Article Text

Abstract
Background Vertical ground reaction force (VGRF) parameters have been implicated as a cause of several running-related injuries. However, no systematic review has examined this relationship.
Aim We systematically reviewed evidence for a relation between VGRF parameters and specific running-related injuries.
Methods MEDLINE, Web of Science and EMBASE databases were searched. Two independent assessors screened the articles and rated the methodological quality. The 3 key VGRF parameters we measured were vertical loading rate, impact/passive peak (Fz1) and propulsive/active peak (Fz2). Standardised mean differences of these parameters were calculated using a random-effects model. Meta-regression was performed using injury type, study type and methodological quality as factors.
Results The search yielded 2016 citations and 18 met the inclusion criteria for the systematic review. The loading rate was higher in studies that included patients with a history of stress fractures and patients with all injury types, both compared with controls. Only studies that included patients with a history of symptoms at the time of kinetic data collection showed higher loading rates overall in cases than in controls. There were no differences between injured subjects and controls for the active and passive peaks of the VGRF.
Summary The loading rate is higher in respondents with a history of stress fractures than in respondents without running injuries. Owing to the absence of prospective studies on other injury types, it is not possible to draw definite conclusions regarding their relation with loading rate.
- Running
- Biomechanics
- Meta-analysis
Statistics from Altmetric.com
Introduction
Overuse injuries such as medial tibial stress syndrome, patellofemoral pain syndrome, iliotibial band syndrome (ITBS), stress fractures, plantar fasciitis and Achilles tendinopathy are common among recreational and competitive runners.1 ,2 Many factors play a role in the aetiology of these running-related injuries. Anatomical and biomechanical factors influence the relation between training load and injury occurrence.3 ,4
Vertical ground reaction force (VGRF) is a biomechanical factor that has been often studied during running. It provides a fairly crude biomechanical measure during running as it neglects the distribution of forces and moments within joints and tissues, but it has the advantage of requiring only a force platform or an instrumented treadmill is needed and no advanced mathematical modelling. Commonly calculated VGRF parameters are loading rate (LR), impact/passive peak (Fz1) and propulsive/active peak (Fz2) (figure 1).

Graphic representation of a typical VGRF profile and the main parameters (LR, loading rate; VGRF, vertical ground reaction force).
If any VGRF parameters predicted running-related injuries, it would provide a potential avenue to reduce injuries as gait retraining can reduce VGRF parameters and these reductions are still present after 1 month.5–8
Whether or not there is a relationship between VGRFs and running-related injuries is unclear. A review by Zadpoor and Nikooyan9 showed that a relation exists between a high LR of the VGRF and stress fractures. On the other hand, some studies found no relation between a high LR and running-related injuries.10 ,11
Therefore, we systematically reviewed the evidence for a relation between VGRF parameters and specific running-related injuries. We also performed a meta-analysis dividing ‘running injuries’ into specific tissue diagnoses (such as ‘stress fracture’, for example).
Methods
Search strategy and inclusion criteria
A search of the MEDLINE, Web of Science and EMBASE databases was conducted in July 2015 by two investigators (HvdW, JWV). The search strategy can be found in online supplementary appendix 1.
Studies were included in the present study if: (1) they compared a group of healthy runners with a group of runners who had a running-related injury or a history of it, or if a group of healthy runners was followed over time and data on running-related injuries were collected during that period; (2) VGRFs were measured during running on running shoes using a treadmill or force plate and (3) the article was written in English (congress abstracts were excluded).
The same two researchers independently screened the articles starting with titles and abstracts and, if necessary, full texts. References of included studies were checked for additional articles that did not appear in the search.
Data extraction
Data on study design and study population were extracted from the articles, as were means and SDs of LR, impact forces (Fz1) and active forces (Fz2) for both groups. When SEs were reported, these were converted into SDs.12 Data were extracted by two researchers (HvdW, JWV). When it was not possible to extract the data from an article, the authors were contacted by email to obtain the data. If this failed and data were presented in a figure in the article, the data were extracted from this figure by measuring the values using a custom code written in Matlab (MATLAB 2014a, The Mathworks, Inc, Natick, Massachusetts, USA). Pixel data from the (error) bars and the scale were extracted, and VGRF values were calculated by converting the pixel data of the bars using the scale data.
