Article Text

Abstract
Objective To investigate the relationships between exercise and incidence of congenital anomalies and hyperthermia.
Design Systematic review with random-effects meta-analysis .
Data sources Online databases were searched from inception up to 6 January 2017.
Study eligibility criteria Studies of all designs were eligible (except case studies and reviews) if they were published in English, Spanish or French, and contained information on population (pregnant women without contraindication to exercise), intervention (subjective or objective measures of frequency, intensity, duration, volume or type of exercise, alone [“exercise-only”] or in combination with other intervention components [e.g., dietary; “exercise + co-intervention”]), comparator (no exercise or different frequency, intensity, duration, volume or type of exercise) and outcome (maternal temperature and fetal anomalies).
Results This systematic review and meta-analysis included ‘very low’ quality evidence from 14 studies (n=78 735) reporting on prenatal exercise and the odds of congenital anomalies, and ‘very low’ to ‘low’ quality evidence from 15 studies (n=447) reporting on maternal temperature response to prenatal exercise. Prenatal exercise did not increase the odds of congenital anomalies (OR 1.23, 95% CI 0.77 to 1.95, I2=0%). A small but significant increase in maternal temperature was observed from pre-exercise to both during and immediately after exercise (during: 0.26°C, 95% CI 0.12 to 0.40, I2=70%; following: 0.24°C, 95% CI 0.17 to 0.31, I2=47%).
Summary/Conclusions These data suggest that moderate-to-vigorous prenatal exercise does not induce hyperthermia or increase the odds of congenital anomalies. However, exercise responses were investigated in most studies after 12 weeks’ gestation when the risk of de novo congenital anomalies is negligible.
- exercise
- women
Statistics from Altmetric.com
Introduction
WHO defines congenital anomalies as structural or functional birth defects with origins during intrauterine life.1 Two to three per cent of all infants are affected by congenital anomalies, and an estimated 300 000 newborns worldwide die every year in the first month of life as a result.1 The causes of congenital anomalies are multifactorial. A better understanding of the factors contributing to the development of these defects is critical for prevention.
Maternal hyperthermia is a well-established teratogen in animal models, and there is epidemiological evidence that suggests adverse effects on human embryos.2 Hyperthermia in pregnancy from exposure to external heat sources during the preimplantation stage is associated with spontaneous abortion or congenital anomalies (eg, neural tube defects). Hyperthermia occurring after implantation can induce anomalies that are dependent on the intensity and duration of intrauterine exposure to hyperthermia, as well as the stage of embryonic development at which hyperthermia occurs.3 While it is recognised that teratogen exposure in the first 15 weeks of pregnancy is associated with an increased rate of abnormalities, exposure in the second and third trimesters is also associated with adverse outcomes.4 For example, human fetal neurological development occurs during the second trimester of pregnancy,5 and there is evidence from animal models on an association between hyperthermia and restricted brain growth and brainstem and cerebellum development.6 Maternal hyperthermia late in pregnancy has also been deemed a potential risk factor for cerebral palsy.5 Therefore, it is critical that hyperthermia is investigated throughout all stages of pregnancy.
The present systematic review and meta-analysis was conducted as part of a series of reviews that will form the evidence base for the development of the 2019 Canadian guideline for physical activity throughout pregnancy (herein referred to as the Guideline).7 The primary objectives of the present systematic review and meta-analysis were (1) to identify the impact of prenatal exercise throughout pregnancy on the odds of congenital anomalies, and (2) to explore the relationship between prenatal exercise and maternal body temperature.
Methods
In October 2015, the Guidelines Consensus Panel assembled to identify priority outcomes for the Guideline. The Panel included researchers, methodological experts, a fitness professional and representatives from the Canadian Society for Exercise Physiology (CSEP), the Society of Obstetricians and Gynaecologists of Canada, the College of Family Physicians of Canada, the Canadian Association of Midwives, the Canadian Academy of Sport and Exercise Medicine, Exercise is Medicine Canada, and a health unit (the Middlesex-London Health Unit). The Guidelines Consensus Panel identified 20 ‘critical’ and 17 ‘important’ outcomes related to prenatal exercise and maternal/fetal health. One of the ‘critical’ outcomes (ie, congenital anomalies) and one of the ‘important’ outcomes (ie, maternal temperature) are examined in this review. This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the checklist was completed.8
Protocol and registration
Two systematic reviews examining the impact of prenatal exercise on fetal and maternal health outcomes were registered a priori with PROSPERO, the International Prospective Register of Systematic Reviews (fetal health: trial registration number CRD42016029869; maternal health: trial registration number CRD42016032376). Because the relationships between prenatal exercise and maternal body temperature are examined in studies related to both fetal and maternal health, records retrieved from both of these reviews were evaluated for inclusion in the current study.
