Article Text

Abstract
The aim was to assess the quality and strength of evidence for the health benefits of specific sport disciplines. Electronic search yielded 2194 records and the selection resulted in 69 eligible studies (47 cross-sectional, 9 cohort, 13 intervention studies). 105 comparisons between participation and non-participation groups in 26 different sport disciplines were reported. Moderately strong evidence showed that both running and football improve aerobic fitness and cardiovascular function at rest, and football reduces adiposity. Conditional evidence showed that running benefits metabolic fitness, adiposity and postural balance, and football improves metabolic fitness, muscular performance, postural balance, and cardiac function. Evidence for health benefits of other sport disciplines was either inconclusive or tenuous. The evidence base for the health benefits of specific sports disciplines is generally compromised by weak study design and quality. Future research should address the health effects of different sport disciplines using rigorous research designs.
- Health promotion
- Sports analysis in different types of sports
- Aerobic fitness
- Intervention effectiveness
- Evidence based review
Statistics from Altmetric.com
- Health promotion
- Sports analysis in different types of sports
- Aerobic fitness
- Intervention effectiveness
- Evidence based review
Introduction
The goal of increasing participation in sports remains a common aim of national governments and often sport is seen as a mechanism to guide young people along a pathway of an active lifestyle. This notion of sport participation contributing to a physically active lifestyle is politically popular but not necessarily supported by national physical activity surveys, as sports participation appears to consistently decline with age.1 Regular participation in sports brings well-documented health benefits,2–4 but the evidence of the health impact of specific sport disciplines largely consists of indirect inferences from physiological and biomedical characteristics of different sports.5
Researching the health impact of sports has tended to concentrate on studying the mortality and morbidity of ex-athletes, but such studies are limited by selection bias and confounding. Earlier studies on ex-athletes have suggested that participants of endurance type sports have reduced risk for obesity, type 2 diabetes, coronary heart disease and premature mortality, but they also have increased risk for osteoarthritis in team games with high knee injury risk.6 These studies usually face the problem that the comparisons have been made with general populations, including individuals with chronic diseases and disabilities at young age.6 Therefore, none of these types of athlete studies can completely control for the strong selection bias as highly fit individuals are selected to be participants in sports. Thus cause-and-effect evaluation is impossible.
Recently a review identified 12 reviews on the health benefits of participation in specific sport disciplines.5 Fewer than 20 specific sports were covered in these reviews and the majority of studies were based on cross-sectional data. It was concluded that in the published literature there is an obvious shortage of higher quality evidence on the health benefits of specific sport disciplines.
In order for the sport movement to justifiably contribute to public health there is a need to know the scientific evidence of the beneficial and adverse health effects specific to different sport disciplines. We feel it is important to place sport within the context of physical activity and exercise. ‘Physical activity’ is “any bodily movement produced by the contraction of skeletal muscle that increases energy expenditure above a basal level.”7 ‘Exercise’ features are “planned, structured, and repetitive and purposive in the sense that the improvement or maintenance of one or more components of physical fitness is the objective.”7 ‘Sport’ is a “subset of exercise that can be undertaken individually or as a part of a team whereby participants adhere to a common set of rules or expectations, and a defined goal exists.”8 For the purpose of this review we considered ‘sport discipline’ as a specific type of sport in which the activity itself consists of uniform movement patterns characteristic of that sport.
As organised sport movement encourages participation in a broad range of different sport disciplines, evidence is needed on the health and functional effects of specific sport disciplines. The aim of our review was to assess the quality and strength of the evidence for the health benefits of specific sport disciplines. This will be the first review of the evidence assessing the health benefits of specific sports.
Methods
Data search
We used criteria for PROSPERO (International database of prospectively registered systematic reviews in health and social care) to provide the structure for our review. We identified three possible sources of potential studies: (1) electronic literature databases and websites, (2) snowballing from reference lists of review and retrieved articles and (3) from the authors’ archives.
