Article Text

Abstract
Background No simple clinical measure exits to evaluate groin pain and its severity in athletes. The aim was to investigate the validity, reliability and responsiveness of a five-second hip-adduction squeeze test for football players designed to assess sports-related hip and groin function, pain and severity.
Methods Construct validity was assessed in 667 subelite male football players with a mean age (±SD) of 24±4 in the beginning of the season. Responsiveness and reliability were evaluated during the season in 52 and 10 players, respectively. Players answered the Copenhagen Hip and Groin Outcome Score (HAGOS) and performed the Copenhagen five-second squeeze assessed on a Numerical Pain Rating Scale (NRS) ranging from 0 to 10.
Results As hypothesised higher pain scores during the Copenhagen five-second squeeze correlated significantly (Spearman's rho=−0.61, p<0.01) with a lesser HAGOS (Sport) Score. The change scores in the Copenhagen five-second squeeze also correlated significantly (Spearman's rho=−0.51, p<0.01), with HAGOS (Sport) change scores in the responsiveness analysis, and test–retest reliability (concordance correlation coefficient) was 0.90. Moreover, significant (p<0.01) between-group differences existed for HAGOS (Sport) Scores in players reporting groin pain intensity at one of the 3 different pain levels: NRS (0–2), NRS (3–5) and NRS (6–10). The NRS (6–10) group had the lowest median (IQR) HAGOS (Sport) Score of 47 (31–61).
Conclusions The Copenhagen five-second squeeze is a valid indicator of sports-related hip and groin function in football players. Players reporting groin pain intensity as 6 of 10 or more in the Copenhagen five-second squeeze experience substantially impaired sports-related hip and groin function.
- Groin
- Hip
- Measurement
- Football
Statistics from Altmetric.com
Introduction
Hip and groin pain in football players can be a long-standing and debilitating condition.1 ,2 Its complex clinical presentation and multiple symptoms related to groin pain3 often impede sports health practitioners' ability to establish its severity and provide specific guidelines for optimal management.4 Several tests, such as tests for hip and groin pain strength, have been suggested as screening and management tools for evaluating readiness for play.4 These tests however require specific equipment and operational knowledge, and not all practitioners will be comfortable or able to use them.
In 2011, we developed a patient-reported outcome score. The Copenhagen Hip and Groin Outcome Score (HAGOS) is capable of measuring the severity of hip and groin pain and function specifically related to sports like football.5 This questionnaire includes 6 specific subscales and 37 questions and requires 10–15 min for testing the individual and calculating a score afterwards.5 For football players, the most interesting and relevant part is the sports-specific part (HAGOS—Sport), consisting of 8 questions and a subsequent score.5 Therefore, as several different hip and groin outcome scores exist, all recommended for younger to middle-aged individuals with hip and groin pain,6 it may be relevant to also include a clinically simpler and potentially more unifying approach.6 ,7 A simple and rapid approach is also highly relevant in a busy and hectic clinical setting to obtain measurements on a regular basis, involving no extra equipment, when assessing hip and groin pain status, severity and sports-related hip and groin function in football players. Different types of squeeze tests have been used for determining clinical entities or diagnoses.8 ,9 Recent research has documented that testing hip-adduction squeeze strength in supine position with resistance imposed between the ankles of the player9 ,10 provides the largest hip adductor moment11 and targets the adductor longus most efficiently.12 ,13 This test therefore seems able to provoke the commonly injured structure(s) around the symphysis in a manner that might be similar to strenuous sporting activity. It is easy to perform on footballers with no need for extra equipment and lasts only 5 s.
The primary purpose of the present study was to investigate whether this simple hip-adduction squeeze (The Copenhagen five-second squeeze test) is related to self-reported sports-related hip and groin function (HAGOS—Sport) in football players. We hypothesised that a strong negative correlation of ≥ −0.5 would exist between the Copenhagen five-second squeeze test and sports-related hip and groin function (HAGOS—Sport).
The secondary purpose was to investigate the responsiveness and reliability of this type of test, given that construct validity could be determined.