Eligibility criteria
This study was guided by the participants, interventions, comparisons, outcomes and study design (PICOS) framework.9
Population
The population of interest was pregnant women without contraindication to exercise (according to the CSEP and the American Congress of Obstetricians and Gynecologists guidelines).10 11 Absolute contraindications to exercise were defined as ruptured membranes, premature labour, persistent second or third trimester bleeding, placenta previa, pre-eclampsia, gestational hypertension, incompetent cervix, intrauterine growth restriction, high-order pregnancy, uncontrolled type 1 diabetes, hypertension or thyroid disease, or other serious cardiovascular, respiratory or systemic disorders. Relative contraindications to exercise were defined as a history of spontaneous abortion, premature labour, mild/moderate cardiovascular or respiratory disease, anaemia or iron deficiency, malnutrition or eating disorder, twin pregnancy after 28 weeks, or other significant medical conditions.10 11
Intervention (exposure)
The intervention/exposure of interest was objective or subjective measures of exercise or intervention (ie, frequency, intensity, duration, volume or type). Exercise during pregnancy could be acute (ie, a single exercise session) or habitual (ie, regular activity). Interventions including exercise alone (termed ‘exercise-only’ interventions) or in combination with other interventions (such as diet; termed ‘exercise+co-interventions’) were considered. Exercise-only studies could include standard care. Studies that included exercise that began after the initiation of labour were not eligible. For this review, the terms ‘exercise’ and ‘physical activity’ were used interchangeably to define any bodily movement generated by skeletal muscles that resulted in energy expenditure above the resting levels.12
Comparison
Eligible comparators were no exercise; different frequency, intensity, duration, volume or type of exercise; different intervention duration; or exercise in a different trimester.
Outcomes
Outcomes of interest were congenital anomalies and maternal temperature. Hyperthermia was defined as increases in maternal temperature of ≥2°C from pre-exercise to during or postexercise, or to an absolute core temperature >38°C.13 14 If maternal temperature was reported at multiple time points, all maternal temperatures during exercise were extracted. Maternal temperature was included if assessed using standard measures.
Study design
Studies of any design were eligible for inclusion, except for case studies (n=1) and reviews. The initial search was not limited by the language of publication.
Information sources
A comprehensive search was created and run by a research librarian (LGS) in the following databases: MEDLINE, EMBASE, PsycINFO, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Scopus and Web of Science Core Collection, CINAHL Plus with Full-text, Child Development & Adolescent Studies, Education Resources Information Center, SportDiscus, ClinicalTrials.gov, and the Trip Database, up to 6 January 2017 (see online supplementary data for complete search strategies). The searches combined keyword terms and controlled vocabulary terms (when available) for each of the following concepts: (1) exercise/physical activity, (2) pregnancy, and (3) outcomes of fetal congenital anomalies and maternal temperature (see online supplementary data for complete search strategies).
Supplemental material
Study selection and data extraction
Two reviewers independently screened the titles and abstracts of all articles identified by the search. Abstracts that met the initial screening criteria at level 1 as determined by at least one reviewer were retrieved as full-text articles for level 2 screening. Two reviewers independently screened full-text articles against study inclusion criteria. For studies where at least one reviewer recommended exclusion, further review was conducted by MHD and/or S-MR for a final decision on exclusion. If agreement could not be reached by discussion, study characteristics related to eligibility were presented to the Guidelines Steering Committee (MHD, MFM, S-MR, CEG, VJP, AJG and NB) and final decisions were made by consensus. Studies that were selected were imported into DistillerSR (Evidence Partners, Ottawa, Ontario, Canada) for data extraction. At this point, studies from the maternal and fetal reviews that were included were de-duplicated against one another in DistillerSR and were considered as one review from this point forward.
Creation of data extraction tables in DistillerSR was done in consultation with methodological experts and the Guidelines Steering Committee. Data from records that met the inclusion criteria were extracted by one person and independently verified by a content expert (MHD, MFM or S-MR). For each unique study, the most recent or complete version (publication) was selected as the ‘parent’ paper; however, relevant data from all publications related to each unique study were extracted. Extracted data included study characteristics (ie, year, study design, country), characteristics of the population (eg, number of participants, age, prepregnancy body mass index (BMI), parity, and pregnancy complications including pre-eclampsia, gestational hypertension and gestational diabetes), intervention/exposure (prescribed and/or actual exercise frequency, intensity, duration and type of exercise, duration of the exercise training, measure of exercise) and outcomes (congenital anomalies and maternal temperature). If data were unavailable for extraction, the authors were contacted to request additional information. If data were only available in figures, and the corresponding authors did not provide numerical data on request, GetData Graph Digitizer (V.2.26) was used to digitise graphs to extract data. Data from figures were extracted independently by two extractors, and the average of the values was used in the final analysis. If the data obtained from the extractors differed by more than 5%, a third reviewer extracted data and the two closest points were averaged. In this case, the data were also reviewed by MHD to ensure accuracy.