We conducted a systematic search of electronic databases including SPORTDiscus, SpoLit, Physical Education Index, Scopus, PubMed and Web of Science from 2003 until the end of April 2013. Tailored search terms were constructed for each database after several test searches and included combinations of the following key mesh terms (sports*) AND (health* OR Gesundheit*, fitness*). Search languages were English, German and Finnish. The full search strategy, identification of publications and data extraction details are described in PROSPERO register with the registration number CRD42013006927 (http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42013006927#.VA3kFPmwL3s).
Briefly, in the first stage of the search, titles and abstracts of identified articles were checked for relevance. In the second stage, full-text articles were retrieved and considered for inclusion. In the final stage, the reference lists of retrieved full-text articles were searched and additional articles known to the authors were assessed for possible inclusion.
Criteria for study inclusion/exclusion
Studies were considered to be eligible for inclusion according to the following criteria: (1) participants: healthy males and females of all ages (we excluded studies where the participants were disabled or chronically ill patient groups), (2) type of studies: original observational studies (cross-sectional and cohort studies) and intervention studies (randomised controlled trials (RCT) and quasi-experimental studies) that were published in peer-reviewed journals, (3) study must include participation in specific sport disciplines, (4) study design must have a non-participation comparison group, (5) outcome variables must be health related in terms of mortality, morbidity or disease risk factors, and/or function related in terms of cardiorespiratory, metabolic or musculoskeletal fitness (we excluded studies in which the outcome variables were injuries or other acute health problems) and (6) studies must be published either in English, German or Finnish languages from January 2003 to April 2013.
The details of the selection process are described in the PROSPERO register as indicated above. In short, the consistency of applying the selection criteria on study titles and abstracts was first checked by two authors (PO and SK) for every 10th record. The inclusion/exclusion of potential full papers was first conducted by one author (PO) and then confirmed by two others (ST and SK).
The cross-sectional studies were considered to provide only descriptive evidence. They were included only in the general description of the identified evidence. Further analysis of the cross-sectional studies will be done separately and reported elsewhere.
Data extraction
For prospective cohort studies the extracted data consisted of: the number, gender and age of the participants in the cohort; duration of follow-up; type of sport discipline(s) included in the analyses with definition of the used comparison categories; name and unit of each outcome variable; used statistic and statistical adjustments; and statistical significance(s) of the pre–post comparisons.
From the intervention studies the following data were extracted: specific type of study design; number, gender and age of participants in each comparison group; type, length, intensity, frequency and bout duration in each intervention group; name and unit of each outcome variable; within and between group pre–post per cent changes and their statistical significance.
Assessment of the quality of the studies
The risk of bias of the prospective cohort studies was assessed by the Newcastle-Ottawa Quality Assessment Scale (NOS) for cohort studies.9 This scale rates the quality of three domains of a study: (1) selection, (2) comparability and (3) outcome. In the selection domain four characteristics are rated: representativeness of the exposed cohort, selection of the non-exposed cohort, ascertainment of exposure and demonstration that outcome of interest was not present at the start of the study. In the comparability domain, the level of controlling the confounding factors is assessed. The outcome domain is rated for the type of the assessment, the length of the follow-up and adequacy of the follow-up. Each of the selection and outcome characteristic is given one star and the comparability domain two stars for high rating, resulting in a total of zero to nine stars for overall quality.
The quality of the intervention studies was assessed by the Effective Public Health Practice Project Quality Assessment Tool (EPHPP).10 The tool assesses six components of a study: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data collection methods and (6) withdrawals and drop-outs. Each component is rated as strong, moderate or weak according to the set criteria. The global rating is strong, if there are no weak component ratings; moderate, if there is one weak component rating; and weak, if there are two or more weak component ratings.
Full description of the quality analyses is provided in the PROSPERO register as indicated above. In short, the assessment of all included studies was first done by one author (PO), repeated half and half by two authors (ST and CF for prospective studies, and ST and AH for intervention studies), and followed by consensus decision among the three.
