Article Text

Abstract
Background The role of inflammation in tendinopathy has historically been a subject of significant controversy. Our primary aim was to determine whether inflammatory cell numbers were increased in painful human tendinopathy versus healthy control tendons. Our secondary aim was to assess whether the inflammatory cells had been linked with symptoms or disease stage.
Methods We conducted a systematic review of the scientific literature using the PRISMA and Cochrane guidelines of the Medline database using specific search criteria. Only studies measuring inflammatory cells using specific markers in tissue from human patients with the clinical diagnosis of tendinopathy were included. Inclusion was agreed on by 2 independent researchers on review of abstracts or full-text using specific predetermined criteria. The search yielded 5 articles in total.
Results There were increased numbers of macrophages (4 studies) and mast cells (3 studies) in tendinopathic versus healthy control tissues. One study demonstrated increased numbers of T cells in tendinopathic tissue versus healthy control tendons. There were reduced numbers of T cells (1 study), macrophages (2 studies) and mast cells (2 studies) in torn tendon versus intact tendinopathic tissue.
Conclusions The existing evidence supports the hypothesis that increased numbers of inflammatory cells are present in pathological tendons. The lack of high-quality quantitative studies in this area demonstrates a clear need for future research to better understand the role of inflammation in tendinopathy.
- Tendon
- Tendinopathy
- Tendinosis
- Immunology
- Orthopaedics
Statistics from Altmetric.com
Introduction
Historically, many different words have been used to described tendon-related pathology including ‘tendinosis’ (implying degenerative aetiology), ‘tendinitis’ (implying inflammatory aetiology) and the recently favoured and less aetiologically specific ‘tendinopathy’.1 This diversity of language reflects this historical disagreement within the scientific community as to the exact role of inflammation in the aetiology of tendinopathy. To contribute to this debate it is important to be precise in terms of one's language, meaning that a sensible way of starting is to define what can be meant by ‘inflammation’ and ‘inflammatory cells’.
In the first century ad, the Roman scholar Celsus described the clinical features of ‘inflammation’ as calor (heat), dolor (pain), rubor (redness) and tumour (swelling). Subsequently, definitions of inflammation have developed and become more complex, reflecting our deeper understanding of the role of inflammation and the way in which it may be involved in a huge variety of disease processes. For example, Ursula Weiss has recently described chronic inflammation in Nature as:2Chronic inflammation, by contrast, is a prolonged, dysregulated and maladaptive response that involves active inflammation, tissue destruction and attempts at tissue repair. Such persistent inflammation is associated with many chronic human conditions and diseases, including allergy, atherosclerosis, cancer, arthritis and autoimmune diseases.
This definition communicates the diversity of chronic diseases in which the role of inflammation has become better understood in recent years, in which Celsus’ clinical features of inflammation are frequently absent or rather subtle. Despite progress, the role of ‘inflammation’ is still far from fully understood. For example, even in a classic ‘inflammatory’ disease such as rheumatoid arthritis in which the synovitis involves a massive inflammatory cell infiltrate associated with augmented angiogenesis, we are far from having a complete understanding of the pathogenesis of the disease.3
The pathological findings in tendinopathy have been described by a large number of studies over the years.4–8 The extracellular matrix changes are characterised by a loss of collagen organisation, fibrocartilagenous change, and glycosaminoglycan deposition. The cellular changes include increases in the overall cellularity, the variation in cellularity, and cell rounding. Notably, there remains a paucity of evidence relating to phenotyping the ‘tenocyte’ in healthy human tendon and the enthesis.
There is no consensus on defining exactly what an ‘inflammatory cell’ is, however, ‘inflammatory cells’ may be reasonably defined as polymorphonuclear leucocytes (PMNs which include neutrophils), monocytes/macrophages, mast cells and T cells.9 The presence of ‘inflammatory cells’ in tendinopathy is controversial. Some descriptive histological studies have described the total absence or presence of ‘inflammatory cells’ using basic histological techniques without the use of specific cell markers, however, these descriptive findings have often related to the absence of acute inflammation in the form of PMNs. As our understanding of chronic inflammation has developed alongside new immunohistochemical techniques,10 it has become increasingly clear that the absence of PMNs cannot be equated to mean the total absence of inflammation.1 Recent reviews have proposed more a role for inflammation in the pathogenesis of tendinopathy.1 ,11
In this context, our primary aim was to determine whether inflammatory cells are increased in painful human tendinopathy versus healthy control tendons. Our secondary aim was to assess whether the presence of inflammatory cells has been linked with symptoms or the degree of structural tendon failure. By asking these research questions and using the objective methodology of a systematic review, we aimed to summarise our current understanding of the role of ‘inflammatory cells’ in tendinopathy, and to define how future studies should be designed in order to further answer these questions.