Quality of evidence assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework was used to assess the quality of evidence across studies for each study design and health outcome.15
Evidence from randomised controlled trials (RCTs) began with a ‘high’ quality of evidence rating and was graded down if there was concern with risk of bias, indirectness, inconsistency, imprecision and risk of publication bias, because these factors reduce the level of confidence in the observed effects. Evidence from non-randomised interventions and observational studies began with a ‘low’ quality of evidence rating and, if there was no cause to downgrade, was upgraded if applicable according to the GRADE criteria (eg, large magnitude of effect, evidence of dose–response). Studies reporting on the effect of acute exercise on maternal temperature were considered cross-sectional studies and therefore began with a ‘low’ quality assessment.
The Cochrane Handbook was used to assess the risk of bias in RCTs and intervention studies,16 and the risk of bias in observational studies was assessed using the characteristics recommended by Guyatt et al,15 which has been used by other physical activity systematic reviews.17 All studies (RCTs, intervention studies and observational studies) were assessed for potential sources of bias, including selection bias (RCT/intervention: inadequate randomisation procedure; observational: inappropriate sampling), reporting bias (selective/incomplete outcome reporting), performance bias (RCT/intervention: compliance to the intervention; observational: flawed measurement of exposure), detection bias (flawed measurement of outcome), attrition bias (incomplete follow-up, high loss to follow-up) and ‘other’ sources of bias. Risk of bias across studies was rated as ‘serious’ when studies having the greatest influence on the pooled result (assessed using weight (%) given in forest plots or sample size in studies that were narratively synthesised) presented ‘high’ risk of bias. The greatest influence on the pooled result was determined as follows: the studies that had the greatest individual per cent contribution in the meta-analyses, when taken together, contribute to >50% of the weight of the pooled estimate. Serious risk of bias was considered when the sample size of studies that were narratively synthesised was similar to the total sample size of studies contributing to >50% of the weight of the pooled estimate in the meta-analyses. Given the nature of exercise interventions, it is not possible to blind participants to group allocation. Therefore, if the only source of bias was related to the blinding of allocation, selection risk of bias was rated as ‘low’. Performance bias was rated as ‘high’ when <60% of participants performed 100% of prescribed exercise sessions or attended 100% of counselling sessions (defined as low compliance) or when compliance to the intervention was not reported. Attrition bias was rated as ‘high’ when >10% of data were missing at the end of the study and intention-to-treat analysis was not used.
Inconsistency was considered serious when heterogeneity was high (I2≥50%) or when only one study was assessed (I2 unavailable). Indirectness was considered serious when interventions included both exercise and additional components (ie, exercise+cointerventions, or exercise-only and exercise+cointerventions pooled in the analysis). Imprecision was considered serious when the 95% CI crossed the line of no effect and was wide, such that interpretation of the data would be different if the true effect were at one end of the CI or the other. When only one study was assessed, imprecision was not considered serious as inconsistency was already considered serious for this reason. Finally, to assess the likelihood of publication bias for a given outcome, funnel plots were created if there were more than 10 studies included in a meta-analysis. Funnel plots were examined visually and if the scatter of the points did not reflect a funnel shape, publication bias was considered serious. If there were fewer than 10 studies, publication bias was deemed non-estimable and not rated down. Due to time constraints and feasibility, one reviewer evaluated the quality of the evidence across each health outcome using the protocol and a second person reviewed the GRADE tables as a quality control measure. The GRADE tables are presented in online supplementary tables 3 and 4.