Summary measures
For the prospective cohort studies, we used statistically significant pre–post exposure/outcome associations (p<0.05) between the sport participation group(s) and the non-participation group as the summary measures. Among the intervention studies, statistically significant (p<0.05) within-group pre-post changes (%), and between-group pre-post differences were used as the measure of intervention effect. The reported outcome variables were grouped, for the purpose of coherence, into 13 commonly used health/fitness domains as follows: mortality, aerobic fitness, cardiovascular function at rest, cardiac adaptation, adiposity, metabolic fitness, blood lipids, bone traits, running performance, muscular performance, postural balance, other.
Meta-analyses
We completed a narrative summary of the study results and when there was sufficient data (≥5 studies) we completed a formal meta-analysis of the included studies using the RevMan V.5.0 software.11 For each study with continuous outcomes, we expressed the effect size using the standardised mean difference between the postintervention values of the randomised groups. We analysed the studies using the mean and SD and visualised the results using forest plots. We quantified and evaluated the heterogeneity to determine whether the observed variation in the study results was compatible with the variation expected by chance alone.12 Heterogeneity was assessed through examination of the forest plots and quantified using I2 statistic.
Strength of the evidence
To assess the strength of the evidence, a rating system based on previously defined best evidence synthesis was used.13 This system rates the evidence as follows.
Strong evidence: (1) at least two RCT of high quality, (2) one RCT of high quality and at least two RCTs of medium quality. Effects must be consistent for both cases.
Moderate evidence: (1) one RCT of medium quality and at least one RCT of low quality or (2) one RCT of medium quality and at least one controlled trial (CT) of high quality or (3) at least three CTs of high quality or (4) one CT of high quality and at least three CTs of medium quality. Effects must be consistent for all cases.
Limited evidence: (1) more than one RCT of low quality or (2) one CT of medium quality and two CTs of low quality or (3) two CTs of low quality and at least two before–after, cohort or longitudinal studies. Effects must be consistent for all cases.
Inconclusive evidence: (1) only one study or (2) multiple before–after, cohort or longitudinal studies or contradictory effects.
No evidence: more than one study with consistent non-significant effects.
Results
Study selection