Methods
Search strategies
This systematic review used the PRISMA Statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and the Cochrane handbook as guidelines in the development of the study protocol, and the report of the current study. The inclusion criteria and methods of analysis were specified in advance and documented in a protocol. Studies were identified using the Medline electronic database. No limit was placed on year of data entry, but in practice, there were no results prior to 1942. The search was undertaken in January 2015. The following search term were used: tendinosis OR tendinitis OR tendinopathy. Additional studies were located by searching papers referenced in listed articles. The studies identified by the searches were combined and duplicates excluded. The abstracts were initially screened before analysis of the selected full-text articles. Full inclusion/exclusion criteria are detailed in the online supplementary appendix 1.
Studies had to relate to human tendinopathy and had to relate to the quantification/semiquantification of inflammatory cells. The quantification/semiquantification of inflammatory cell numbers had to involve the use of specific cell markers as defined by the individual studies. Review articles and case studies were excluded. Studies which used only descriptive analysis and/or no specific inflammatory cell markers were excluded. Studies without any kind of control group were excluded. If a study could not be obtained in English it was excluded.
The search, the selection of studies, and the data analysis were performed independently by two individuals (PG and BD). Agreement on inclusion was achieved after review of the full-text articles and a joint decision by both individuals based on the inclusion/exclusion criteria; if opinion was divided then a casting vote was given to SGD. The data were then extracted using a spreadsheet; this included data relating to study heterogeneity and methodological quality. The data extracted included patient characteristics, inflammatory cell markers used and cells used, method of tissue analysis, control group, results and statistical methods. Methodological quality was assessed using a 10-point scoring system (see online supplementary appendix 2) based on the method used by Dean et al.12
Study selection
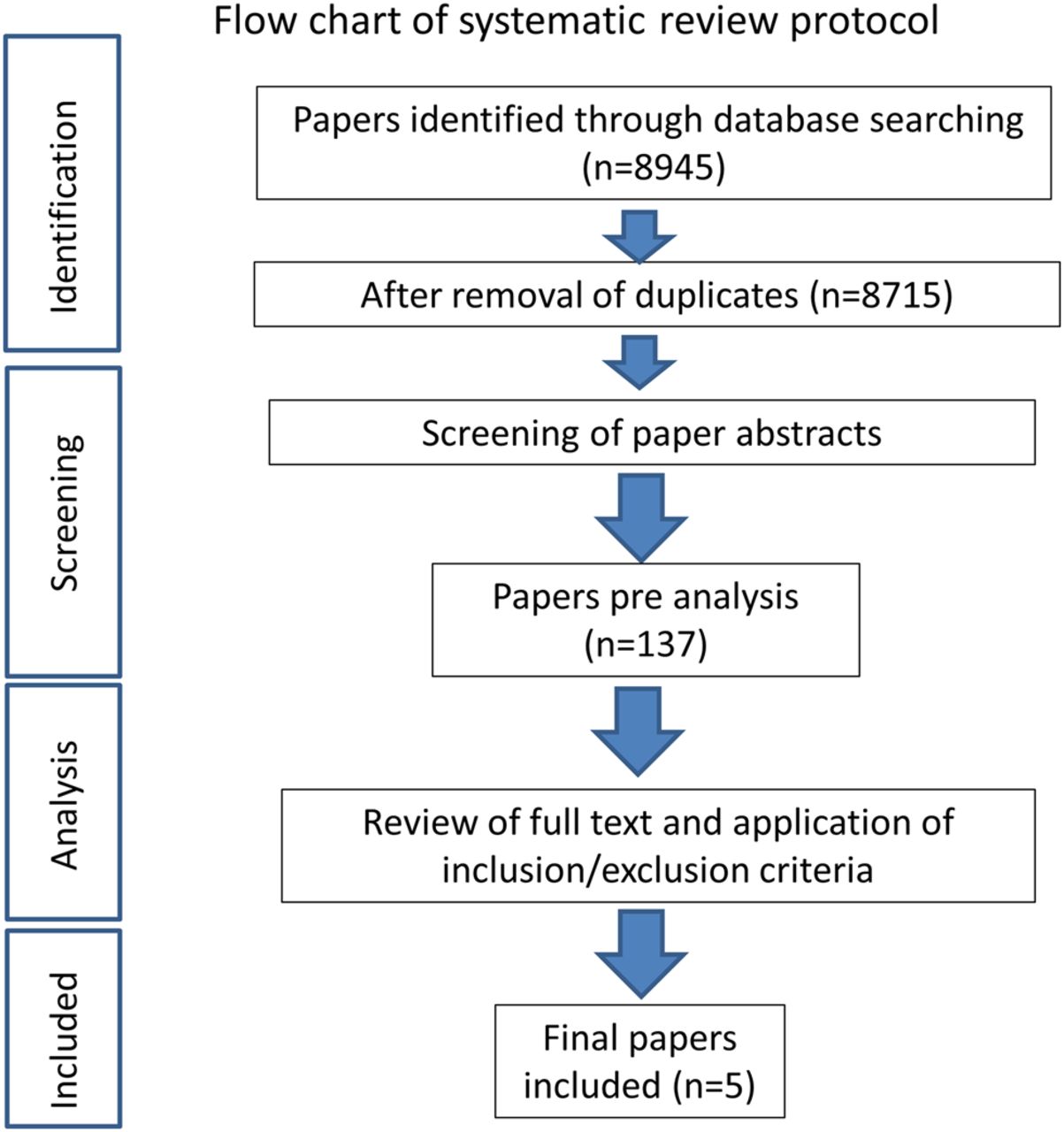
The search strategy yielded 8945 results (figure 1). After removal of duplicates and review articles, there were 8715 papers. Screening the papers revealed 130 which provisionally met the criteria based on their abstracts, and another 7 papers were provisionally included after screening the references of relevant papers by hand. Further assessment of eligibility, based on full-text papers, led to the exclusion of 132 of these 137 papers. The reasons for the exclusion of these 132 papers were as follows: not related to inflammatory cells (104), no control group (10), descriptive (6), non-specific markers (11) and methodologically biased (1). This left five papers meeting our inclusion criteria and they are summarised in table 1.
Details of included studies

{kind=link}
Flow chart of systematic review protocol.
Study characteristics
Of the five included studies, three related to the rotator cuff, one to the Achilles and one to the patellar tendon. In total, five studies analysed differences between a healthy control group and a tendinopathic group; of these studies, three13–15 carried out statistical tests for differences between control and tendinopathy, while the other two studies16 ,17 described differences without documenting the use of any statistical tests. Three studies analysed differences between different structural stages of tendinopathy; of these, one study14 carried out this analysis statistically, while the other two carried out this analysis descriptively.16 ,17 One study13 analysed differences between subgroups based on pain symptomatology.