Statistical analysis
Statistical analyses were conducted using Review Manager V.5.3. (Cochrane Collaboration, Copenhagen, Denmark). Statistical significance was set at p<0.05. For all dichotomous outcomes, ORs were calculated. Inverse-variance weighting was applied to obtain OR using a random-effects model. For continuous outcomes, the mean differences between exercise and control groups were examined and the weighted mean differences were calculated using random effects. The SD of change scores was calculated assuming a correlation of 0.5 and then converted into SE. For continuous outcomes that reported on prevalues and postvalues for acute exercise, change scores were calculated using the generic inverse variance method.16 18 First, the mean differences were calculated by subtracting the precondition (prior to exercise) value from the postcondition (during exercise/postexercise). Next, the SD of the change score was calculated assuming a correlation of 0.5 and converted into SE. As indicated above, for each outcome, all instances of acute exercise were combined onto a single forest plot and were not separated by study design. In studies where there were no observed events in the intervention or control group, data were entered into forest plots, but were considered ‘not estimable’ and excluded from the pooled analysis as per the recommendation in the Cochrane Handbook method.16 The I2 index was calculated to indicate the per cent of total variability attributable to between-study heterogeneity. Meta-analyses were performed separately by study design when the exposure was chronic exercise. For RCTs and non-randomised interventions, sensitivity analyses were performed to evaluate whether the effects were different when examining relationships between exercise-only interventions versus exercise+cointerventions and the outcome of interest. A staged approach was used to determine inclusion of study designs other than RCTs. For each outcome, RCT evidence was initially examined. If fewer than 2000 women were included in the exercise-only RCT meta-analysis, the impact of prenatal exercise on the specific outcome was examined further using observational evidence (non-randomised interventions, cohort, cross-sectional and case–control studies of any sample size). When possible, the following a priori determined subgroup analyses were conducted for exercise-only interventions and observational studies: (1) women diagnosed with diabetes (gestational, type 1 or type 2) compared with women without diabetes); (2) samples of women with overweight or obesity (mean BMI>25.0 kg/m2) prior to pregnancy compared with samples of women who were of various BMI (mean BMI<25 kg/m2 but possibly with some individuals with BMI>25.0 kg/m2); (3) women >35 years of age compared with women <35 years of age; and (4) women who were previously inactive compared with those who were previously active (as defined by individual study authors). If a study did not provide sufficient detail to allow it to be grouped into the a priori subgroups, then a third group called ‘unspecified’ was created. Tests for subgroup differences were conducted, with statistical significance set at p≤0.05. Subgroup differences were only interpreted when statistically significant differences were found.