Methodological quality assessment
The methodological quality of the included studies was rated by two researchers (HvdW, JWV) with a methodological quality checklist developed by Downs and Black.13 The checklist has been used before to study the relation between biomechanical factors and sports injuries.14 ,15 The 12 items relevant for cohort and case–control studies were scored by the two researchers. Items related to reporting of the study (items 1–4, 6 and 7), external validity (11, 12) and internal validity (16, 18, 20, 25) were selected. Items applicable to systematic reviews without meta-analysis and reviews on intervention studies were not selected. Any difference in quality assessment between the two reviewers was resolved by a consensus meeting.
Data pooling
Data of LR, Fz1 and Fz2 were pooled in R (V.3.1.2) using the metafor package (V.1.9–5).16 ,17 A random-effects model was used to calculate the standardised mean difference with 95% CIs and heterogeneity.
A random-effects meta-regression was performed with injury type, study design and methodological quality as factors. For each factor, an omnibus test for all coefficients was performed (Q statistic). Classification of injuries into injury types was carried out on the basis of clinical reasoning. Studies were classified into high or low methodological quality on the basis of the score on the Downs and Black list (>70% vs ≤70%, respectively). A p value of <0.05 was accepted as statistically significant.
Results
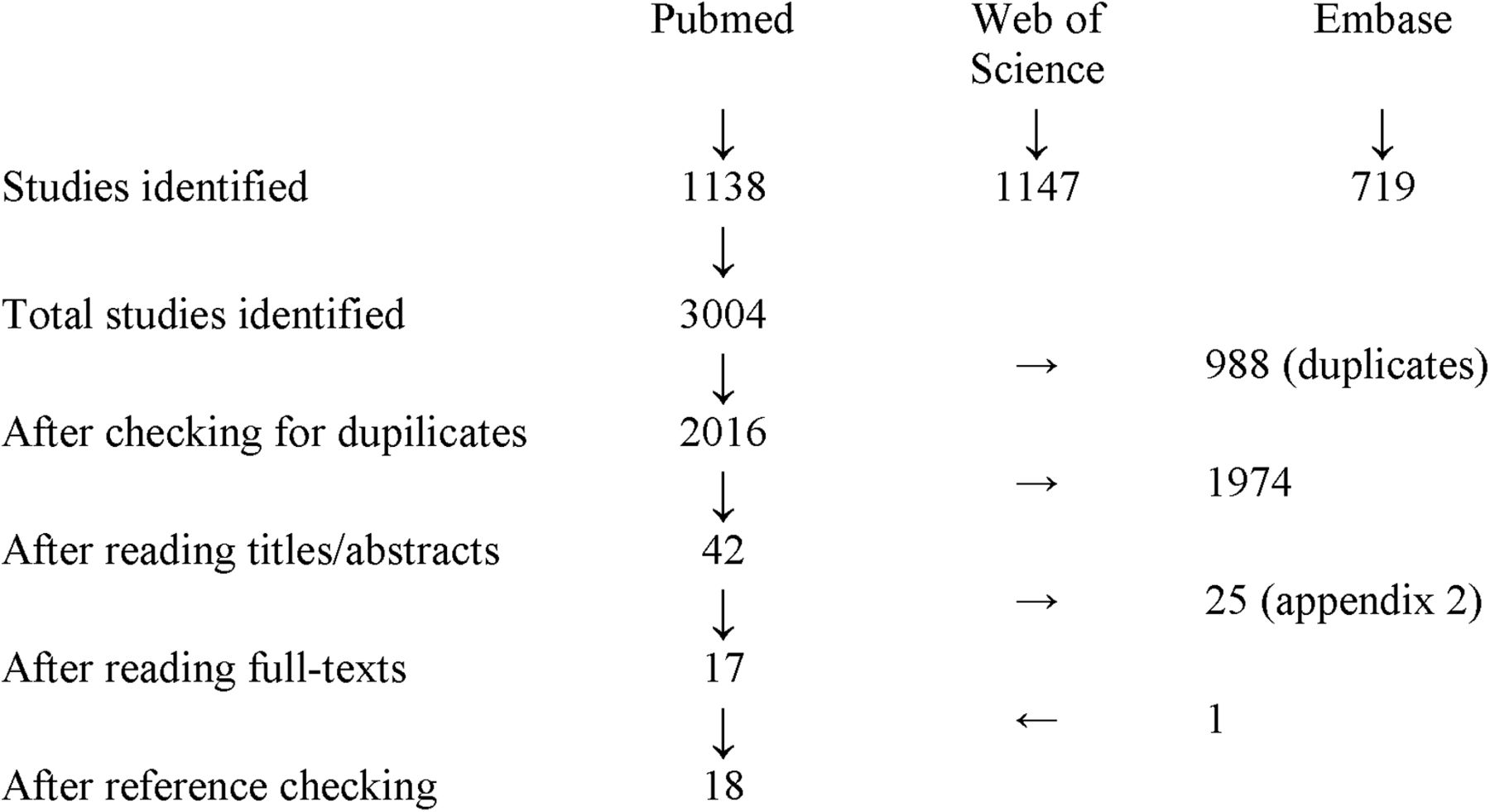
The search resulted in 2016 studies after removing duplicates. After screening the titles and abstract, 42 were identified as potentially relevant (figure 2). Subsequently, the full texts of these 42 articles were screened and 17 studies (table 1) were selected for the review (excluded studies including reasons for exclusion can be found in online supplementary appendix 2). One article was included after reference checking.18 Of the 18 included studies, 2 did not present exact values of the VGRF parameters (means and SDs/SE). One of these studies only presented p values and the other only presented values in a figure.19 ,20 Authors of both papers were contacted to retrieve the exact values of the VGRF variables: data of one study were retrieved from the author,19 but no data could be retrieved for the other study,20 so those data (mean of both legs) were