Methods
This study is based on data from a large cohort study investigating hip and/or groin pain,14 self-reported outcome,15 clinical characteristics, muscle strength, range of motion and radiological findings in male football players.16–19 All participants provided written informed consent according to the Helsinki Declaration. The Danish National Committee on Health Research Ethics (H-2-2010-127) approved the project. The reporting of the study follows the ‘Strengthening the Reporting of Observational studies in Epidemiology’ (STROBE statement).20
A total of 40 teams including 725 players were invited to join the baseline evaluation in the beginning of the season. To be included players had to be 18 years of age. Twenty-five participants failed to meet this inclusion criterion of being at least 18 years of age (n=10) or failed to answer the self-reported injury status questionnaire correctly (n=15). Thus, a total of 700 players, representing 40 teams (division 1–4) in Eastern Denmark, were eligible for the study. Football players were all playing at a subelite level. Players were asked to answer two self-reported questionnaires: (1) HAGOS5 and (2) a self-reported questionnaire concerning descriptive data and injury status, which is a questionnaire evaluating hip and/or groin disability5 that consists of six subscales (Symptom, Pain, Activities of Daily Living, Sports and Recreation, Participation in Physical Activities and Quality of Life). Each subscale is scored as a percentage of the total possible score, ranging from 0 to 100, where 0 indicates severe problems and 100 indicates no problems. It has proven to be valid, reliable and responsive for evaluating individuals with hip and/or groin pain, with the original study including a large proportion of male football players.5
At baseline, after fulfilling the two self-reported questionnaires, all eligible players also performed the Copenhagen five-second squeeze test. Teams were tested within the first 6 weeks of resuming the new season (July/August/September, 2011) before initiation of the training session. The Copenhagen five-second squeeze test is performed by placing one arm between the ankles of the player, instructing the player to isometrically and continuously squeeze as hard as possible for 5 s and subsequently rate the pain experienced in the groin during this manoeuvre on a 0–10 Numerical Rating Scale (NRS), with 0 representing no pain and 10 representing maximal pain (figure 1).

Numerical pain rating (0–10) during the Copenhagen five-second squeeze (right), and the traffic light approach (left). Red light indicates the player should STOP current football activity and should seek clinical workup by a health professional. Yellow light indicates ATTENTION, the player should be clinically reviewed by a health professional before football activity and participation level are decided on, and green light indicates GO for football activity and participation, but may in relation to return-to-football still need a clinical review by a health professional before deciding on the actual participation level.
Data collection was performed by observers from the Sports Orthopedic Research Centre—Copenhagen (SORC-C). Data collection sessions were performed with each team before or after a training session. Data included in the study were based on information as well as results of the Copenhagen five-second squeeze test of football players (all participants) at baseline and at a clinical examination (players seeking clinical examination and advice for treatment) later during the season. Clinical examination was offered to all participating players with hip and groin pain symptoms during the season, and all players could access this service by calling our staff office on the phone. Clinical examinations later during the season were obtained by a physiotherapist specialised in musculoskeletal and sports physiotherapy (KT) and were also used in a clinical study on MRI findings.16 Examinations and terminology used in the present study followed the clinical entity approach, as proposed by Hölmich et al,9 ,10 classifying groin injuries into adductor, iliopsoas and inguinal-related injuries. Reliability analyses only included players with similar symptomatic and functional states at baseline and follow-up. This was ensured by only including players in the test–retest reliability analysis of the Copenhagen five-second squeeze test that had a change in their score from baseline to follow-up assessment of 10 points or less, which is below the suggested minimal important change in a cohort seeking treatment for hip and/or groin pain.5 Floor and ceiling effects of the Copenhagen five-second squeeze test were established for players with an identifiable clinical entity at the follow-up visit, as they could be considered symptomatic.
Developmental process of the Copenhagen five-second squeeze test
The methodological framework for developing and evaluating the Copenhagen five-second squeeze test were in accordance with the COSMIN guidelines21–23 and included the following parts: (1) construct validity in a large football cohort and (2) determination of responsiveness, reliability and floor and ceiling effects in a smaller group of players from the same large cohort.