Study methodology and assessing the risk of bias
All included studies described their study group and control groups, and clearly described the methods of tissue analysis. The results of the methodological quality assessment are detailed in the online supplementary appendix 3. The median score of the studies was 8 (range 6–10).
Of the five studies, three produced quantitative and/or semiquantitative results with a stated statistical significance of p<0.05. Of the two studies which did not state statistical significance, one used quantitative methods, and the other semiquantitative.
Studies that did not have control groups for comparison were excluded. Studies that used quantitative or semiquantitative methods in addition to a formal statistical analysis were included in the results. Studies which used quantitative or semiquantitative methods and solely a descriptive analysis (no formal statistical analysis) were included, but these results are clearly separated in the tables. This methodological assessment means that the results have not included studies with a large degree of bias, and that those with higher degrees of potential bias have been highlighted to readers. The study heterogeneity and nature of the different measures relating to the cells precluded a meaningful meta-analysis of the overall results. The summary measures were descriptive in nature, that is, increased, unchanged or decreased.
Results
There were significant differences in inflammatory cells between healthy control tendon and tendinopathic specimens (table 2).
Inflammatory cells in tendinopathic specimens versus healthy control tendon
There were higher numbers of macrophages in tendinopathic specimens versus healthy control in four studies;13 ,14 ,16 ,17 two of these used quantitative assessment,13 ,14 while two used descriptive assessment.16 ,17 Mast cells were increased in three studies14–16 in tendinopathic tissue versus healthy controls; two of these studies used quantitative assessment,14 ,15 while one used descriptive assessment.16 One study demonstrated increased numbers of T cells in tendinopathy versus control tendons,14 while one study showed no change13 and two studies did not detect significant numbers to be present in either tissue.15 ,17 One study demonstrated an increased number of leucocytes16 and one study showed no change in natural killer cell numbers in tendinopathy versus controls.13
There were significant differences between intact tendinopathic tissue and torn tendon (table 3). There were reduced numbers of T cells (one quantitative study) in torn versus intact tendinopathic tissue.14 There were reduced levels of macrophages in two studies of which one was quantitative14 and one descriptive,16 while one descriptive study showed no difference in macrophage levels.17 Mast cells were reduced in torn tendon versus intact tendinopathic tissue in two studies, one quantitative14 and one descriptive.16
Inflammatory cell differences as structural tendon failure increases
Only one study assessed the relationship between pain and inflammatory cells.13 This study assessed 32 patients over 4 years following their initial tendon biopsy, notably, the initial cohort was 50 in size and 18 patients were lost to follow-up over this period. Of the 32 patients, 20 were symptomatic and 12 asymptomatic; there were no significant differences in terms of inflammatory cell numbers at the baseline biopsy between these two groups.