extracted from the figure presented in the article. One study collected prospective and retrospective data in a cohort of runners before and after an exhaustive run.21 From this study, only the prospective collected injury data and VGRF data from before the exhaustive run were included in the review. From one study that included a minimalistic shoe condition and a running shoe condition, only the running shoe condition was included.19 The study by Bredeweg et al22 collected data at several speeds that were different for males (9 km/h and 10 km/h) and females (8 km/h and 9 km/h); since all participants ran at 9 km/h, this condition was included in the meta-analysis.
Characteristics of the included studies
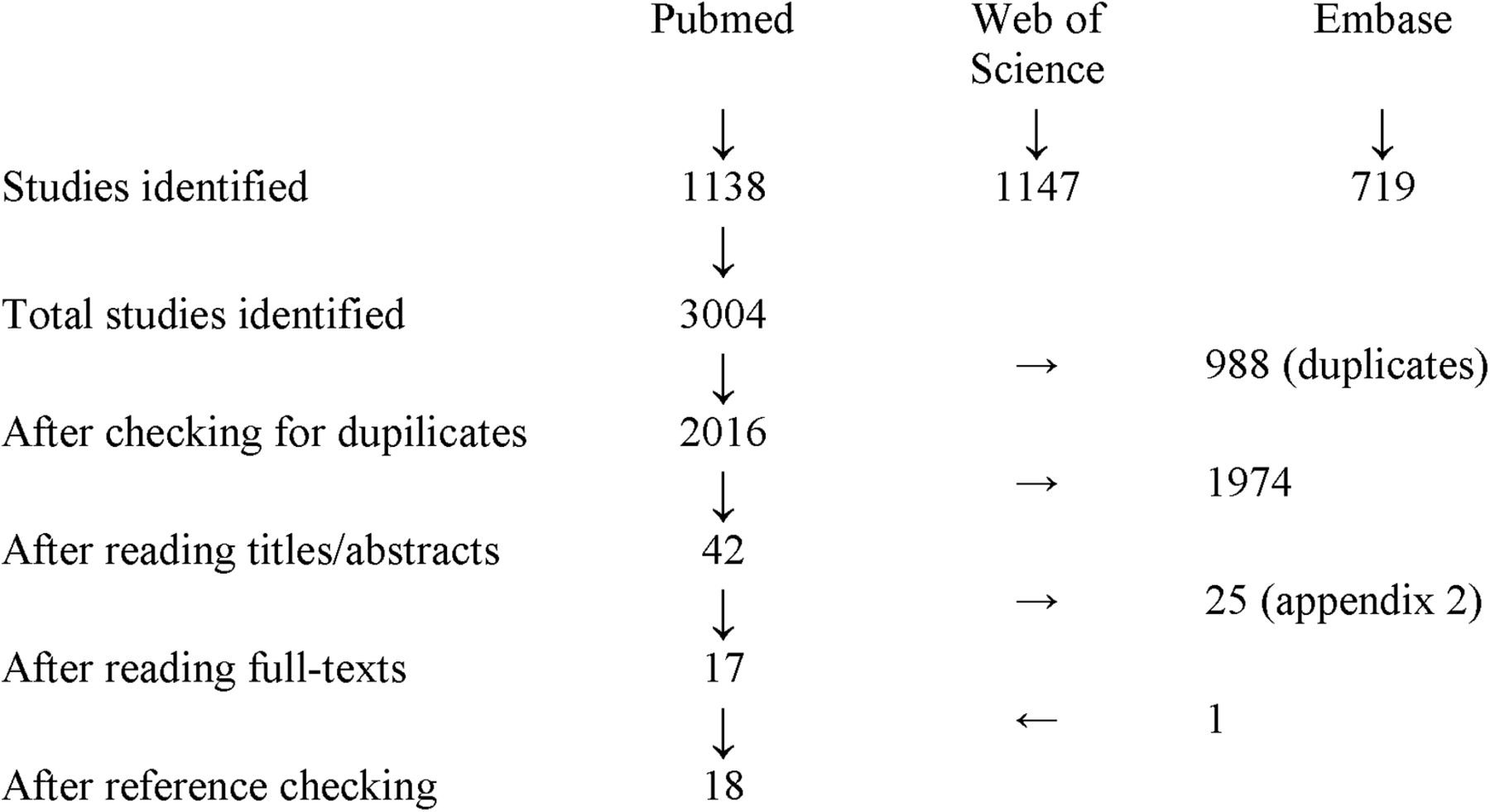
Flow chart of the search and screening process.
Study characteristics
The characteristics of the studies are presented in table 1. On the basis of the injury type, studies were categorised into five categories: (1) tendinopathy (Achilles tendinopathy and plantar fasciitis),10 ,19 ,23 ,24 (2) stress fractures (metatarsal, tibial and femoral),18 ,20 ,25–29 (3) anterior knee pain (AKP; including patellofemoral pain syndrome),30–32 (4) ITBS11 