The data search yielded 2194 records (figure 1). After removing duplicates, the remaining records were assessed under the inclusion/exclusion criteria resulting in 50 unique records, for which full papers were sought. After the inclusion of 41 full papers from other sources, 91 papers remained for potential inclusion. Subsequently, 22 papers were excluded for not meeting the inclusion criteria. Thus the resulting search outcome included 69 eligible studies, of which 47 were cross-sectional, 9 prospective cohort and 13 intervention studies. The cross-sectional studies were excluded and retained for separate analysis.
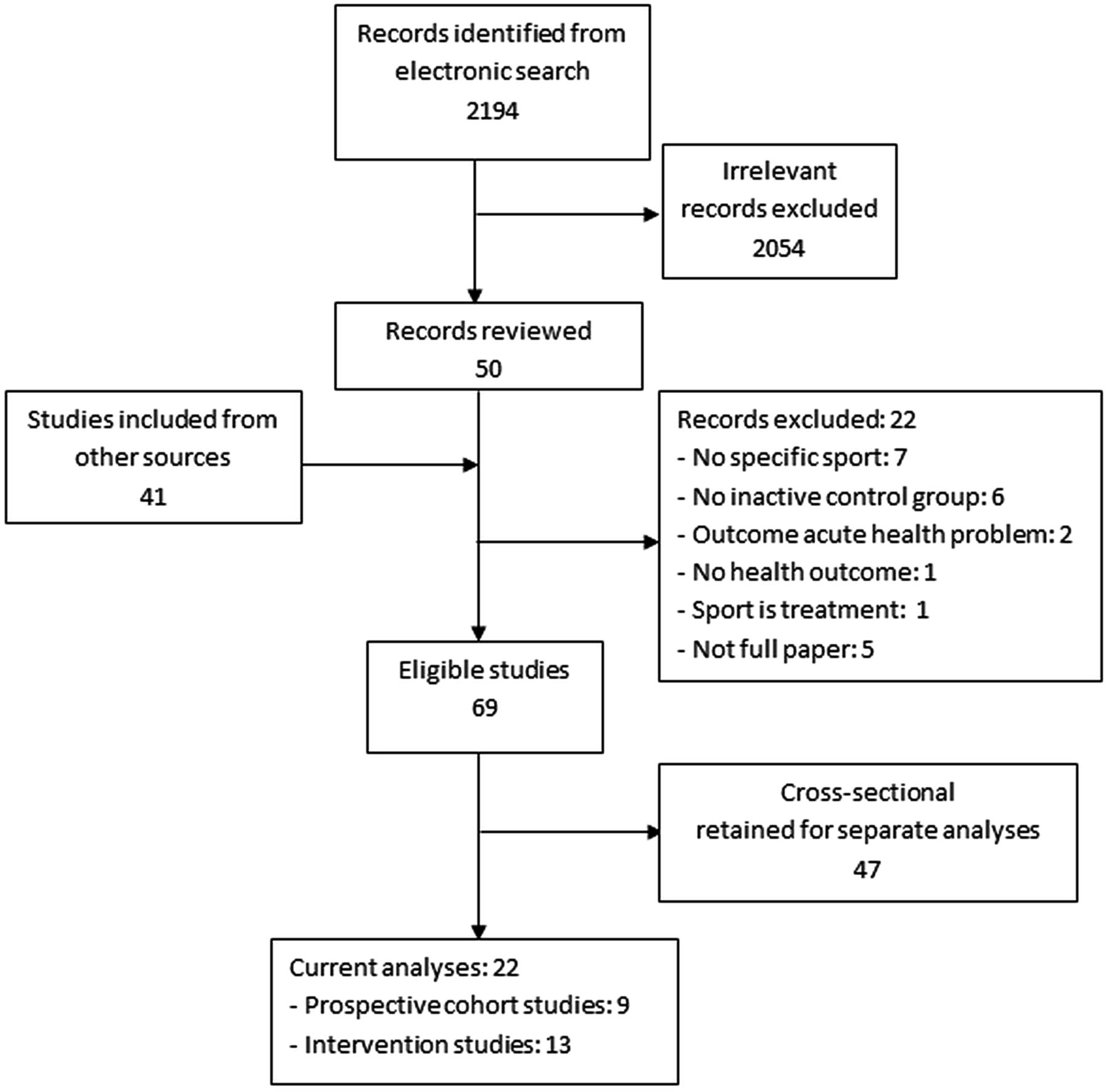
Flow chart of the data search.
The participants in the prospective cohort and intervention studies were all adults between the ages of 19–90 years, healthy and relatively inactive.
Sport discipline specific comparisons
Altogether 105 comparisons between participation and non-participation groups were reported involving 26 different sport disciplines (table 1). Sixty-eight of the comparisons came from cross-sectional studies, 15 from prospective cohort studies and 21 from intervention studies. Running and football had the most comparisons (22 and 18, respectively), most of these from prospective cohort and intervention studies. Gymnastics had 17 comparisons and all came from cross-sectional studies. Cycling had nine; swimming eight; rowing and climbing three, tennis, squash, volleyball and hurdling two and all other disciplines only one comparison.
Number of comparisons by sport discipline and study design
Study characteristics and synthesis of results
Prospective cohort studies
Nine prospective cohort studies met the inclusion criteria, four dealt with jogging/running, four with cycling, three with swimming and one each with tennis, rowing, racquetball and golf (online supplementary table S1). Jogging/running was shown to be associated with reduced total cardiovascular, cancer, neurological and infectious mortality and moderate disability among men and women.14 The decrease in mortality was shown for male and female runners, who were members of a nationwide US running club and who averaged more than 1 hour of running each week. Jogging/running was also shown to reduce weight gain among women15 ,16 and men.15 One study showed no association between jogging/running and the risk of cardiovascular disease (CVD).17
To be consistent with the definition of sport discipline we used, cycling was limited to recreational cycling (we excluded cycling for transport or other utility purposes). These studies examined associations with changes in waist circumference,18 CVD incidence,17 incidence of colon cancer,19 and all-cause, cardiovascular and cancer mortality.20 No statistically significant associations were found.
