Article Text

Abstract
Background There have been few in-depth studies of upper limb injury epidemiology in rugby union football, despite reports that they accounted for between 14% and 28% of all rugby injuries.
Objective To report on upper limb injury incidence, injury severity and to identify the risk factors associated with upper limb injuries, for example, level of play, season (years) and playing position.
Design Prospective cohort study across five rugby seasons from 2004 to 2008.
Setting Formal rugby competitions—suburban, provincial and international.
Participants 1475 adult male rugby players in Colts, Grade and Elite competitions.
Main outcome measurements An upper limb injury resulting in a missed game and its characteristics.
Results A total of 61 598 athletic exposures (AE) and 606 upper limb injuries were recorded. About 66% of the injuries were to the shoulder. The overall upper limb injury incidence rate (IIR) was 9.84 injuries/1000 AE (95% CI 9.06 to 10.62). Statistically significant associations were found between upper limb injuries and level of play; and between shoulder injuries and playing position (p<0.05). No association was found between upper limb and shoulder injuries and study year. The overall upper limb IIR decreased as the level of play increased; 10.74 upper limb injuries/1000 AE (95% CI 9.93 to 11.56) in Colts to 6.07 upper limb injuries/1000 AE (95% CI 5.46 to 6.69) in Elite.
Conclusions The upper limb IIR decreased as the level of play increased indicating that age, level of skill and playing experience may be risk factors for upper limb injury.
- Injury Prevention
- Sporting injuries
- Shoulder injuries
- Rugby
Statistics from Altmetric.com
Introduction
Upper limb injuries, incorporating the shoulder to fingers, have been reported to account for between 14% and 28% of all rugby injuries and to be more severe and associated with the longest absence from competition compared with other injuries.1–9 To date, there has been little research with a focus on upper limb injury incidence and associated risk factors in rugby union football (‘rugby’).
The upper limb injury incidence rate (IIR) in rugby has been reported to be in the range 1.50–7.90 injuries/1000 player participation hours (pph) in amateur, youth and professional players.10 ,11 In terms of the nature of upper limb injury, 55–71% were sprain/strain and 4–26% were dislocation or fractures.12 ,13 Hand/finger fractures and shoulder dislocations accounted for 80% of the most severe upper limb injuries.5 Studies have reported that a substantial portion of all upper limb injuries (45–75%) are shoulder injuries; where the shoulder complex included the acromioclavicular joint (ACJ), the glenohumeral joint (GHJ), the sternoclavicular joint (SCJ), clavicle, deltoids, biceps tendons and rotator cuff.5 ,9 ,14 Shoulder injuries accounted for 9–17% of all injuries. 5 ,7–9 ,15 ,16 The IIR to the shoulder was reported to be in the range 1–4.9 injuries/1000 pph in non-professionals and 8.9 injuries/1000 pph in professional players.10 ,11 ,17 ,18 During the 2003 and 2007 Rugby Union World Cups (RWC), 8% and 11%, respectively, of all injuries were to the shoulder.6 ,8 In the RWC the most common types of shoulder injury were sprain and strain, while dislocation and fracture resulted in the greatest absence from play.
Age group and level of play have been identified as general injury risk factors in rugby.6 ,7 ,19 ,20 The IIR in rugby has been reported to increase with age and competition level.7 ,10 ,12 ,13 ,16 ,20 ,21 Haseler et al11 reported that 33% of all injuries in community youth rugby were to the upper limb with 62% of those being shoulder injuries. Brooks et al13 reported in professional club rugby that the forwards had a non-significant higher upper limb injury incidence and average severity compared to backs; 19% and 14% (injury incidence), respectively, and 21 and 7 days (average severity), respectively.
Although upper limb injuries, in particular shoulder injuries, are well understood medically, the aetiology and risk factors in rugby union football are not. The main aims of this study were to measure upper limb injury incidence and severity, and identify risk factors associated with upper limb injuries, for example levels of play, game event, season (years) and playing position.
