are at risk of injury (eg, minutes played), distance covered or a count of the number of specified events (eg, tackles, throws or jumps). In some sports, exposure is commonly expressed as the number of athletic participations (eg, games, races, training sessions), often referred to as ‘athletic exposures’. Table 2 in online supplementary appendix 1 provides a range of examples of exposure measures used.
Supplemental material
In team sports, we recommend recording exposure for each individual within a team rather than merely estimating the number of matches the team plays and match duration (team exposure), because the former permits the researcher to examine individual risk factors. Results of all the individuals are then summed to provide exposure at the sport or team level.
As injury risk is often markedly different between training and competition, these exposures should be recorded and reported separately. To do this consistently, it is necessary to define competition and training, and to consider situations where applying the definition may be challenging.
We define competition as organised scheduled play between opposing athletes or teams of athletes, or athlete(s) competing (i) against time and/or (ii) to obtain a score (judged or measured).
We define training as physical activities performed by the athlete that are aimed at maintaining or improving their skills, physical condition and/or performance in their sport.
In many sports, it is common to simulate competition as a part of training. Examples include preseason ‘friendly scrimmages’ between two teams or dividing a single squad into teams that compete against each other. In general, this should be counted as training exposure. Additionally, activities such as warm up and cool down should be counted separately and reported as training injuries, even if occurring around competition.
It is likely that in some sports, these definitions will not be fully applicable. In such cases, we encourage sport-specific consensus groups to define what constitutes competition and training in that sport.
Tracking exposure for illness analyses
Because athletes remain at risk of developing illness even when they are not participating in sport, it is inappropriate to use exposure measures such as playing hours or movement counts to quantify illness risks (except for the rare cases of transmissible infections that are specific to participation in a sport, eg, scrum-pox). Instead, it is often most appropriate to use exposure measures based on the time athletes are under surveillance (eg, days or years), rather than time engaged in competition and training.
Recording exposure during multiday competitions
Multiday competitions, such as championships and tournaments, represent an exposure measurement challenge, particularly for injury analyses. Ideally, investigators should obtain accurate records of every athlete’s individual participation (eg, training and competition minutes) throughout the tournament. However, this is not always feasible. Acceptable exposure estimates can also be made by obtaining summary data from every team for each day of the tournament (eg, squad numbers). As a minimum standard, exposure can be estimated for each event by multiplying the number of registered athletes by the duration of the tournament (the number of days of competition). In multisport tournaments, this should be calculated for each sport. However, this approach assumes that all athletes have the same exposure and participate every day, which is rarely the case.
Training subcategories
Different types of training should, if possible, be recorded and reported separately. Training types can be generally categorised as follows:
Sport-specific training: sessions involving the techniques and/or tactics of the sport, usually supervised by of a coach.
Strength and conditioning: sessions solely composed of resistance training and/or conditioning training. In many cases, training sessions are mixed (sports-specific, but with addition of some strength and conditioning, eg, plyometrics, endurance). As a pragmatic consideration, any session containing sports-specific training should be categorised as such, even if the session includes some strength and conditioning, purely to streamline exposure tracking.
Other training sessions: sessions that include activities other than sport-specific training or strength and conditioning. These include recovery sessions (eg, low-intensity running and stretching), rehabilitation and postrehabilitation transition sessions (ie, postreturn to sport but prior to resuming normal training).
Sport-specific injury surveillance systems may need to depart from this guidance if there is a need to address a specific training concern, however, at a minimum, all training exposure that contain sports-specific training should be tracked.
Sport-specific injury surveillance systems are encouraged to develop specialised procedures for tracking the diversity of training exposures in their particular sport. Training programmes vary considerably among sports and many coaches intentionally design training programmes that integrate multidimensional training (eg, plyometric stretching, sports-specific training, light running) into a single session. In general, investigators should prioritise capturing specific data on the training activities considered to present the greatest health risk.