Among the three studies on swimming, no association was shown with the risk of CVDs17 and weight change,15 but there was a significantly reduced all-cause mortality in one study.21
Four other sport disciplines were included in one cohort study each. Regular golf practice as a member of a golf club was shown to be associated with reduced all-cause mortality22 and tennis practice with decreased risk of CVDs.17 Participation in rowing or racquetball showed no association with CVD risk.17
According to the NOS tool, the overall quality was high for one study, moderate for seven studies and low for one study (table 2).
Quality assessment of the prospective cohort studies according to the Newcastle-Ottawa Scale*9
Intervention studies
Thirteen intervention studies met the inclusion/exclusion criteria (online supplementary table S2). According to the EPHPP tool, five of these were RCTs and eight controlled clinical trials with randomised intervention groups (randomised into different sport interventions) and non-randomised but matched control groups. Nine of the intervention studies came from the same laboratory (Department of Exercise and Sport Sciences, University of Copenhagen, Denmark). Of these, two studies among women and two studies among men reported results from the same intervention experiment.
The intervention studies reported effects of four different sport disciplines: recreational small-field football (10 studies), running (9 studies), swimming (1 study) and equitation (1 study).
Football was shown to consistently improve aerobic fitness,23–27 measures of cardiovascular function at rest,23 ,25 ,26 ,28 ,29 metabolic fitness,24 ,26 ,28 running performance30 ,26 ,28 and reduced adiposity.23–27 ,29 Improved cardiac adaptation,31 ,26 blood lipids29 ,27 and muscular performance32 ,29 were indicated in two studies each, and increased bone mineral density and improved postural balance each in 1 study.32
Running was shown to improve aerobic fitness in four studies,23 ,25 ,26 ,28 cardiovascular function at rest in three studies,24–26 and running performance in three studies.30 ,23 ,26 Some, but fewer, evidence was shown for improvement in metabolic fitness,24 ,25 cardiac adaptation,24 muscular performance32 and postural balance.32
Another RCT33 showed that postural control, as assessed by centre of pressure sway and Flamingo test, improved in response to 12 weeks of soccer and running training among men.