For the ‘maternal temperature’ outcome, subsequent posthoc subgroup analyses were conducted: duration of exercise (≤20 min, 21–40 min and >41 min) and intensity of exercise (‘light’, ‘moderate’ and ‘vigorous’ intensity as indicated by objective or subjective measures19). Objective measures included cut-offs reported as the percentage of maximum maternal heart rate, maternal heart rate reserve and percentage of maximum oxygen consumption.19 In the case where two intensity measures were reported, creating a discrepancy of subgroup placement, objective measures were used. In instances where target intensity differed from the actual reported intensity of exercise, the actual intensity was used.
For outcomes where a meta-analysis was not possible, the results were presented as a narrative synthesis, structured around each outcome. Within each outcome, the results were organised by study design. Unless otherwise specified, studies were not included in meta-analyses if data were reported incompletely (SD, SE or number of cases/controls not provided), or if data were adjusted for confounding factors or if the study did not include a non-exercising control group. In studies where data were included in the meta-analysis but additional information was available, the studies were included in both the meta-analysis and narrative synthesis.
Results
Study selection
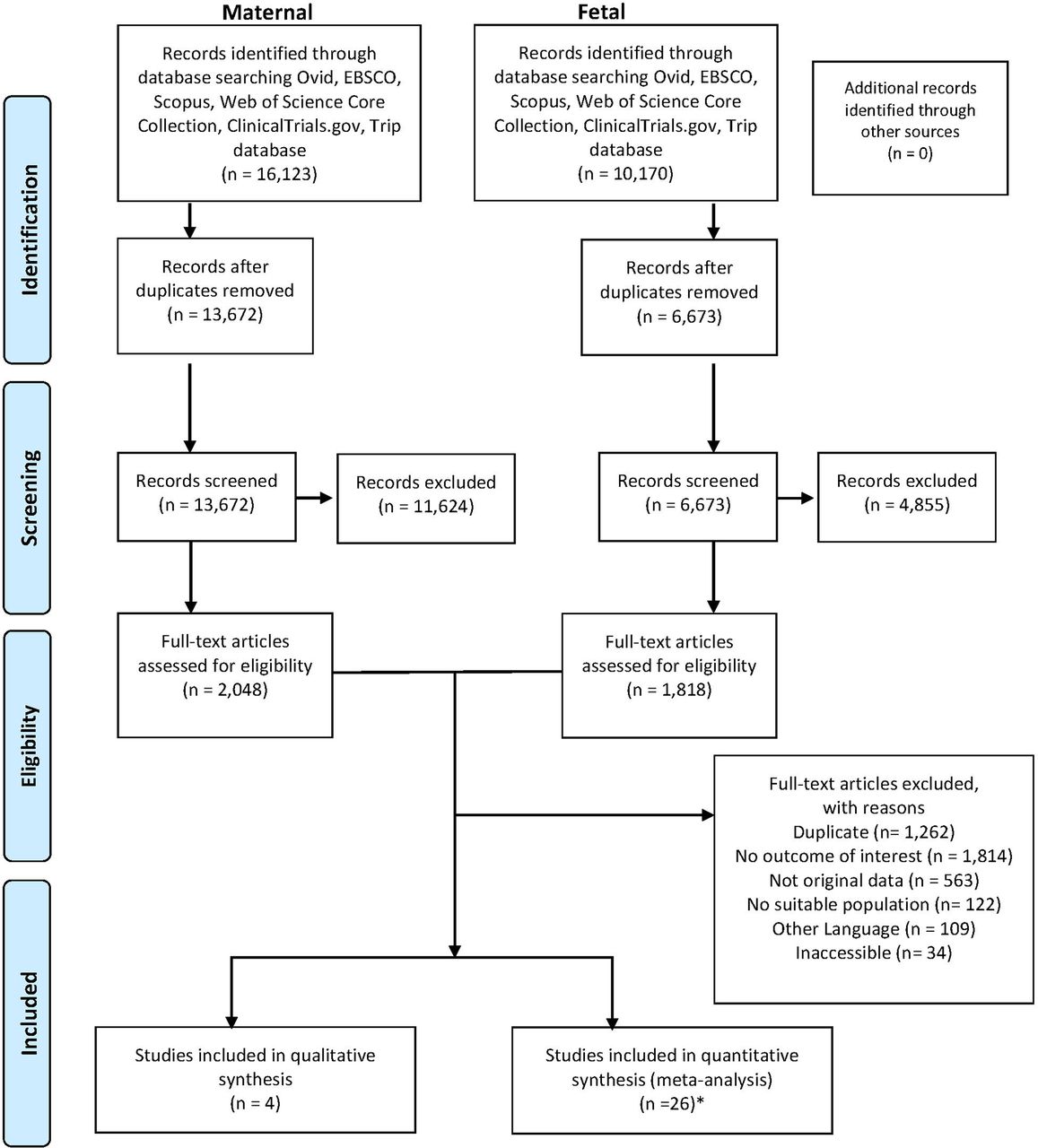
Although all languages were included in the initial search, for feasibility reasons studies that were published in languages other than English, Spanish or French were excluded. Twenty-nine unique studies including 79 395 women met our inclusion criteria. A PRISMA diagram depicting the flow of information through phases of the systematic review is shown in figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. *One study was included in both the qualitative and quantitative analyses.
Study characteristics
Congenital anomalies
Congenital anomalies were defined as per the authors’ definitions and were assessed via medical records or maternal self-report. Fourteen studies (ten RCTs, three non-randomised trials and one cohort study; n=78 735) from nine countries assessed the relationship between exercise and congenital anomalies. These studies represented all stages of gestation, with interventions beginning as early as conception and as late as the third trimester. The interventions included yoga or aerobic exercise performed 1–7 days per week, for 15–50 min per session at a low to moderate intensity of exercise. Additional details regarding the studies can be found in online supplementary table 1.
Maternal temperature
Fifteen studies (n=447 women) from five countries assessed prenatal exercise and maternal temperature across all trimesters. Maternal temperature was measured in rectal, skin, oral and tympanic locations. Additional details can be found in online supplementary table 1.
Synthesis of data
Congenital anomalies
There was ‘very low’ quality evidence from 10 RCTs (n=5141 women) indicating that prenatal exercise did not affect the odds of congenital anomalies (OR 1.23, 95% CI 0.77 to 1.95, I2=0%; figure 2).20–29 The quality of evidence was downgraded from ‘high’ to ‘very low’ because of serious risk of bias, indirectness of the interventions and imprecision.