Construct validity
Construct validity refers to the degree to which the scores of a health measurement instrument are consistent with hypotheses in regard to relationships to scores of other instruments, or differences between relevant groups based on the assumption that the health measurement instrument used as a comparator validly measures the construct to be measured.23 Construct validity was studied by correlating the subscale scores of the Copenhagen five-second squeeze test with the subscales of the HAGOS. Construct validity was determined by a cross-sectional comparison of the Copenhagen five-second squeeze test and the HAGOS performed in the beginning of the season. We expected highest correlations when comparing scales measuring similar constructs. Since the Copenhagen five-second squeeze test is designed to measure pain during maximal adductor activation, we overall expected higher correlations between the Copenhagen five-second squeeze test and the HAGOS (Sport) subscale than any other subscales. Moreover, we hypothesised a correlation of at least −0.5 between the Copenhagen five-second squeeze test and HAGOS (Sport) subscale.
NRS ratings were also divided into three groups according to the pain monitoring model of Thomee;24 group 1: (NRS=0–2), which is considered safe, group 2, (NRS=3–5) considered acceptable, and group 3 (NRS=6–10), considered high risk. We investigated whether these three levels of pain experienced during the Copenhagen five-second squeeze test would yield different HAGOS (Sport) scores and hypothesised that there would be higher and thus better scores in individuals of group 1 compared to groups 2 and 3, and in group 2 compared to group 3.
Reliability, responsiveness and floor and ceiling effects
Test–retest reliability correlation coefficients should be ≥0.7 for the Copenhagen five-second squeeze.25 Included in the test–retest reliability analysis were only stable patients25 with a score change of 10 points or less, indicating a change less than the minimal important change.5 For responsiveness, which is the ability of a health measurement instrument to detect change over time in the construct to be measured,23 we hypothesised that the change in scores of the Copenhagen five-second squeeze test would correlate better with the HAGOS (Sport) subscale than any other subscales and with a correlation of at least 0.4.5
In this part of the study floor and ceiling effects were considered present if more than 15% of the players were reporting worst (0) or best (10) possible score.25 Only football players for whom a clinical entity could be identified at clinical examination were included in this analysis.
Sample size calculation
A sample size of more than 50 participants is sufficient to show correlations of −0.5 and−0.4, which are the correlation magnitudes we hypothesised would exist in analyses concerning validity and responsiveness, respectively, in the present study.
Statistical analyses
Descriptive values were presented as mean ±1 SD for parametric data and median IQR for non-parametric data. Spearman's rho was used for all correlation analyses on validity and responsiveness testing. Correlations of 0.5 were considered large, 0.3 moderate and 0.1 small.26 One-way analysis by ranks (Kruskal-Wallis) was used to detect differences between the three groups, and an independent measures test (Mann–Whitney) was used for comparison between sample pairs. The relative test–retest reliability was calculated using Lin's concordance correlation coefficient (CCC),27 ,28 because these data were not normally distributed and because this analysis is considered robust with as few as 10 pairs of data.27
Results
Figure 2 shows the full participant flow. Of the 700 players eligible for the study, Copenhagen five-second squeeze data could be obtained from 667 football players. These players had a mean age (±SD) of 24±4 years, mean (SD) height of 182±7 cm and mean (SD) weight of 79±9 kg. In total 11 subscales of 4002 (0.3%) could not be calculated. For responsiveness, reliability and floor and ceiling effects 52 players provided data on the Copenhagen five-second squeeze test at baseline and at the clinical examination later during the season. Here, 4 subscales (0.6%) of 624 could not be calculated.

Flow chart of the study process.
Of these 52 players, 39 were diagnosed with at least one clinical entity, and data from these players could be included for analyses of floor and ceiling effects.
Construct validity
Table 1 shows data from all correlation analyses. Increased groin pain intensity on the Copenhagen five-second squeeze correlated significantly with lower scores (HAGOS—Sport) (Spearman's rho=−0.61, p<0.01). There was also a significant correlation with the other subscales (Symptoms, Pain, Activities of Daily Living, Physical Activity and Quality of Life), ranging from Spearman rho=−0.51 to −0.60, p<0.01, but to a lesser degree than with the HAGOS (Sport). Furthermore, large numerical (>20 points) and significant (p<0.01) between-group differences existed for HAGOS (Sport) scores presented as median (25th and 75th centiles) in players reporting groin pain intensity at one of the three different pain levels: NRS (0–2), (Sports-scale) 97 (86–100), compared to players reporting NRS (3–5), HAGOS (Sport) 69 (56–84), again compared to players reporting NRS (6–10), HAGOS (Sport), median 47 (31–61), visualised in figure 3.