Wearable physical activity tracking devices enable investigators to capture large volumes of competition and training data at the elite level and from community sports participants across large sample groups. We encourage the use of these devices for tracking exposure. However, we caution that any device needs to be fit for purpose, and researchers should obtain evidence on their validity and reliability before data collected through these devices are used for injury surveillance.
Expressing risk
Rates and proportions
Rates and proportions of injury and illness in studies of sports are usually reported as a count of ‘cases’ of the outcome of interest (the ‘numerator’), divided by a population at risk of developing the outcome (the ‘denominator’).60 Because research questions such as ‘How many players have suffered a knee injury?’, ‘What is the risk of getting injured in this sport?’ and ‘How does sport A compare with sport B for concussion risk?’ are very different, there are various ways of reporting risks relating to sports injury and illness. We explain some fundamental terms here.
Prevalence—How many? Prevalence is a proportion and refers to the number of existing cases divided by the total population at risk at a given point in time (point prevalence, eg, the proportion (percentage) of players in a volleyball team who—today—are suffering from patellar tendinopathy). It is a snapshot at one point in time, but can be repeated to determine changes in prevalence over time (eg, weekly). With serial measurements, it is possible to report, for example, the average prevalence over the course of the season and also to compare different stages of the season.
Period prevalence extends the concept of a single point in time to a window of time (eg, one season, a year). It refers to the proportion of athletes that has reported the condition of interest (eg, patellar tendinopathy) at any time during that given window. Notably, this includes people who already had the condition at the start of the study period as well as those who acquired it during that period.
Incidence—How often (do new cases occur)? Incidence is a rate and, as with any rate, time comes into play. Incidence refers to the number of new injuries/illnesses in the population that develop during a defined period of time. The term ‘incidence rate’ is synonymous, but we argue that it is a tautology—‘incidence’ is a rate.
Note that prevalence is calculated based on the number of athletes with a health problem, while incidence refers to the number of new health problems.
Recommendations: expressing risk in SIIS
Incidence-based measures usually represent more appropriate outcomes for sudden-onset conditions (eg, ankle sprains, ACL injuries) and prevalence-based measures for gradual-onset conditions (eg, asthma, patellar tendinopathy).46 Overuse injuries and pain problems such as low back pain and patellar tendinopathy are often chronic, with periods of remission and exacerbation. For example, in a professional volleyball team, there could be only one new case of patellar tendinopathy (so incidence will be low), yet 40% of the players (ie, nearly all pre-existing) could be affected by patellar tendinopathy during the season (period prevalence). Therefore, for such conditions, prevalence (the proportion of athletes affected) is a more appropriate measure than incidence (the number of new cases during the season).
Because sports and the activities that comprise them are so diverse, there is no single approach to expressing risk appropriately for all sports injury surveillance projects.61 In general, incidence-based measures that provide a standard time-window for the population at risk (injuries per hour) are preferable to measures for which the time at risk varies across individuals (injuries per athletic exposure, ie, per training session or match), because time-based measures better facilitate comparison across sports.
To provide numbers that are easy to interpret, avoiding small decimals, these data are typically reported as ‘per 1000 player hours’ (eg, concussion rate in men’s rugby study was reported as 4.7 per 1000 player hours, rather than 0.0047 per player hour).62 Such numbers allow risks to be compared (eg, How does concussion risk vary across contact sport codes?). We expect that subsequent sport-specific statements will recommend suitable, standard incidence-based measures for each sport. Table 2 in online supplementary appendix 1 provides a range of examples of risk measures.
If one injury event results in multiple injuries, these should only be counted as one when calculating overall injury incidence (eg, if a downhill skier crashes and suffers two injuries, a concussion and a tibia fracture, these are counted as one injury when calculating incidence).
Because of the difficulties in accurately measuring exposure to pathogens (which may be greater when not training or competing), illness risk should be estimated based on the entire period of exposure (eg, the duration of a competition, a ‘season of play’, a year), not athletic exposure only. We recommend reporting illness risk as either the incidence, the number of new illness cases divided by a period of time (eg, illnesses per 365 athlete-days),63 or as the period prevalence of illness, the proportion of athletes that were ill during a defined period.64 65
Where time-based measurements of exposure are unavailable, but participant numbers are available, crude rates of injury per number of participants per period can be derived. In such cases, we suggest that the incidence that may be most useful to permit population-level comparisons among sports or studies is ‘injuries per 365 athlete-days’.