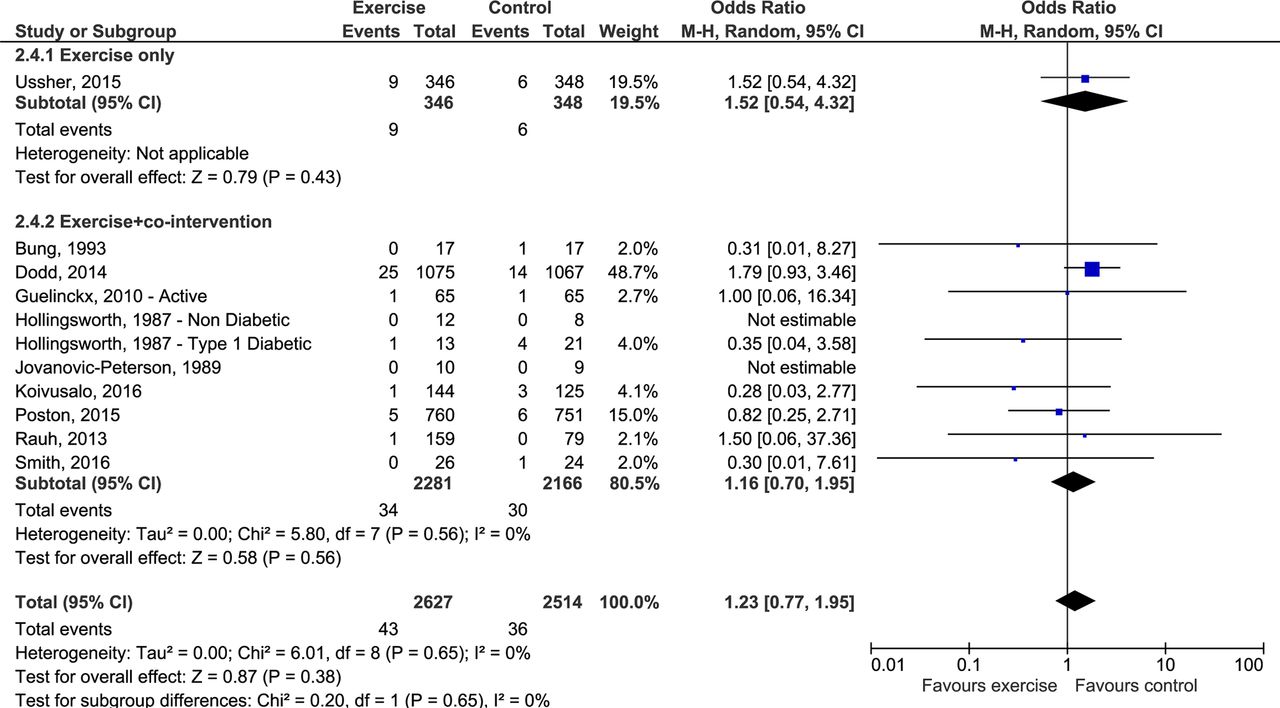
Effects of prenatal exercise-only versus exercise plus cointervention compared with control on congenital anomalies (randomised controlled trials). Analyses conducted with a random-effects model. M-H, Mantel-Haenszel method.
Sensitivity analysis
The pooled estimate for the exercise-only interventions was not significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.65).
Non-RCT studies
There was ‘very low’ quality evidence (rated down due to serious risk of bias, inconsistency and imprecision) from three non-randomised exercise+cointerventions (n=322 women)30–32 and one cohort study (n=73 272 women)33 that also showed no effect of prenatal exercise on the odds of congenital anomalies (see online supplementary figures 1 and 2).
Maternal temperature
GetData Graph Digitizer was used to extract numerical data in figures from four studies.33–36
Resting maternal temperature
Resting maternal temperature was reported in 10 studies (n=426).34 36–45 From conception to 16 weeks’ gestation, resting temperatures ranged from 37.1°C to 38.1°C.37 43 In pregnancy weeks 17–27, resting temperatures ranged from 36.2°C to 37.75°C.34 37–39 44 In the third trimester (>27 weeks), resting temperatures ranged from 36.2°C to 37.6°C.34–37 40–42 44
Rest to during exercise
There was ‘very low’ quality evidence from six studies (n=182 women; one RCT, three cohort and two cross-sectional studies) examining the effect of acute exercise on maternal temperature from rest to during exercise. The quality of evidence was downgraded from ‘low’ to ‘very low’ because of inconsistency. Maternal body temperature increased significantly from rest to during exercise in the second and third trimesters (pooled estimate based on five studies, n=170; 0.26°C, 95% CI 0.12 to 0.40 I2=70%; figure 3).34–37 45 One study (n=12) that could not be included in the meta-analysis because pre-exercise temperatures were not reported demonstrated that maternal temperatures during exercise did not exceed 38°C during the first, second and third trimesters (37.4°C±0.4, 37.2°C±0.3 and 37.3°C±0.2, respectively; online supplementary table 1).46 The posthoc tests for subgroup differences performed were not statistically significant (see figures 3 and 4).

Effect of acute exercise on changes in maternal temperature from pre-exercise to during exercise. Subgroup analyses were conducted with studies including exercise of the following durations: ≤20 min, 21–40 min or >40 min. EX, exercise; IV, inverse variance; wks, weeks.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of acute exercise on changes in maternal temperature from pre-exercise to during exercise. Subgroup analyses were conducted with studies including exercise of moderate and vigorous intensity. EX, exercise; IV, inverse variance; wks, weeks.