Correlations between Copenhagen five-second squeeze test and HAGOS in all players, and in a smaller group of players from the same cohort evaluated early (at baseline) and later in season

HAGOS scores in subgroups based on the Copenhagen five-second squeeze score. HAGOS, Copenhagen Hip and Groin Outcome Score; NRS, Numerical Rating Scale.
Responsiveness, reliability, floor and ceiling effects
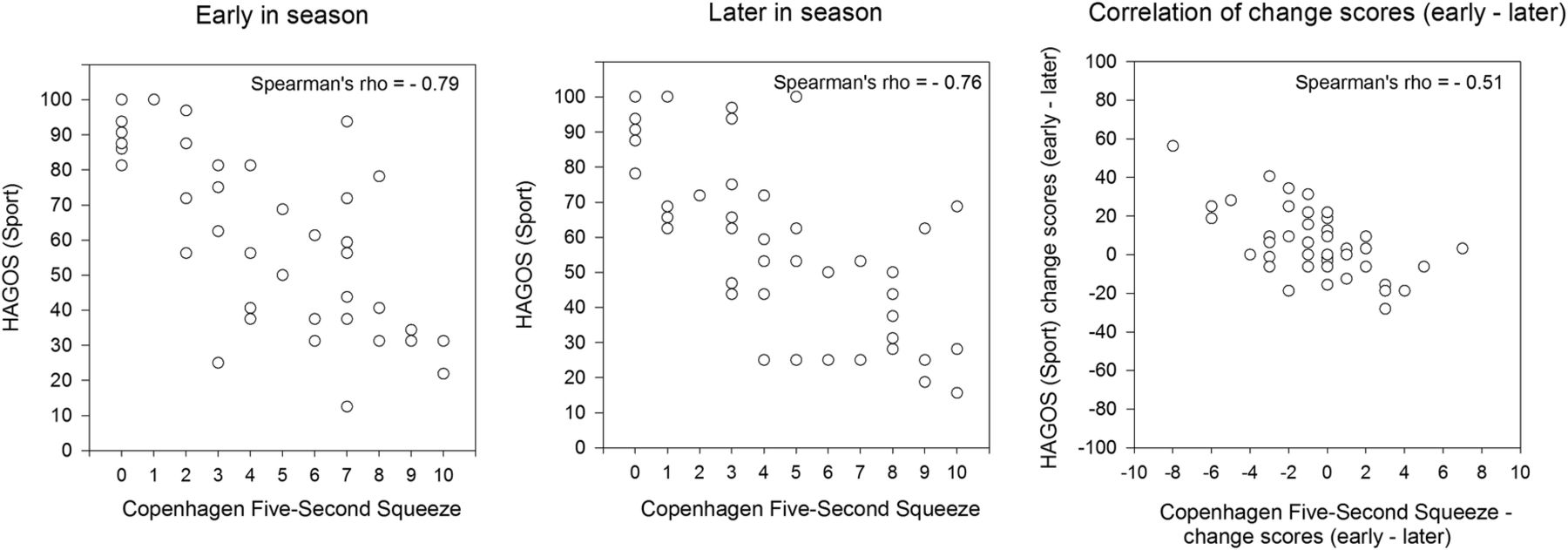
Increased groin pain intensity on the Copenhagen five-second squeeze correlated significantly with lesser HAGOS (Sport) scores early as well as later in the season (Spearman's rho=−0.79 and −0.76, p<0.01, respectively (n=52)). Change scores in the Copenhagen five-second squeeze correlated significantly with HAGOS (Sport) change scores (Spearman's rho=−0.51, p<0.01, figure 4), and to a higher degree than with all other change scores, except for (symptoms), which correlated −0.64, p<0.01, as shown in table 1. Test–retest reliability of the Copenhagen five-second squeeze test for football players with a stable hip and groin status (n=10) showed a CCC of 0.90 (CI 95% 0.67 to 0.97).