Discussion
This study's findings support the hypothesis that inflammatory cells contribute to the pathogenesis of tendinopathy. There were higher levels of inflammatory cells in tendinopathic tissue versus healthy control tendons. There were reduced levels of inflammatory cells in torn tendon versus intact tendinopathic tissue. This evidence is based on a small number of studies, as very few studies have investigated inflammatory cells in tendinopathy using specific cell markers and quantitative techniques. It was notable that there was a significant diversity of opinion as to whether inflammatory cells were present in tendinopathy among a number of excluded studies. For example several studies described little or no inflammation being present despite using no specific method of identifying inflammatory cells;18–21 however, other studies described the presence of increased inflammatory cells in tendinopathy on a similar basis.22–24 This review's findings suggest the absence of acute inflammatory cells (PMNs) demonstrated previously by these descriptive basic histological studies18–21 should not be equated with the absence of chronic inflammatory change. This discrepancy in findings demonstrates neatly why the presence of inflammatory cells in tendinopathy has been a subject of such controversy, as much opinion was more based on subjective opinion than on an objective analysis of the evidence. Only one study investigated the relationship between inflammatory cells and pain, meaning that it was not possibly to draw any firm conclusions in this regard.
Definitions of ‘inflammation’ and ‘inflammatory cells’ are diverse, arguably, this represents the complexity of these concepts and it is beyond the scope of this review to enforce a consensus opinion on readers. However, it is useful to appreciate that inflammation has many facets including cell phenotype, cell receptors, cytokines and other biochemical mediators such as matrix enzymes.1 This review has summarised the evidence related to inflammatory cells, and this is supported by other work in both animals and humans, which has demonstrated specific inflammatory changes in tendinopathy. Several studies have demonstrated increased expression of inflammatory cytokines including tumour necrosis factor (TNF) α, interleukin-1β (IL-1β) and IL-6 in tendinopathy.1 ,7 ,25–27 Tendon healing has been shown to involve changes in inflammatory cytokine expression and changes in macrophage phenotype.28 ,29 Tenocytes have also been shown to possess TNFα and IL-21 signalling systems,30 ,31 notably, with IL-21 production being demonstrated to increase in response to the application of TNFα and IL-1β. The dynamic response of tendon cells and tendon to mechanical load appears related to an extremely intricate interplay between inflammatory mediators, matrix enzymes and the matrix itself;27 ,32 certainly evidence has shown that tendon's reactive response to load has an inflammatory component. The concept of the inflammatory component's importance is reinforced by the findings in animal models of tendinopathy which have demonstrated that inflammatory cells accumulate,33–35 and that inflammatory cytokines increase.25 ,36–38 This is also supported by the finding of increased levels of inflammatory cytokines in human tendinopathy.26 ,39 ,40
This study has demonstrated that there is a relative paucity of work relating to the characterisation of cell phenotype in tendon using specific markers. Our understanding of the role and functions of other cell types including macrophages, fibrocytes and fibroblast-like synoviocytes is largely based on work carried out in other chronic inflammatory diseases such as rheumatoid arthritis but has progressed substantially.41–43 However, the phenotype of the ‘tenocyte’ is still relatively unknown. There is also a relative paucity of work relating to the characterisation of human tendon-derived cells. Pauly et al44 characterised human supraspinatus and long head of biceps-derived cells, comparing them with chondrocytes and osteoblasts largely in terms of matrix gene expression. They found that tendon-derived cells expressed significantly less type II collagen and decorin compared to chondrocytes, while type I collagen expression was increased in the tendon-derived cells. Taylor et al45 analysed the gene expression of equine tendon-derived cells, finding that COL1A2 was highly expressed in vitro, and that scleraxis expression is reduced in culture.