Methods
Study design and participants
The Rugby Union Injury Surveillance Study (RUISS) was a prospective cohort study of rugby players from a cross-section of competition levels. This paper reports on the cohorts: Elite—Australian teams in the Super 12/14 competition and the Australian Wallabies (potentially four or five teams); Grade—12 rugby clubs from the NSW Rugby Union Sydney Grade Competition and Colts—12 rugby clubs in the NSW Rugby Union Premiership Colts under 20-year-old competition. Each season clubs and teams were first approached regarding their support for the study, after which players from the supporting clubs/teams were recruited. The number of teams approached each year depended on the available budget, competition structure and the level of support available from each team. There were either four or five elite teams, three team divisions considered in Grade clubs and two team divisions in Colts clubs. The study was approved by the UNSW Human Research Ethics Committee and all participants gave written informed consent. All participants were male. The sample period was the 2004–2008 rugby seasons (five seasons). The sample size was not calculated to measure a specific outcome effect.
Injury definitions
The operational definition of injury in RUISS was an injury or medical condition related to a game event that caused a player to miss a subsequent game. Injury severity was defined as the number of games missed by the player as the result of the injury until the player was available again for game selection. Games were scheduled weekly. Severity was categorised as: ModerateA—1 game missed (usually 8–13 days); ModerateB—2–3 games missed (usually 14–28 days) and Severe—missed at least 4 games (usually>28 days). These definitions overlapped with those defined in the rugby consensus statement.22
Data collection
On a weekly basis, injury and participation data were recorded using standardised paper forms by a trained recorder affiliated with each team and communicated to the RUISS research team. Player absences were followed up with team staff to ascertain whether the absence was related to injury. The recorder was typically a trainer, physiotherapist, physiotherapy student or sports science student. Training was provided to each recorder by the RUISS research team and there was weekly communication with each recorder, which afforded the possibility to clarify issues. Common pathology types were recorded for the nature of injury, for example, sprain, dislocation, subluxation for a joint injury; strain and cork/intramuscular haematoma for a muscle injury, bruise/contusion or laceration for a superficial injury and fracture for bone injury. Injuries were recorded by at least: anatomical region of injury, nature of injury and injury event. In addition, detailed injury diagnoses were obtained whenever possible from the team's medical staff. Player positions were categorised as: forwards (Front Row and Back Five) and backs (Halves, Inside backs and Outside backs). All data were entered contemporaneously into a purpose-written database.
Data analysis
IIRs were calculated. Athletic exposure (AE) was used as the denominator for the estimation of IIRs where AE is defined as one athlete participating in one game in which he was exposed to the possibility of athletic injury. Any injury that occurred following return to play was considered a new injury for the purposes of incident rate ratios (IRR) calculation and statistical analyses. The following injury characteristics were analysed: body region, anatomical injury description, nature of injury and severity. Poisson regression with robust variance estimators was applied to assess the relationships between injury and injury risk factors (season, level of play and player position) and IRR were generated. All analyses were undertaken using the SPSS V.18.0 statistical software and the α level was set at 0.05.23
Results
A total of 1475 male rugby players were recruited over the five seasons. Table 1 presents the annual number of participants per level of play; because some players participated in multiple seasons, each participant is treated in table 1 as if he was a new recruit to the study in each season. Using an estimate of 20 potential participants per team, the annual average participation proportion was 56%. A total of 606 upper limb injuries meeting the study definition were recorded by 436 participants during 61 598 AE, including 398 missed game shoulder injuries. Over the five seasons 70.4% of upper limb injured participants had only one upper limb injury and 22.7% had two injuries. On a seasonal basis, the proportions of upper limb-injured participants who suffered at least two upper limb injuries were 11.5%, 16.4%, 14.0%, 11.1% and 24.1% (2004–2008 consecutively). Sixty-five players experienced two injuries to the same upper limb body region in a season and of these 14 (21.5%) occurred during the first game following return to competition. The overall upper limb IIR was 9.84 injuries/1000 AE (95% CI 9.06 to 10.62; table 2). This equates to an estimated 13.12 injuries/1000 player hours on the assumption that each player participated in the entire 80-min game. The highest proportion of injury to the upper limb was to the shoulder (66%) followed by injuries to the hand/finger (20%) and wrist (6%). The shoulder had the highest IIR at 6.46/1000 AE (95% CI 5.83 to 7.09); 8.61 shoulder injuries/1000 player hours. The univariate Poisson regression identified a significant difference in the IRR by upper limb region, with the shoulder three times more likely be injured than to the hand/finger (p<0.05, IRRshoulder=3.34 95% CI 2.75 to 4.05).