Similarly, the proportion of participants with new or recurring injury or illness (ie, excluding pre-existing cases and exacerbations) during the event has been used to provide an impression of the risk associated with participation in each sport in both the summer and winter Olympic Games.64 65 However, this approach—period prevalence—can suggest widely different relative risks of activities that differ substantially in the amount of exposure participants experience.64 For example, exposure differs substantially between a football player and a sprinter. Period prevalence describes the absolute risk of participation in the Olympic Games, but not the relative risk (the risk of injury during 1 hour of football play vs 1 hour of marathon running).
Injury rates reported on a per-event (eg, per rugby tackle) basis provide information about how likely a particular aspect of play (‘event’) is to result in injury. Understanding events that both do66 and do not result in injury67 68 helps researchers identify injury prevention opportunities. In the absence of information about how frequently the event occurs within a sport and the average duration of the sport in which participants are exposed, rates per event also provide an incomplete view of the overall risks a sport poses. Using time-based and event-based denominators (eg, tackles in football codes) in parallel can help provide insights into both, which event (eg, tackle type) is most frequently associated with injuries and which event carries the highest risk when it occurs. To date, there have been relatively few injury surveillance studies in which such statistics have been provided together.29 For televised sports and those using new technology such as activity trackers, measurement of the duration of playing time and intensity for each individual is feasible, and coding of the number, characteristics and duration of activities each participant engages in (eg, tackles) is routine for some professional sports (eg, football). We include a real-life illustrative case of surveillance methods being used to investigate injury risk in rugby in online supplementary appendix 1.
Communicating risk to stakeholders
From clinical and practical perspectives, it is important that the end-users (the athletes, coaches and medical staff members) can make sense of the injury reports and increase the chances of having them participate in risk management plans. This can be done by expressing the injury incidence based on the concerned sport’s specifications. For instance, if an injury incidence for a specific muscle group (eg, hamstrings) is expressed as 0.9 injuries per 1000 hours of exposure, the incidence per player per season (0.28 injuries per player per season) could be multiplied by the average number of athletes per squad for the concerned sport (eg, 25 in football). This gives seven hamstring injuries per squad per season, a quantity which is more easily interpreted by end-users.
Another relevant measure, which is easy to communicate to managers, coaching staff and athletes, and which is associated with team performance in football,69 is player availability. Player match availability is calculated as the sum of player match opportunities (ie, the number of matches multiplied by the full size of the squad) minus the sum of player match absences due to injury or illness, and can be expressed as the average percentage over the period of interest (eg, one season). Training availability can be calculated in the same way.
We encourage sport-specific consensus statements to recommend relevant measures to communicate risk to relevant stakeholders.
Burden of health problems
Burden is a collective measure of the overall impact of a health problem in a specified population. In public health, burden is often expressed by financial cost, mortality or morbidity. One common approach is specific measures such as quality-adjusted life years or disability-adjusted life years.70 Burden allows different health problems to be compared—Does low back pain or diabetes cause more burden to society?
The burden of injuries and illnesses can also be expressed using measures that combine their frequency and consequences.71 72 For example, in football and rugby union, injury burden has been reported as the number of days of time loss per 1000 hours of player exposure.73–79 This contrasts with incidence (discussed earlier) where the numerator is the number of injuries, rather than the consequence of those injuries—days of time loss.
As measures of incidence and consequences vary depending on the purpose and setting of data collection, there is no single method of calculating burden in sport. To facilitate comparison among sports, investigators should consider reporting the number of days of time loss per 365 athlete-days for each outcome of interest, in addition to measures based on sport-specific exposures. We expect that subsequent sport-specific statements will provide recommendations on suitable, standard burden measures for each sport.