There was only one study on swimming and one on equitation. Body mass index decreased slightly but significantly in the swimming group, and muscle strength in trunk flexion and knee extension decreased significantly in swimming and control groups, but less in the swimming group.34 Equitation training showed significant increase in muscle strength and decrease in fatigue index.35
According to the EPHPP tool (table 3), all 13 studies used either RCT design or controlled clinical trial design, and were rated strong for the design. The ‘representativeness’ component, or selection bias, was rated weak for all studies. The global rating of the intervention studies yielded no ‘strong’, six ‘moderate’ and seven ‘weak’ scores.
Quality assessment of the intervention studies according to the EPHPP tool*
Meta-analysis
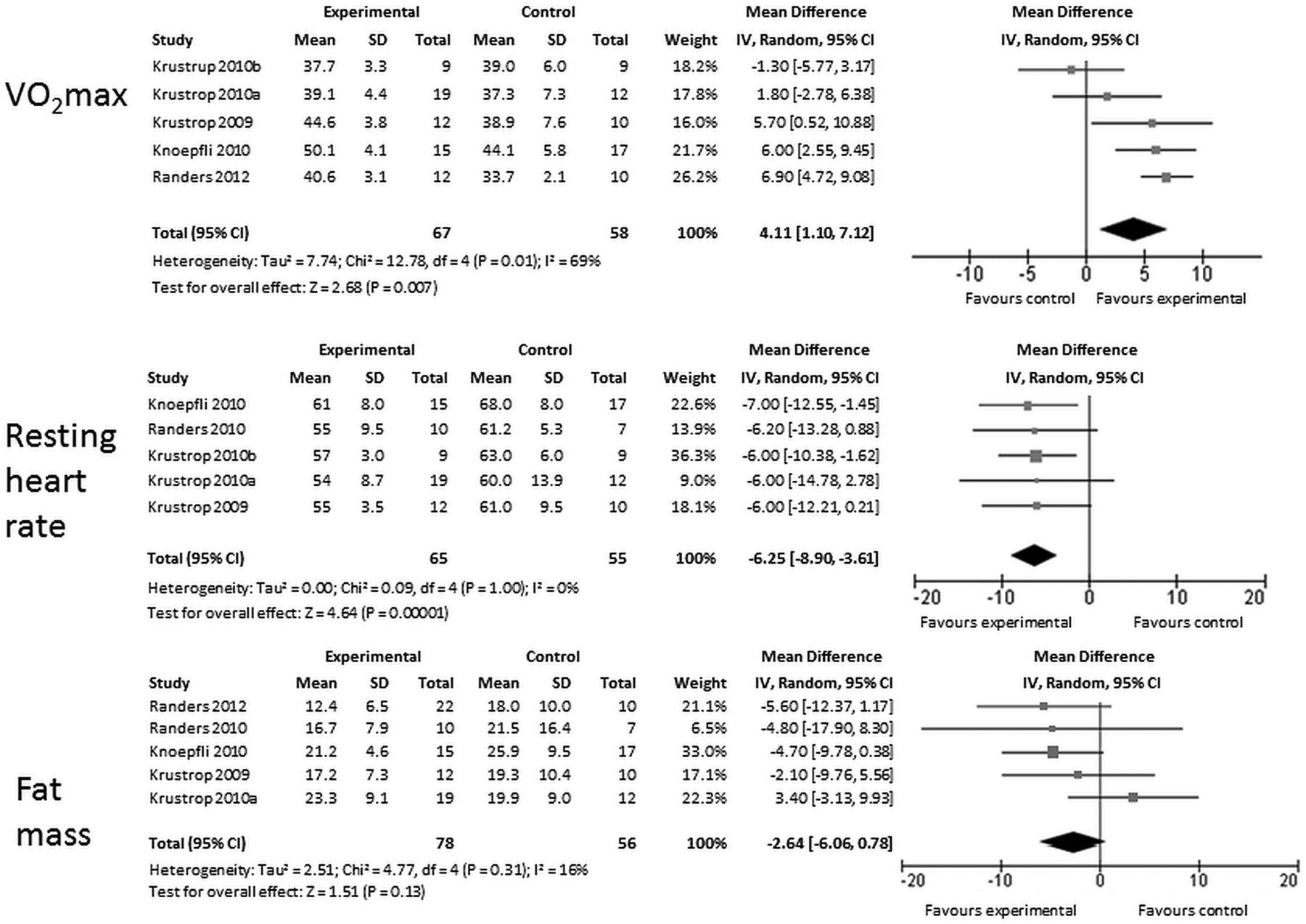
There was sufficient data for the meta-analysis of the effect of football on three outcomes: VO2max, fat mass and resting heart rate (figure 2). For any other sport discipline, the data was insufficient for meta-analysis.
{kind=link}
{kind=link}
Meta-analysis of the effects of recreational football on aerobic fitness (VO2 max mL/kg/min), resting heart rate (bpm) and fat mass (kg).
Pooled estimate of effect for football showed a statistically significant overall increase of 4.11 mL/kg/min (CI 1.10 to 7.12) in VO2max and a decrease of 6.25 bpm (CI −8.90 to −3.61) in resting heart rate. The pooled effect for VO2max was positive and moderate but with significant heterogeneity (I2=69%). Fat mass decreased by 2.64 kg (CI −6.06 to 0.78) but the change was borderline statistically significant. There was no evidence of heterogeneity in pooled effects for resting heart rate (I2=0%) or fat mass (I2=16%). We found no evidence of publication bias.
Discussion
Strength of the evidence on health benefits of sport disciplines
Our review identified the associations with or effects on health and functional outcomes for 26 different sport disciplines. This is the first time this evidence has been collated and compared in a systematic review. The most commonly studied sport disciplines were running (22 comparisons participation vs no participation), football (18), gymnastics (17), recreational cycling (9) and swimming (8).