and (5) studies that included all running-related injury types.21 ,22 ,33 Of the 18 studies, there were 13 on LR, 15 on Fz1 and 14 on Fz2. Nine studies reported peak LR, but for four studies it was not clear whether peak or mean LR was calculated.11 ,21 ,30 ,32 All studies scaled the reported VGRF data to body weight.
Participants
A total of 1172 participants were included in the 18 studies (676 controls, 496 cases). LR was assessed in 1031 participants (594 controls, 437 cases), Fz1 in 1047 participants (611 controls, 436 cases) and Fz2 in 935 participants (562 controls, 373 cases).
Pooled data
Loading rate
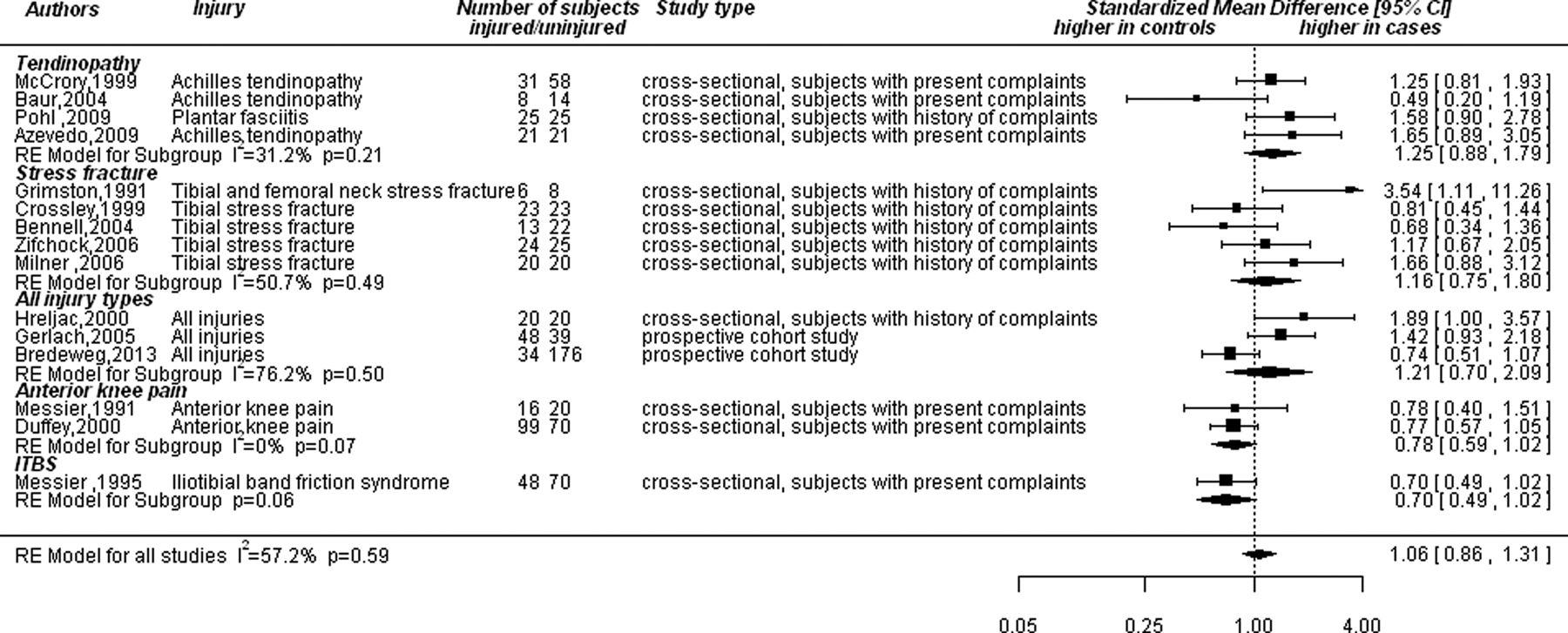
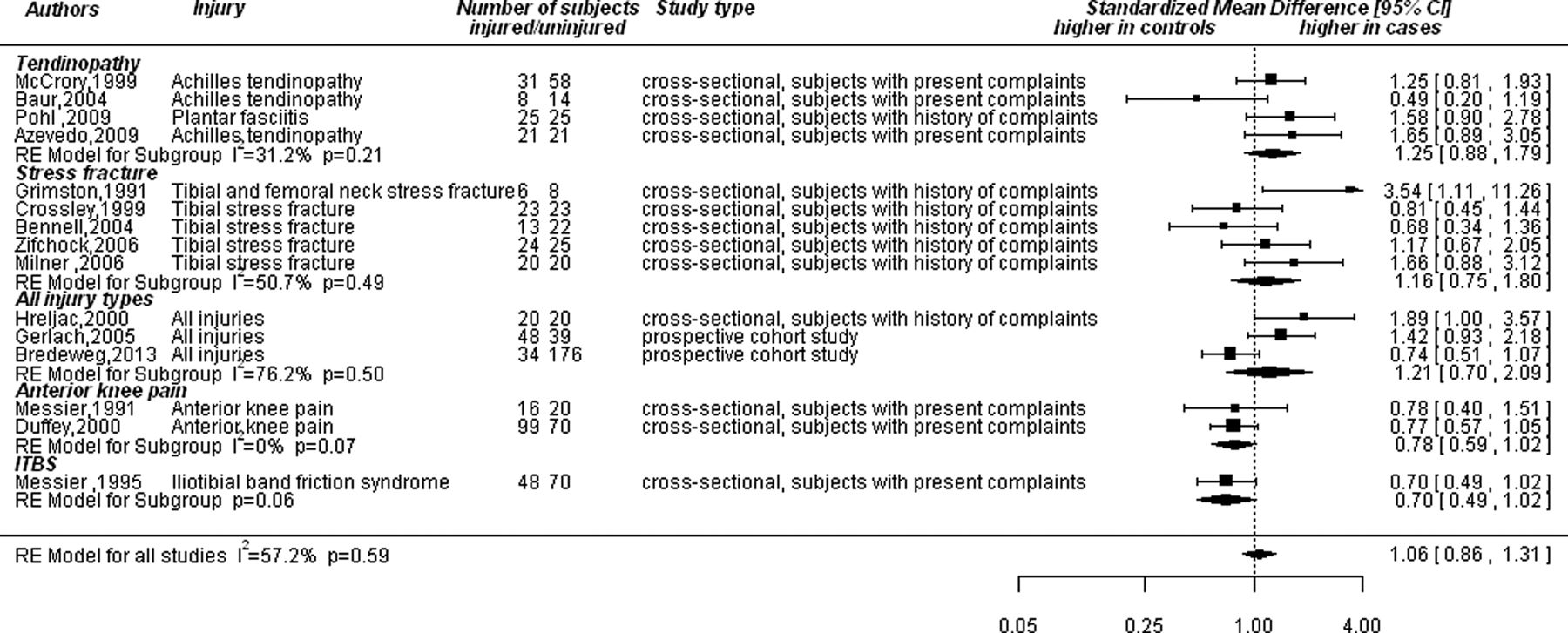
LR was not significantly higher in patients than in controls when all studies were pooled together (figure 3), although this comparison approached significance (p=0.09). LR was higher in patients with a history of stress fractures and in patients with all running-related injury types included into a single study. The mean difference in LR between groups in the four studies on stress fractures was on average 12%. No differences were found between controls and subjects with tendinopathy, AKP or ITBS.