Burden can also be visualised using a risk matrix, in which the incidence of each health problem of interest is plotted against its consequences (such as mean time loss, as illustrated in figure 5). This is an effective way to communicate the overall burden (and its determinants) for a range of health problems. However, there are certain limitations to interpreting risk matrices, depending on how figures are designed and how data are structured (see Fuller for a detailed review).80
Burden measures that use time loss as a measure of severity fail to incorporate the most severe health problems (ie, fatalities and non-fatal catastrophic injuries and illnesses) and other cases where the athlete fails to return to sport (eg, due to retirement). As previously discussed, time-loss-based severity measures also under-represent overuse injuries and chronic illnesses.46 47 In this case, mean OSTRC-H severity scores can be used instead of time loss, as illustrated in figure 6.13

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk matrix based on Oslo Sports Trauma Research Center Questionnaire on Health Problems severity scores illustrating the burden of injuries and illnesses affecting elite Norwegian endurance athletes (unpublished data). Error bars represent 95% CIs.
Study population characteristics
Depending on the purpose of the study, demographic and health data may be included in injury and illness surveillance protocols. The demographic information captured should, as a minimum, include age, sex and level of competition and disability/impairment type in Paralympic sport. These can be supplemented with data on other relevant characteristics that could help investigators evaluate risk factors.
It is important to describe the performance and training level of the study population, both because they are often closely related to health outcomes and to allow appropriate studies to be compared.42 It is beyond the scope of this consensus group to provide a universal classification of competitive level. For example, the criteria used to define ‘elite’ vary considerably among sports. We encourage sport-specific methodological consensus groups to define what constitutes ‘elite’, ‘sub-elite’ and ‘recreational’ athletes in their sport.
Classification of sport categories
There are many ways of classifying and grouping sports. Any sports classification system used in surveillance should be clearly described in the methods section of reports. The description should permit other researchers to understand and replicate the process by which sports were grouped. The research problem being addressed should shape the classification system used, rather than vice versa.
Data collection methods
The methods underpinning the data collection have great impact on the outcome of sport injury and illness surveillance studies.42 81 82 A systematic review of ongoing injury surveillance systems in sport found that data quality aspects were published for only 7 of the 15 systems and validation studies for only 4.83 The review concluded that data quality could be improved through the establishment of data collection standards.
Given the wide range of settings in which surveillance is undertaken, the data collection methods should be flexible enough to adapt to the specific context (eg, sport culture, level of sport, availability of resources) and to the specific research question and objectives of the study.42 These factors in combination will determine:
who should provide the information (eg, athlete, physician, physiotherapist, coach, non-clinical volunteer);
what data sources should be used (eg, athlete self-report, medical records, examinations, video recording);
the frequency of data collection and reporting (eg, daily, weekly, monthly);
the timing of and window for data collection (eg, day of injury/illness or of competition/training or following day, within a week);
the duration of surveillance (eg, tournament, season, whole year, playing career).
Taking all of these variables into account, it is evident that ‘one size does not fit all’.84 85
In 2001, WHO81 86 published guidelines for injury surveillance that remain relevant. In particular, some general aspects about quality of the data collection systems (ie, objectivity, reliability, validity, practicability, risk of bias, cost-effectiveness/time-effectiveness, acceptability), quality of implementation (eg, guidance document, communication, compliance and data check) and some methodological issues (eg, handling of missing values, completeness of reports, coverage, response rate) are important.9 87 88 In addition, the choice of injury definition, exposure measure and methods used to express rate influence the results substantially, as discussed in the relevant sections of this document.
The reliability of the system can be improved by tailored education, ongoing support for the people who report the data and a detailed process manual,86 and should be evaluated at least by analysis of inter-rater reliability of people reporting the data.88
Validity and completeness of data reporting can be analysed comparing with another ‘“gold standard’ data source.38 89–93 A recent study showed that research-involved staff recording the data in a surveillance programme reported a greater number of mild injuries than did non-researchers.94
An example of specific measures to improve reliability of a surveillance project is illustrated in box 1, based on the procedure of the Professional Rugby Injury Surveillance Project.95
Implementation recommendations for injury/illness surveillance; the implementation of an injury and illness surveillance project should include the following aspects:
Methods based on this consensus statement on definitions and data collection procedures.