Number of teams and participants per season during the period 2004 to 2008. Each participant is treated in this table as if he were a new recruit to the study in each season
Upper limb injury incidence rates and CI by level and region
The upper limb IIR decreased as the level of play increased; 10.74 upper limb injuries/1000 AE (95% CI 9.93 to 11.56) in Colts to 6.07 upper limb injuries/1000 AE (95% CI 5.46 to 6.69) in elite (table 2). In multivariate Poisson regression analysis, upper limb injury incidence was significantly associated with the level of play (p=0.049) with the Elite cohort demonstrating a significantly lower IIR than the reference group of Colts (p<0.05, IRRElite=0.55 95% CI 0.35 to 0.85). Forwards had a higher injury rate than backs, although this was not statistically significant. No associations were found between playing position or season and upper limb IIR.
Because shoulder injuries dominated upper limb injury in terms of the IIR and severity, a separate multivariate Poisson regression analysis was undertaken on only shoulder injuries with respect to level of play, playing position and season. A statistically significant association was found between shoulder injury and playing position (p=0.011). Forwards had a 28% greater chance of shoulder injury compared to backs (p<0.05, IRRforwards=1.28 95% CI 1.06 to 1.55). A significant association was found between level of play and shoulder injury with Elite players having a 51% lower chance of shoulder injury than the Grade and Colts players (p<0.05, IRRElite=0.49 95% CI 0.26 to 0.90). No association was found between season and shoulder injury. Over the five seasons, 73.9% of participants who suffered a shoulder injury had only one shoulder injury and 20.1% had two shoulder injuries. On a seasonal basis the proportions of all shoulder injured participants who suffered at least two shoulder injuries were 11.4%, 16.9%, 20.6%, 9.8% and 15.8% (2004–2008 consecutively). Fifty-one players experienced two shoulder injuries during the same season and of these nine players were injured during the first game following return to play. In four of these cases, the second injury incident resulted in substantial time loss, greater than 9 weeks.
Nature of injury
Descriptive analyses of injury characteristics are presented in tables 3–5. Table 3 presents the selected upper limb injuries by anatomical region and level. Table 3 shows that 75% of shoulder injuries occurred to the three main joints in the shoulder: the ACJ, the GHJ and the SCJ. The ACJ experienced the greatest IIR (2.42/1000 AE). ACJ IIR was highest in the Colts and decreased as the level of competition increased.
Injury incidence rates and CI for selected anatomical regions (full version is available online)
The most common upper limb injuries were: sprains or strains (53%), fractures (17%) and dislocation (11%). Sprains or strains and dislocation injuries were more common to the shoulder, accounting for 79–84% of those categories. Shoulder sprain or strain and dislocation injuries were equally distributed among the three levels of play. Fractures affected the forearm, wrist and hand/finger accounting for nearly 90% of all fracture injuries sustained in the upper limb.
Injury mechanisms
Table 4 presents the IIR for the top five injury mechanisms by level of play. Overall, contact was responsible for nearly 70% of all injuries. Tackling was associated with a slightly higher upper limb IIR than being tackled. Being tackled resulted in a greater upper limb IIR in Colts (2.47/1000 AE; 95% CI 2.08 to 2.86) and decreased as the levels of play increased. Contact was the mechanism of fewer injuries in elite than other levels, and non-contact, such as an overuse, was the highest in the Elite level. Set plays (line outs and scums) were associated with very few upper limb injuries.