Forrest plot of the LR for all injury categories (ITBS, iliotibial band syndrome; LR, loading rate).
Compared with controls, LR was higher in studies that included patients with previous symptoms; this difference was not found in studies that included patients with existing symptoms nor in prospective studies (figure 4).

Forrest plot of the loading rate sorted by study type.
When both factors, injury type and study type, were included in the analysis simultaneously, neither had an influence on the LR differences (injury type: Q=4.22 (df=4), p=0.38; study type: Q=3.64 (df=2), p=0.16). However, there was interdependence between the factors as all studies that investigated stress fractures and all running-related injury types included exclusively participants without existing symptoms (previous symptoms and prospective studies) and all but one study that investigated tendinopathy, AKP and ITBS included exclusively patients with existing symptoms.
Impact peak (Fz1)
There was no difference in Fz1 between controls and patients in general, nor for any of the injury categories (figure 5). Study type (Q=2.77 (df=2), p=0.25, I2=55.1%) did not influence the results.
Forrest plot of the passive peak (Fz1) for all injury categories (ITBS, iliotibial band syndrome).
Active peak (Fz2)
None of the injury categories showed a difference between controls and patients in magnitude of Fz2 and nor was there a general difference (figure 6). Study type had no significant influence on the outcome (Q=0.43 (df=2), p=0.81, I2=36.8%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forrest plot of the active peak (Fz2) for all injury categories (ITBS, iliotibial band syndrome).
Methodological quality
Results of the methodological quality assessment are shown in table 2. For sensitivity analyses, studies with a low methodological quality score (≤70%, n=3) were compared with those with a high methodological quality score (>70%, n=15). Methodological quality had no influence on the outcomes of the meta-analysis for LR (Q=0.08 (df=1), p=0.78), Fz1 (Q=0.18 (df=1), p=0.66) and Fz2 (Q=3.56 (df=1), p=0.051). Studies with a low methodological score showed a tendency for a larger difference in Fz2 between cases and controls, but this could be attributed to a single study.18
Methodological quality assessment of the included studies
Discussion
LR was higher in patients with a history of stress fractures as well as in studies that included patients with all running-related injury types, both compared with controls. The LR of the VGRF was not significantly higher in patients with other running-related injuries. The finding for a relation between loading and stress fractures was in line with a previous review.9 Differences in LR between patients with a history of stress fractures and controls were 10–15%. No differences in LR between cases and controls were found in studies that only included participants with lower-limb tendinopathy, AKP or ITBS. No differences were found for impact (Fz1) and active peak (Fz2) between cases and controls. There was no difference between studies with a high and a low methodological quality.
Aetiological differences between injuries or methodological issue?
A first explanation for the present findings is that injury types may have different aetiologies, for example, those affecting bony structures (such as stress fractures) compared with soft-tissue injuries,34 or injuries related to running pace compared with injuries related to changes in running volume.35 Of the three studies that included multiple types of injuries, only one gave a description of the included injury sites.22 The largest group in this study was that of participants with knee injuries (41%) and it showed the smallest difference between cases and controls of the three studies. This study included novice runners, whereas the other two studies that included all injury types included experienced runners.21 ,33
Although these studies did not provide an overview of the included injury type, it is known that experienced runners report a lower proportion of knee injuries, compared with novice runners, and a higher proportion of foot injuries.2 So the study with a high proportion of knee injuries22 found smaller differences between cases and controls compared with the studies that possibly included a higher percentage of foot injures.21 ,33 This seems to be in line with the studies on knee injuries, and also with the study of Pohl et al (2009) on plantar fasciitis,24 where LR was higher in cases. Therefore, aetiological differences may be an explanation for the present findings.