Correlation of scores and change scores for the Copenhagen five-second squeeze and HAGOS (Sport). HAGOS, Copenhagen Hip and Groin Outcome Score.
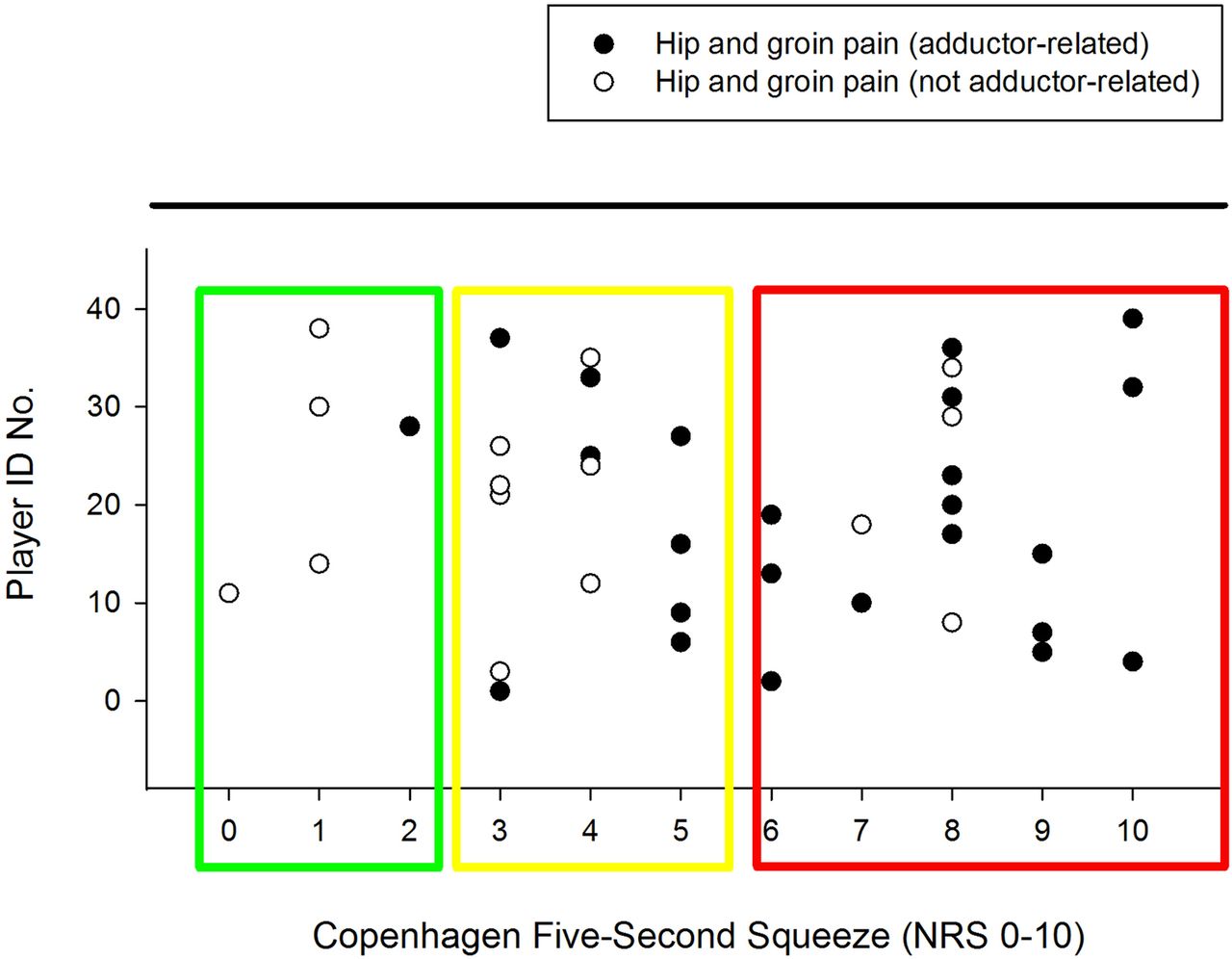
Floor or ceiling effects for the Copenhagen five-second squeeze test were only present in 4 (10%) of 39 patients presented in figure 5. Finally, a post hoc analysis revealed that football players with adductor-related groin pain had significantly higher Copenhagen five-second squeeze scores: median (IQR) 6.5 (5.0–8.8) than football players with other types of hip and groin pain median (IQR) 3 (1–7), p<0.01, with individual values most often (in 23 of 24 cases) exceeding the acceptable level (NRS >2) (figure 5). For players with adductor-related groin pain (n=24), a correlation of −0.56, p<0.01, was found when correlating the Copenhagen five-second squeeze to HAGOS (Sport), whereas this correlation was −0.64, p<0.05, in those with other types of groin pain (n=15).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Copenhagen five-second squeeze scores in football players with hip and groin pain seen at the clinical visit later during the season. Each player ID number refers to the number assigned to the individual football player during this visit. NRS, Numerical Rating Scale.