Rest to during recovery
There was ‘very low’ quality evidence from 15 studies (n=447 women; 1 RCT, 1 non-randomised intervention, 9 cohort studies and 4 cross-sectional studies) regarding changes in maternal body temperature from rest to the recovery period (following exercise) during the first, second and third trimesters. The pooled estimate was based on 10 studies (n=394 women) and demonstrated maternal body temperature increased following exercise compared with rest (within 10 min of recovery; 0.24°C, 95% CI 0.17 to 0.31, p<0.00001, I2=47%34 36 38 40–45 47; online supplementary figure 3). Five studies (n=53 women) could not be included in the meta-analysis due to incomplete reporting of results (ie, SD not reported, baseline values missing) or lack of a comparison group. One demonstrated that maternal temperatures during exercise and up to 10 min postexercise did not exceed 38°C during the first, second and third trimesters (37.4°C±0.4, 37.0°C±0.4 and 37.2°C±0.4, respectively; online supplementary table 1).46 In another study, there were no numerical values of temperature response reported, but the authors stated that there was no significant change in maternal temperature in response to acute vigorous exercise in the second and third trimesters (online supplementary table 1).48 Results from three other studies showed that compared with rest, maternal temperature after exercise of any intensity did not increase core body temperature by more than 0.5°C37 39 or 1°C49 (online supplementary table 1). At both points of measurement (first and third trimesters), maternal core temperature did not exceed our thresholds for hyperthermia.49 The tests for a posteriori subgroup differences performed were not statistically significant (see online supplementary figures 3 and 4).
Discussion
Congenital anomalies are considered adverse fetal outcomes and maternal hyperthermia is one of the established risks for these anomalies. The purpose of this review was to conduct a comprehensive analysis of the impact of prenatal exercise on (1) the odds of congenital anomalies and (2) maternal hyperthermia. There was ‘very low’ quality evidence from 14 studies (n=78 948 women) indicating that prenatal exercise initiated at any time during pregnancy was not associated with congenital anomalies. There was ‘very low’ to ‘low’ quality evidence from 15 studies (n=447 women) indicating an increase in maternal body temperature up to 1°C during and following exercise performed during the second and third trimesters. The increase in maternal temperature during or following an acute bout of exercise was not significantly different between different intensities or different durations of exercise. Importantly, increases in maternal temperature never reached hyperthermia (ie, did not increase by 2°C or more), suggesting that exercise-induced increase in maternal temperature is safe for the fetus.
Guidelines for prenatal exercise worldwide recommend that all women without contraindications to exercise be physically active to obtain the many known maternal and fetal health benefits.10 11 50 However, the impact of prenatal exercise on risk of hyperthermia or congenital anomalies was not addressed in previous guidelines for prenatal exercise. Maternal hyperthermia is a well-known teratogen that is associated with congenital anomalies.2–6 51 The findings of our review that prenatal exercise does not exceed hyperthermic thresholds are supported by a recent review.52 The risk of congenital anomalies via hyperthermia during exercise may be attenuated by pregnancy-induced physiological mechanisms that could improve the ability of pregnant women to adequately thermoregulate during and after a bout of exercise. When heat stress is induced by exercise, the produced heat is dissipated primarily via cutaneous vasodilation and sweating initiated by the autonomic nervous system.53 Pregnancy is associated with up to a 50% increase in blood volume, concurrent with decreased cardiovascular resistance, which results in an increase in stroke volume and cardiac output.53 The predominant challenge to the cardiovascular system in response to heat stress is to produce adequate cardiac output for sufficient blood flow. This challenge may be mitigated by the natural increase in cardiac output induced by pregnancy.54 Additionally, research has shown that vasodilation in the muscle and skin can be produced via the heat-induced release of nitric oxide within the skeletal muscle and skin for increased heat dissipation.55 This may be a mechanism that is improved in pregnant women, as increased vascular nitric oxide is a well-known vasodilatory mediator that allows pregnant women to attain lower peripheral resistance through vasodilation.56 There is also a systemic increase in vascular nitric oxide during pregnancy,56 which could further enhance vasodilation to the skin and assist pregnant women with the dissipation of heat. These proposed physiological mechanisms may explain the lack of association between prenatal exercise and congenital anomalies. However, we cannot speak to the sequential nature of this relationship as no studies included in this review investigated both outcomes together or examined exercise in a hot environment.