A second explanation for the findings is that studies on tendinopathy, AKP and ITBS included almost exclusively participants who had symptoms at the time of data collection. This may have influenced the results as these participants may have altered their running pattern because of pain or discomfort towards a pattern characterised by reduced LRs. It is possible that prospective studies on these injuries will find differences between controls and cases.
Differentiating between these two explanations is not possible because injury type and study design were not independent of each other; studies on stress fractures and all running-related injury types included participants without symptoms at the time of data collection, whereas the other studies included participants with symptoms at the time of data collection. Therefore, further research is required to resolve this issue.
Clinical relevance
The present results indicate that reducing the LR of the VGRF may reduce the risk of stress fractures. Some studies have already shown that the LR of the VGRF can successfully be reduced following a gait retraining programme that uses feedback on tibial peak acceleration,6 and step frequency.8 LR reductions were still present 1 month after retraining in two of these studies,6 ,8 but not in the other.36 Also, the LR of the VGRF itself may be used as a target variable that is provided to runners as feedback during gait retraining. The use of reducing the LR for treatment and prevention of injuries other than stress fractures is not supported by the current result. Another issue is that the results suggest that the presence of symptoms reduces the LR. So in these participants, a LR reduction is already achieved. This may indicate that gait retraining should aim at patients who have partially recovered and are free of symptoms. Further research on the use of gait retraining for the treatment of running-related injuries is required as there is still a missing link between biomechanical adaptations following gait retraining and the resolution of running-related injuries.
Regarding prevention, several running styles, such as Chi running,37 Pose running,38 forefoot striking39 and running with a high step frequency,7 have been associated with lower LRs compared with conventional rearfoot striking. This is in line with a simulation study that showed that foot angle at initial contact had a large influence on LR.40 Landing on the heel with a dorsal flexed ankle resulted in a higher LR. Horizontal velocity at initial contact also exerted a large influence on the LR. Hence, these running style adaptations may help prevent running-related injuries. High LRs are not the only factor that plays a role in the development of running-related injuries, however, so an exclusive focus on LRs should therefore be avoided. Further research is required to investigate the consequences of running style adaptations.
Strengths and limitations of the review and meta-analysis
The present meta-analysis has some limitations. We mostly identified case–control studies and only two prospective studies.21 ,22 Therefore, the direction of the relation between injury and running style is unclear. However, by differentiating between studies that included runners with existing symptoms and studies with runners with no existing symptoms, it was possible to hypothesise about this relation. Pain may lead to lower LRs, whereas higher LRs increase the risk of injury. Furthermore, most studies did not state from which population the participants were recruited, which may lead to bias in generalising the results. A further limitation was the assessment of the methodological quality. The checklist that was used included only a part of the items from the original checklist by Downs and Black. The validity and reliability of the checklist may therefore be changed. Also, some items have been shown to have poor reliability. Therefore, the results of the sensitivity analysis should be interpreted with caution. On the other hand, no well-suited instruments to rate the methodological quality of biomechanical studies are available at the moment. Another limitation is that VGRFs do not reflect the forces and moments within the body. For this reason, it is not possible to draw conclusions about the exact injury mechanism. On the other hand, since VGRFs are easy to measure, they are very well suited as target variables in gait retraining.
Summary
LR is higher in patients with a history of stress fractures. A higher LR in injured runners was also found in studies that included all running-related injury types. Owing to differences in study design, it is not possible to draw definite conclusions regarding the relation between LR and these other running-related injury types. No differences between cases and controls were found for impact peak and active peak.
What are the findings?
A high loading rate of the vertical ground reaction force was found in patients with a history of stress fracture.
It is possible that a high loading rate of the vertical ground reaction force also has influence on the development of other running-related injuries, but at the moment it is not possible to distinguish between the effects of injury type and study design.
How might it impact on clinical practice in the future?
Reducing the loading rate of the vertical ground reaction force by 10–15% may help in prevention and treatment of stress fractures. Several running adaptations have been described that may achieve such a reduction.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement 1
- Data supplement 2 - Online supplement 2
Footnotes
Contributors HvdW and SWB designed the study. HvdW and JWV executed the search, screened the articles, extracted the data and rated the methodological quality of the studies. HvdW performed the analysis and drafted the manuscript. All the authors interpreted the data. JWV and SWB revised the manuscript and approved the final version.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Warm up