Mandatory standards for compliance with defined timescales for completion for report forms.
Guidance document (a quality protocol) shared with all clubs/national team’s medical staff (preseason/tournament).
Regular contact between study lead and responsible person at each club/national team (face-to-face meeting preseason/prior the tournament, conference call mid-season/tournament).
All injuries cross-checked with club/teams medical records and followed up with medical staff for missing, incomplete, inconsistent or duplicate entries (regularly during season/tournament).
Data cleaning and final review of the dataset with responsible person at each club/team prior to definitive analysis (end of season/tournament).
Injury reports where individual club/team data are are reported, analysed and compared with the average of all participating clubs/teams (mid-season and end-of-season/tournament).
Medical meeting (end of season/tournament), where whole surveillance results and translational value are presented to club/team medical practitioners for discussion.
From pen and paper to electronic solutions
Health problems and exposure can be captured using different methods ranging from paper copy data collection forms to a comprehensive web-based surveillance system, for example, internet platforms, apps or text messaging.51 90 91 96–100 The traditional pen and paper approach is often easy to implement,50 as it reduces the need for specific technical knowledge, equipment and related costs.51 101 Data can be verified and cleaned as they are manually entered.101
Electronic data capture reduces time for duplication of data entry,50 and associated entry errors.101 In terms of costs, there is potential long-term cost-effectiveness through the elimination of expenses linked to the printing, shipping, management and storage of physical documents.101
Web-based solutions allow instant and remote on-demand queries of real-time data (including end-users such as team medical staff), as well as integration with other data feeds (eg, performance, load, sleep). Web-based solutions should preferably be prototyped prior to being implemented in a larger injury surveillance setting. Full integration of surveillance reporting systems within clinical electronic medical record keeping systems has been used successfully in a number of professional elite leagues.102 While electronic solutions can lead to high response rates among athletes,90 91 98 there are also reports of poor athlete engagement,97 and thus demonstrates the importance of understanding uptake barriers. It is important to use surveillance tools that minimise intrusion into the daily activities of the data reporters (athletes, medical teams, coaches), for example, by limiting the number of questions to responders so that only essential data are captured. Another recommendation is to provide a clear incentive to athletes and teams to participate in injury surveillance, for example, by allowing continuous feedback within the data collection system (eg, performance data, load monitoring data) or sending regular reports back to the teams, athletes and other relevant stakeholders.103
Data collection methods must be adapted to the specific research question, the sport context and the skill set of the research team, and should follow strict quality standards. The quality of the surveillance system includes the quality of the forms (baseline, health problems and exposure) as well as the quality of the data collection procedure, implementation, data cleansing and analysis methods.51 The quality and usability of the forms and the data collection procedures should be examined before implementation. Reliability and validity should be analysed, and all translations should follow the standards of intercultural adaptation.104 105 The adherence to the data collection protocol as well as the completeness and consistency of responses should be monitored on a regular basis during implementation. Collaboration between research groups to share resources and joint data analytics can help advance the management of sport injuries/illnesses.106 Having data collection forms and related material available in free-to-access formats make it easier for sports bodies to participate in surveillance activities,51 and this consensus statement includes some sample forms as mentioned in online supplementary appendix 2.