Discussion
In the present study, we set out to investigate whether a simple groin-pain test—the Copenhagen five-second squeeze—was related to HAGOS (Sport) and whether it could be considered a valid indicator of sports-related hip and groin function (HAGOS—Sport) in football players. Our a priori hypothesis that a strong negative correlation of ≥−0.5 would exist between the Copenhagen five-second squeeze test and sports-related hip and groin function (HAGOS—Sport) was confirmed.
Clinical relevance of the Copenhagen five-second squeeze test: implementing the red, green or yellow light approach for groin pain in male football
Large clinically relevant between-group differences (>20 points) existed for HAGOS (Sport) scores for players reporting groin pain intensity at the three different pain levels, NRS (0–2), NRS (3–5) and NRS (6–10). The present study suggests that these subdivisions can function as ‘traffic lights’. Red light clearly indicates STOP current football activity and seek clinical workup by a health professional. This is illustrated by those with a NRS of 6 or more and a corresponding median HAGOS (Sport) score below 50 points, which indicates severe disability, far outside the reference values of asymptomatic players,15 and at the level of football players seeking treatment for adductor-related groin pain19 ,29 or athletes with femoroacetabular impingement syndrome.30 ,31 Yellow light (NRS of 3–5) indicates ATTENTION, where the player should be clinically reviewed by a health professional before football activity and participation levels are decided on, as the HAGOS (Sport) median score of this group is just outside the reference values of asymptomatic players.15 We suggest that yellow light should be set to alert early clinical review and appropriate intervention in the form of load management and specific exercise prescription until symptom reduction has reached the acceptable level. Whether an NRS score of 0–2 in itself is a green light for football play remains debatable, it does however indicate that these players have experienced no or very minor hip and groin sporting-function restrictions, and as such offers a rapid screening for players that seem fit to play. This procedure may however be too simplistic to cover all important decision-making aspects of letting a player return to play. We therefore suggest that green light indicates GO for football activity and participation but may in relation to return-to-play still need a clinical review by a health professional before deciding on the actual participation level.
Measurement qualities of the Copenhagen five-second squeeze
The present study showed that the Copenhagen five-second squeeze test had good measurement qualities. Data on responsiveness and reliability were promising and the Copenhagen five-second squeeze displayed no signs of floor or ceiling effect in symptomatic players, suggesting that this tool could be used in clinical settings. This type of approach has never been validated before. The a priori hypothesis including directions and magnitude of correlations for the change scores were all met, with one surprising exception in regard to the higher numerical HAGOS (symptoms) correlation with the Copenhagen five-second squeeze test compared to the HAGOS (Sport). However, as the Copenhagen five-second squeeze test had negative correlations (higher than −0.4) for HAGOS (Symptoms) and HAGOS (Sport), the magnitude of these correlations still suggest that the Copenhagen five-second squeeze test is related to relevant measures of hip and groin symptoms and function.