According to the used scale of the strength of the evidence,13 the health benefits of these disciplines can be summarised as follows:
For running, moderate evidence shows improvements in aerobic fitness, cardiovascular function at rest and running performance; all these changes are shown for women and men. Limited evidence for improvements was shown in metabolic fitness and adiposity among both genders, and in postural balance among men. Inconclusive evidence was found in cardiac adaptation, muscular strength and in all-cause and disease-specific mortality.
Moderate evidence shows that recreational football improves aerobic fitness, cardiovascular function at rest and adiposity in both genders. These observations are corroborated and quantified by the performed meta-analyses: pooled data shows 11% increase in aerobic power, 10% decrease in resting heart rate and 13% decrease (borderline significant) in fat mass. These changes were accrued with the football dose of 12–16 weeks duration, about 80% HRmax intensity, about two sessions per week frequency and 1 hour bout duration. The degrees of improvements can be clinically significant based on recent findings showing that those who have 10 METs or greater exercise capacity have an extremely low risk of death from CVD36 and those who have low resting heart rate have a lower risk of CVD and all-cause mortality.37 Limited evidence shows improvements in metabolic fitness, cardiac adaptation and muscular performance, in both genders, and in blood lipids and postural balance among men. Inconclusive evidence is shown for benefits in bone mineral density.
For swimming, we found some evidence for reduced total and CVD mortality and adiposity, but it was inconclusive. Evidence for improved muscle strength in equitation was also inconclusive. There was no evidence to show that recreational cycling has beneficial effects on total, cardiovascular and cancer mortality, CVD incidence or adiposity.
All these findings pertain to ostensibly healthy and relatively inactive middle-aged persons.
Owing to the small number of studies reporting the effects of other sport disciplines, conclusions about the health benefits cannot be drawn.
One new study eligible for our review has been published after the closure of the data search. Mendham et al38 studied rugby and ergometry cycling and showed that regular rugby training for 8 weeks improved submaximal power output, decreased fat mass and increased fat-free mass in middle-aged men. This is the first intervention study showing effects of recreational rugby.
After the submission of this review, a special issue of Scandinavian Journal of Medicine & Science in Sports39 has published 16 original articles on the health and functional effects of recreational football. Reported results show that football improves the structure and function of the heart, lowers blood pressure, reduces blood lipids and body fat, and improves functional capacity.40 These observations strengthen the evidence on the benefits of football found in the present review.
Risk of sports injuries
From the public health perspective, the health benefits due to participation in different sport disciplines have to be balanced with the possible health risks involved. Sports injuries are especially of potential concern. The reviewed intervention studies provide some relevant information. No injuries were reported in swimming33 and in equitation34 interventions among women. Of the four interventions with football and running training among women, two reported no training-related injuries.31 ,26 Both of the other studies in women25 ,32 reported 4 injuries among 78 women, for both football and running. The studies among men reported 2/15,23 1/13,24 0/1029 and 1/2727 football-related injuries, and 0/15,23 2/1228 and 2/941 running-related injuries. These injury rates add up to approximately 1 injury per 700 h of football training and 500 h of running training. In high-intensity interval running relatively more training-related injuries (5/8) were reported although three of these were transient in nature.41
The present information, limited to relatively small short-term intervention studies, suggests that while many types of sport disciplines may induce significant cardiometabolic and musculoskeletal benefits, football and running training particularly among previously untrained women and men may expose them to increased risk of injuries, albeit mostly minor ones. Thus, when implementing sport disciplines as health-enhancing physical activities, the known effective injury prevention measures42 should be built in as an integral part of the intervention programmes. The reviewed trials are too small and too short in duration to evaluate the possible occurrence of uncommon severe complications and longer trials are needed to assess the sustainability of benefits and participation over time.
Methodological considerations
Overall the evidence base of the health benefits of different sport disciplines is diverse, comprising of many relatively simple cross-sectional studies addressing a mixed variety of single sport disciplines and fewer prospective cohort and intervention studies. The latter two types of published studies focus mainly on running and football. According to the NOS tool,9 the quality of eight of the nine prospective cohort studies were rated overall as at least moderate. Particularly strong aspects were the selection of non-exposed cohort, outcome not present at onset, control of potential confounders and the duration of the follow-up. A weaker aspect was the ascertainment of exposure due to the use of physical activity self-report.