Injury incidence rates and CI by mechanism and level of play (full version is available online)
Playing position
The overall IIR for the upper limb was highest in forwards than backs (IIRforwards=7.22/1000 AE 95% CI 6.55 to 7.88; IIRbacks=5.65/1000 AE 95% CI 5.06 to 6.24). In both the forwards and the backs, more than 60% of the injuries occurred to the shoulder, 69% and 61%, respectively. A statistically significant association was found between shoulder injury and playing position as reported earlier.
Injury severity
A total of 32% of all upper limb injuries were classified as severe (table 5). Shoulder injuries caused the highest percentage of time loss in weeks (65%) compared to the other upper limb injuries. Forearm injuries caused the longest average absence (5.3 missed games per injury). In total, the upper limb injuries resulted in players being unable to participate in 2097 games during the study period.
Injury severity by region
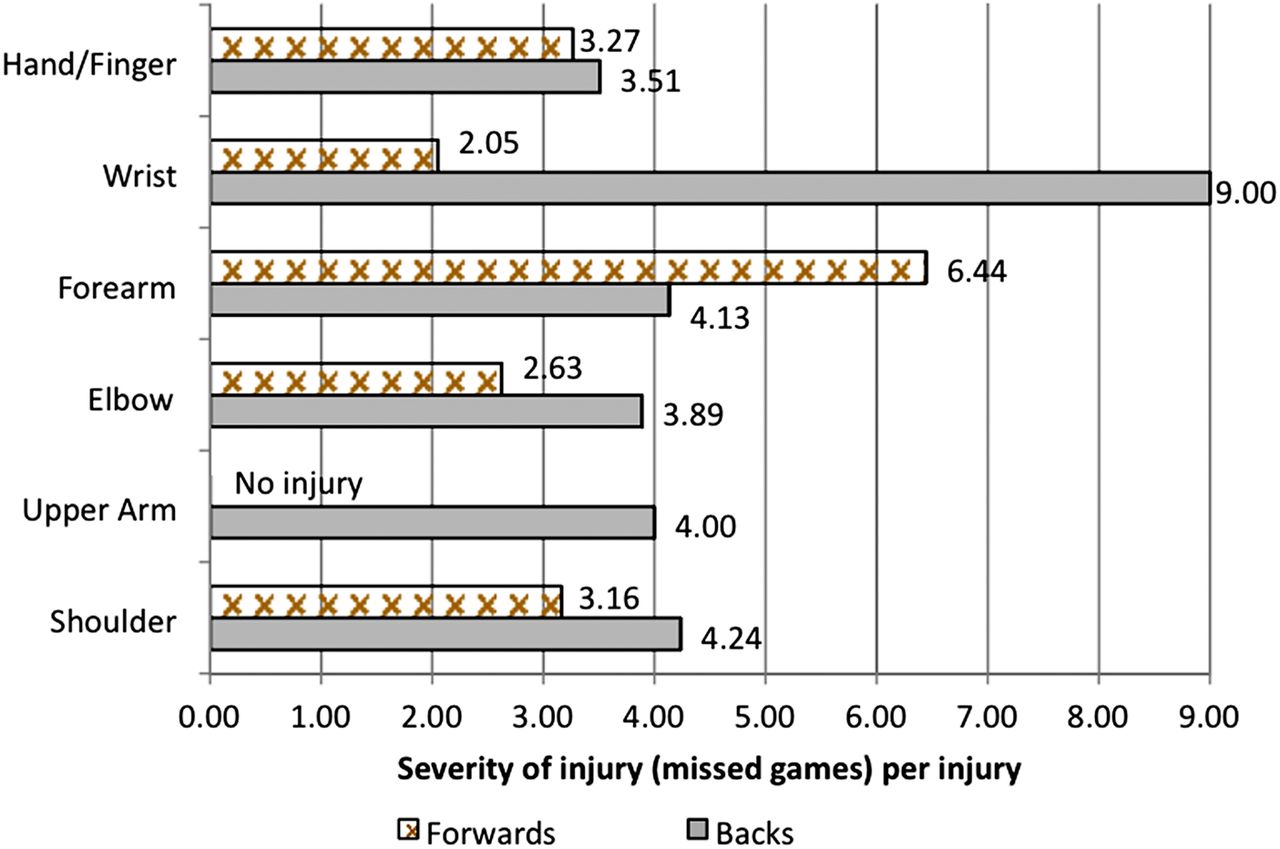
The average injury severity (missed games) per injury by region and playing position is shown in figure 1. The backs had a higher average injury severity than the forwards for injuries to the shoulder, the upper arm, the elbow, the wrist and the hand/finger. In the forearm, the forwards had a higher average severity (6.44 missed games per forearm injury) than the backs (4.13 missed games per forearm injury). Shoulder injuries sustained by backs caused a longer absence than the forwards with the average injury severity of 4.24 games missed per shoulder injury in backs compared to 3.16 missed games per shoulder injury in forwards. The wrist injury severity for backs was much greater (9 missed games per wrist injury) than forwards (2.05 games missed per wrist injury).