The regulation of fetal temperature at rest relies on the maternal–fetal gradient, whereby the fetus maintains a temperature of ~0.6°C above the maternal core temperature due to elevated fetal metabolism which results in heat transfer to the mother.57 It has been suggested that prenatal exercise may reverse the fetal to maternal temperature gradient from the mother to the fetus if maternal temperature surpasses that of the fetus.58 There are, however, physiological adaptations during pregnancy that may aid in thermoregulation to prevent hyperthermia, such as increased maternal cardiac output, peripheral vasodilation and increases in oestradiol (promoting vasodilation and heat dissipation) in the second and third trimesters.53 56 59 There is also a downward shift in the threshold for sweating as pregnancy progresses, which enables evaporative heat loss beginning at lower temperatures.37
Strengths and limitations
We used rigorous methodological standards (eg, GRADE) to guide the process of this systematic review and meta-analysis. Subgroup analyses were conducted to further elucidate the influence of duration and intensity of exercise on maternal temperature. The studies that provided information on the maternal temperature outcome also had several limitations. First, different measurement sites were used to assess body temperature (ie, rectal, skin oral and tympanic). In women, oral and mean tympanic temperatures tend to read below 37°C, while mean rectal temperatures are greater than or equal to 37°C.60 It has been suggested that the oral and rectal sites are acceptable for approximation of internal temperature.60 However, it is expected that the magnitude of temperature change (eg, from rest to exercise, and rest to postexercise) would be comparable between modes of measurement. Maternal temperature was evaluated during different modes of exercise, and 5 out of 15 studies involved exercising in water.34 39 43 44 46 However, only three of five studies assessed the acute change in temperature while the woman was immersed in water.39 44 46 Although thermoregulation mechanisms in the water are not fully understood, evaporative heat loss may be impaired in the water or heat dissipation enhanced due to increased conductivity of water (as long as the water is thermoneutral; 32°C and 35°C).58 Finally, the quality of evidence from studies included in our meta-analyses was ‘very low’ to ‘low’, which indicates limited confidence in the results.
Studies that provided information on the congenital anomalies outcome also had several limitations. The primary limitation was the paucity of exercise-only interventions which prohibited direct assessment of the independent impact of exercise on the odds of anomalies. Further, there were four intervention studies starting as early as the first trimester, preventing us from analysing the odds of congenital anomalies with prenatal exercise early in pregnancy. Congenital anomalies were also not defined consistently across all studies included in this review, and it was therefore impossible to determine if all included studies were consistent in the outcomes they reported under the umbrella term of ‘congenital anomalies’. Compliance with the interventions was poorly reported, which may limit the scope of our results. Further, there was a lack of information regarding the impact of repeated bouts of exercise, as well as the impact of exercising above versus below recommended levels of 150 min of moderate-intensity exercise each week.7 However, as the observed increase in temperature with exercise was minimal and well below hyperthermic thresholds, it is unlikely that exercise-induced temperature increases cause congenital anomalies.
Conclusions
Overall, there was consistent evidence that prenatal exercise did not increase the odds of congenital anomalies. In addition, exercise in the second and third trimesters was found to induce a small increase in maternal body temperature that did not reach hyperthermic levels and may therefore be considered safe for the fetus. Additional high-quality studies specifically investigating maternal temperature in the first trimester are needed.
What is already known
Hyperthermia in pregnancy from exposure to external heat sources during the preimplantation stage is associated with spontaneous abortion or congenital anomalies.
In non-pregnant populations, exercise is known to increase core body temperature.
Whether prenatal exercise induces a similar sustained increase in maternal core body temperature is not well understood.
What are the new findings
These data suggest that moderate-to-vigorous prenatal exercise does not induce hyperthermia or increase the odds of congenital anomalies.
However, most studies investigated exercise responses after 12 weeks’ gestation when the risk of de novo congenital anomalies is negligible.
Acknowledgments
The authors wish to acknowledge Mary Duggan from the Canadian Society for Exercise Physiology which is the primary knowledge user for the Canadian Institutes of Health Research Knowledge Synthesis Grant. We also thank Anne Courbalay and Bailey Shandro for their assistance with the systematic review.
References
Footnotes
Contributors MHD, SM-R, MFM, GAD, KBA contributed to the conception of the study. MHD, SM-R, MFM, GAD, KBA, AJG, NB, VJP, CEG, LGS, RB contributed to the design of the study and development of the search strategy. LGS conducted the systematic search. CY, AK, RJS, VLM, LR, FS, MJ, TSN, A-AM completed the acquisition of data. MHD, NB performed the data analysis. All authors assisted with the interpretation. MHD and CY were the principal writers of the manuscript. All authors contributed to the drafting and revision of the final article. All authors approved the final submitted version of the manuscript.
Funding This project was funded by a Canadian Institutes of Health Research Knowledge Synthesis Grant (140995). MHD is funded by an Advancing Women’s Heart Health Initiative New Investigator Award supported by Health Canada and the Heart and Stroke Foundation of Canada (RES0033140). RJS is funded by a Canadian Institutes for Health Research Doctoral Research Award (146252). A-AM is funded by a Fonds de Recherche du Québec – Santé Doctoral Research Award (34399).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.