In this context, it is vital to better understand the cell phenotype in normal and disease tendon, and whether specific inflammatory changes are linked to disease stage or symptom progression. Questions could be answered using techniques such as flow cytometry and cell sorting, which would then enable the development of an understanding as to which cell subpopulations are expressing which particular proteins and genes. It may be hypothesised that a specific subpopulation of tendon-derived cells are more inflammatory in terms of cell marker expression, and that this group of cells is pivotal in propagating the inflammatory response in tendinopathy by secreting proinflammatory cytokines. For example, it has been shown that mast cells exert proinflammatory effects on human tendon-derived cells in vitro.46 Macrophage depletion has been shown to increase the ultimate tensile strength of healing mice Achilles tendons.47 Changes in macrophage phenotype and epithelial-to-mesenchymal transition genes have been noted following Achilles tenotomy and during repair.29 The development of a better understanding of the role of specific cell subpopulations in pathogenesis of tendinopathy and during tendon healing is vital to identify potential therapeutic targets and develop more effective future treatments for patients. Studies of equine tendinopathy suggest that chronic inflammation may develop due to inadequate resolution of inflammation.48 ,49 Recent work relating to IL-33 appears to show much promise in terms of providing a novel therapy.50 Certainly, further work is needed in humans before specific inflammatory targets can be actively pursued in clinical trials; it is vital that a better understanding of the role of the chronic inflammatory process in tendinopathy is first demonstrated.
The findings of this review are consistent with chronic inflammation being present in tendinopathy; it is worth reiterating that acute inflammation, as reflected by the presence of PMNs, has not been demonstrated in tendinopathy. Much in the same way that osteoarthritis was once seen as a non-inflammatory disease but is now recognised to have a significant inflammatory component,51 our understanding of tendinopathy appears to be moving towards the incorporation of an important inflammatory component.52
Limitations of this review
The results and generalisable meaning of this review are both limited by the quality and heterogeneity of the included studies. There was significant study heterogeneity in terms of the tendon studied, the type of control tendon used, the stage of the tendinopathic tissue analysed, mode of tissue analysis, mode of inflammatory cell quantification and the cell markers used. It is important to note that the tendon sampling method may contribute to the differences observed, and the amount of loose connective tissue in specimens may vary between healthy controls and the tendinopathic. The exclusion of studies which did not use specific cell markers was a decision taken in order to exclude studies which have relied on the more subjective interpretation of tendon histology. We appreciate this cut-off is somewhat arbitrary, but the decision about where this line should be drawn was agreed on by all authors; it was felt that summarising the results of the potentially highly biased descriptive basic histological studies would not add significant value to this review. The degree to which the results of the studies were descriptive, semiquantitative or quantitative was highly variable. As a result, it has been made clear when results have not been shown to be statistically significant (tables 2 and 3). The variable blinding of the observers undertaking the semiquantitative tissue grading does increase the risk of study bias towards positive findings.
Only one study measured the proportion of cells that were inflammatory cells,14 while the remaining studies did not normalise the measure of inflammatory cells to the overall cell number. Given that cellularity increases in tendinopathy, it is likely that not normalising for cell number will increase the chance of positive findings. However, this is not to say that these positive findings are not of meaning, it would simply be interesting to see the results for the normalised inflammatory counts and if the positive results remained. The review has also highlighted that studies are not always as unbiased and objective as they could be in terms of tissue sampling, image analysis and cell quantification. It is important that future studies note these potential pitfalls. One way of enhancing our understanding of disease pathogenesis is to obtain better control tissue. In order to better understand the resolution of pain, a fruitful future avenue may be that of obtaining tissue from patients with resolved tendinopathy pain, and comparing this with patients with persistent pain.
Conclusions
The existing evidence supports the hypothesis that there are increased levels of specific inflammatory cells in tendinopathy which is consistent with a presence of a chronic inflammatory process. The lack of high-quality quantitative studies in this area demonstrates a clear need for future research to better understand the role of inflammation in tendinopathy which may lead to novel therapeutics.
What are the new findings?
Very few studies have assessed inflammatory cells in tendinopathy using specific cell markers and quantitative techniques.
A small number of studies suggest that inflammatory cells are increased in tendinopathy versus healthy control tendon.
There is a clear need for future research to investigate the role of inflammation in tendinopathy, particularly in relation to pain symptoms.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online appendix 3
Footnotes
Contributors BJFD and PG contributed to study conception and design, data collection and analysis, drafting of the article and critical revision of the article. SGD and AC contributed to study conception and design, critical revision of the article.
Funding The authors of this work are funded by the Musculoskeletal Biomedical Research Unit of the National Institute for Health Research (BD, SGD and AC), Arthritis Research UK (SGD), the Jean Shanks Foundation (BD) and Orthopaedic Research UK (BD).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.