According to the EPHPP tool,10 the ‘representativeness’ component, or selection bias, was rated weak for all intervention studies, because in these types of exercise interventions the participants are typically highly selected due to the multistep screening procedure including a clinical health assessment for the safety of the exercise stress test and the training. This limitation may reduce the potential reach of sports programmes to less active groups. ‘Blinding’ was also a weak component in these studies due to the fact that in exercise interventions of this type, it is difficult to blind both the participants and the assessors; the exercise intervention cannot be blinded from the participants and the assessors are typically involved not only in the measurements but also in providing the interventions.
Sport for public health?
Khan et al8 states that sport is one sector that can improve the health of nations through increased physical activity. The sport for all movement has increasingly used the improvement of health as its social justification.43 The potential of different sport disciplines to promote public health depends, on one hand, on the prevalence of a given sport and on the other hand, on health benefits of that sport. Apart from the study-specific synthesis of the data, it is clear from the meta-analysis that significant improvements in cardiovascular function can be achieved by participation in the twice weekly football sessions. The potential public health impact of regular twice weekly participation would ensure that all participants achieve existing physical activity guidelines. The challenge is to see if such programmes can attract and retain participants to enjoy the benefits of regular participation.
In order to promote sport for all effectively as an evidence-based physical activity for public health, the focus and type of research needs to be appraised according to the largest possible population impact. Especially there is a need for prospective cohort studies and intervention trials on those sport disciplines that are prevalent among populations. We suggest that any assessment of national surveys of physical activity should include discipline specific assessments of sport, for example, the UK's Health Survey for England.1
Conclusions
The present review indicates that there is considerable amount of published evidence on the health benefits of different sport disciplines, but the information is fragmentary. Most identified studies have used cross-sectional design addressing a large number of single sport disciplines but do not demonstrate the cause and effect nature of the found relationships. More substantial evidence was found from prospective cohort and interventions studies focusing particularly on recreational football and running. According to the synthesis of the data, there is conditional evidence to show that recreational football can benefit aerobic fitness, cardiovascular function, metabolic fitness, adiposity, cardiac adaptation, muscular performance and postural balance. Such physiological effects can be conducive for reduced risk of cardiovascular and all-cause mortality. For running, similar evidence shows benefits in aerobic fitness, cardiovascular function, running performance, metabolic fitness, adiposity and postural balance. Most of these benefits apply to adult women and men. The evidence found for health benefits of other sport disciplines was either inconclusive or tenuous.
Our review shows evidence (up to April 2013) for the potential public health impact of different sport disciplines, but the evidence base is generally compromised by weak study design and quality. The exception is for running and football which provide the strongest evidence for positive health benefits. We call on the research community to tackle this deficiency by examining the impacts of the most popular sports, based on participation levels, using rigorous research designs.
What are the new findings?
-
Sport as a general domain of physical activity is often claimed to benefit health. Published evidence on the health benefits of specific sport disciplines is scarce and impaired by weak study designs. Rigorous evidence on the health benefits of different sport disciplines would help support the sport movement to take a stronger role in promoting participation in sports for public health.
-
We found evidence on the sport–health relationship for 26 different sport disciplines. Most evidence came from cross-sectional studies, and less from prospective cohort and intervention studies.
-
Studies on only five sport disciplines (running, football, cycling, gymnastics and swimming) provided more than three comparisons between participant and non-participant groups.
-
Best evidence was found for recreational football and running. These can especially benefit cardiovascular and metabolic fitness.
-
There was some, but inconclusive, evidence for health benefits of recreational cycling and swimming. No solid evidence showed health benefits for any other sport discipline.
Acknowledgments
The authors thank graduate student Tero Pasanen for his help in extracting the cross-sectional data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
-
Contributors PO, ST, SK and PKo contributed to conception. PO, ST and SK contributed to design. PO, ST, AH, PKe and CF contributed to analysis. PO, ST, UMK, PKe and CF contributed to interpretation. PO, PKe and CF drafted the manuscript. All authors revised the manuscript and gave final approval.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.