Supplemental material
Research ethics and data security
Research ethics govern the conduct of medical research and aim to protect the dignity, rights and welfare of human participants. They detail principles such as informed consent, data confidentiality, the use of research ethics committees and risks, burdens and benefits. Importantly, informed consent is the process in which permission is granted in full knowledge of the possible consequences (risks and benefits), for example, for their data to be used for research purposes. In some contexts, injury and illness surveillance may be regarded as an integral part of data audit and quality control processes, and—as long as individual patient data are fully deidentified—may not require informed consent. It is the duty of all researchers (and all other users of the data) to consider—and adhere to where appropriate—internationally recognised guidelines for research ethics (such as the Declaration of Helsinki107 and the Declaration of Taipei).108
Data protection governs how data are collected, shared, used and conserved, and aims to ensure that personal data are safe from unforeseen, unintended or malevolent use. Particular attention must be directed to the security of data stored on cloud-based systems and other electronic repositories. Researchers must adhere to the data protection regulations applicable to their context (such as General Data Protection Regulation in Europe).109
Reporting guidelines: STROBE Sports Injury and Illness Surveillance
The statement on STROBE was published in 2007.110 Since then, it has been adapted (‘extensions’) to ensure the statement is relevant to other areas of interest such as infectious diseases,111 and most recently (2018) for pharmacoepidemiology.112 These extensions of STROBE have stressed, like the original, that they only guide on how to report findings from observational studies rather than guiding study design. However, the two are related and researchers are strongly encouraged to consider the elements of the checklists when planning studies—this may eventually improve study quality and ensure researchers are able to report what is needed at the end of the study. STROBE has checklists for the three most common study types: cohort studies, case-control studies and cross-sectional studies. Here, we summarise our consensus recommendations on the collection and reporting of SIIS data as an extension to the initial STROBE checklist. These apply regardless of study design. Note that many other study designs common in sports and exercise medicine research—such as randomised controlled trials—should be reported against other reporting standards (like ConsolidatedStandards of Reporting Trials, which will be refreshed in 2020).113 As most sports medicine studies rely on surveillance methods to collect injury and illness outcome data, the recommendations in this consensus statement apply widely.
To guide researchers in the field of sport and exercise medicine, we have adapted (‘extended’) the STROBE checklist so that it reflects recommendations from this current IOC consensus statement on studies of injury and illness surveillance in sport. This extension refers to 21 of the original items. It includes only items specific to the reporting of injuries and illnesses in sport, as amendments to reflect broader epidemiology methodology developments should be more appropriately documented by the EQUATOR network which oversees STROBE.
It is intended that this new checklist—STROBE-SIIS—will help researchers design an injury/illness surveillance study and plan the study protocol, as well as better report their observations (online supplementary appendix 3). By consistently using STROBE-SIIS, the authors ensure that other researchers will be able to more easily replicate, compare and synthesise sport and exercise medicine research studies.
Supplemental material
We also strongly recommend that researchers publish their study protocols ahead of study completion, ideally with an open-access formal register, and also report on any changes made to the initial protocol during study conduct, together with their rationale for the change, once the study has been completed. Details of where protocols and their amendments are publicly available should be stated in papers submitted for publication.
Feedback on this checklist is welcome and we will both monitor and evaluate the impact of its use overtime. We welcome researchers with relevant expertise to translate this checklist to other languages for the benefit of the international sports medicine community.
Acknowledgments
The authors would like to thank Ali Abdalla Hassan and Mohamed Abdo Badwi Ismael at Aspetar Orthopedic and Sports Medicine Hospital for their assistance with the online survey. The authors would also like to thank Paul Blazey and David Moher in developing and revising the STROBE-SIIS checklist.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RoaldBahr, @benclarsen, @dvorak_11, @CarolynAEmery, @CarolineFinch, @MHgglund, @drsimonkemp, @margo.mountjoy, @DrJohnOrchard, @docpluim, @kenquarrie, @TSoligard, @drkeithstokes, @Evertverhagen, @larsengebretsen
Presented at This article has been co-published in the British Journal of Sports Medicine and Orthopaedic Journal of Sports Medicine.
Correction notice This article has been corrected since it published Online First. The competing interests statement has been added and figure 1 replaced.
Contributors Please see 'Methods' section.
Funding The International Olympic Committee has provided funding for the consensus meeting.
Competing interests BR receives payment for duties as Editor-in-Chief of the The Orthopaedic Journal of Sports Medicine. KK is the Editor-in-Chief of the British Journal of Sports Medicine.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement No data are available.