Methodological considerations and limitations
One limitation of the Copenhagen squeeze test can evidently be the potential under-reporting of groin pain symptoms by players during testing, when they realise that an NRS of six or more may imply cessation of football activity (partly or fully). This problem is, however, well known, and no different from players who report available for play when they already know they are injured. One possible manner to accommodate for this weakness in the Copenhagen five-second squeeze test would consist of including an objective measure of squeeze strength by applying a handheld dynamometer in the same position, and at the same time, as the Copenhagen squeeze is being conducted, as already tested for precision and torque production by Light and Thorborg.11 The latter clearly showed that the position of the Copenhagen five-second squeeze gives higher torque values than other frequently used squeeze testing positions, which may explain why this test is so useful and highly correlated to sports-related hip and groin function. By including a measure that includes subjective pain measure and objective force measure sports medicine practitioners could in the future test players rapidly before making valid decisions on cessation from play, instead of relying on information solely provided by players.
Reliability of a self-reported single question measure is obviously difficult, as recollection of previous response in a classical 1–3 week test–retest design is inevitable. For this reason, we believe that including those with a condition, predefined by clinically irrelevant changes on all subscales from test to retest, could make up for this limitation. We have thereby included data from players unaware that they would be used in a test–retest reliability analysis. As several weeks passed between test and retest, we believe recall bias must have been very limited. We could only include 10 players in the test–retest reliability. Considering the small sample size a CCC of 0.90 seems very promising in terms of obtaining precise information from players.
Post hoc analysis indicates that players with adductor-related groin pain have higher Copenhagen five-second squeeze scores (more pain) than players with other types of groin pain. However, when correlating the Copenhagen squeeze with HAGOS (Sport) in subgroups of players with adductor-related groin pain and the subgroup of players suffering from other types of groin pain, a large significant correlation was still obtained in both groups, suggesting that the Copenhagen five-second squeeze relates to sports-related hip and groin function irrespective of groin pain diagnosis/entity. However, caution is needed when interpreting these analyses, as they were conducted post hoc and only included 24 players with adductor-related groin pain and 15 players with other clinical entities, respectively.
We hope that others will test this tool in sports known to elicit groin pain and attempt to replicate our findings. Furthermore, future research on predictive and prescriptive validity of the red, green or yellow light approach in relation to injury/re-injury and loading/treatment strategies, respectively, would be of high clinical relevance. The clinical advantage of this tool is evident: it only takes 5 s to perform, it includes a real live snapshot of the current groin pain status during a standardised, active and relevant maximal effort and it does not require any specific equipment or data handling afterwards.
Conclusions
The Copenhagen five-second squeeze is a rapid and valid indicator of sports-related hip and groin function, and in situations where football players report groin pain intensity of 6 or more on this test substantially impaired sports-related hip and groin function is indicated. Furthermore, the Copenhagen five-second squeeze is a highly responsive and reliable measure that can be used as a continuous indicator of sports-related hip groin function and as a ‘traffic light’ in the management of footballers with groin pain.
What are the findings?
The Copenhagen five-second maximal squeeze is a rapid and valid indicator of sports-related hip and groin function in footballers.
The Copenhagen five-second squeeze is a valid, reliable and responsive measure of sports-related hip and groin function in football players with hip and groin pain.
Players reporting groin pain intensity as 6 of 10 or more in the Copenhagen five-second squeeze experience substantially impaired sports-related hip and groin function.
How might it impact on clinical practice in the future?
In ongoing monitoring and assessment of male footballers with and without groin pain, the Copenhagen five-second squeeze will hopefully be routinely included from now on, as it is a very rapid and easy procedure, that captures relevant restrictions in sports-related hip and groin function.
Being novel and rapid, the Copenhagen five-second squeeze is also a promising research tool in future research on groin pain in athletes, especially when testing large football cohorts, and in situations where testing is difficult due to time and location-related restraints.
Acknowledgments
The authors are thankful to the participating clubs and to Michael Hansen and Lasse Lundquist for assisting with the data collection.
References
Footnotes
Contributors KT contributed to the original idea of this study and the design and drafted the manuscript. Analysis of the data was performed by KT, and all authors revised and consented to the design, discussion and conclusion sections in the paper concerning the data. All authors commented and contributed with important intellectual content and final approval of the version to be published.
Funding MPN was funded by the Lundbeck Foundation on a pregraduate scholarship during the time he was involved in the current study.
Competing interests None declared.
Ethics approval The Danish National Committee on Health Research Ethics (H-2-2010-127) approved the project.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Statistical analyses and data sets are available from the corresponding author.