{kind=link}
The average severity of injury (missed games) per injury by playing position. This figure is only reproduced in colour in the online version.
The reason for the higher wrist injury severity in backs compared to forwards could be attributed to the fact that almost 62% of the severe injuries were fractures and backs suffered all wrist fractures (100%). Shoulder injuries tended to be more severe in backs compared to forwards. This could be related to the fact that 78% of all fractures were experienced by the backs. Fractures usually required a long period of absence from competition to ensure appropriate healing.
Shoulder injuries in tackles
An ancillary analysis was undertaken to examine shoulder injuries caused by the tackle (see supplementary table S1—available online). Overall, the shoulder IIR caused by the tackle was 3.10 shoulder injuries/1000 AE (95% CI 2.66 to 3.54). The highest injury was to the ACJ and sprain/strain was the nature of injury most often injured, 1.44/1000 AE (95% CI 1.14 to 1.74) and 2.29/1000 AE (95% CI 1.91 to 2.67), respectively. The overall shoulder IIRs showed little difference between the tackler and the ball carrier, 1.51/1000 AE (95% CI 1.20 to 1.82) and 1.59/1000 AE (95% CI 1.28 to 1.91), respectively. Injuries to the ACJ, SCJ and posterior soft tissues in the shoulder affected the ball carrier more than the tackler while the injuries to the GHJ, and the anterior and inferior soft tissues, in the shoulder occurred more frequently to the tackler than the ball carrier. The ball carrier suffered more fractures, and injury to the muscle and tendon, compared to the tackler while sprain/strain, dislocation and superficial injuries were marginally similar or the same for both the tackler and the ball carrier.
Discussion
Using consistent methods over a 5 year period, an average upper limb missed game IIR of 9.84/1000 AE (or estimated 13.12 injuries/1000 player hours) was observed from a total of 61 598 athletic exposures in rugby. The majority of upper limb injuries were to the shoulder (66%). The upper limb IIR in this study was similar to Haseler et al11 but more than three times that observed by Garraway et al (2000).10 Garraway et al's research was conducted in Scottish amateur and professional rugby between 1993 and 1998. The cohort in the current study was Australian elite (professional), Grade (semiprofessional) and Colts (semiprofessional). Since rugby turned professional in 1995 there has been a reported increase in injury incidence. The reason for this apparent increase has been attributed to ball-in-play time and the greater number of tackles, rucks and mauls.24 ,25
While there are numerous studies on elite or professional teams, there is a lack of injury data on semiprofessional and youth players at the Colts level/U20s.3 ,5–8 ,13 ,14 ,18 ,26–28 The current study found that the upper limb IIR decreased as the levels of play increased (Colts → Grades → Elite) and a statistically significant association was found between level of play as a predictor of upper limb injury in general and shoulder injury in particular. This finding was in contrast to previous research where the authors had suggested that IIRs generally increased as the levels of competition increased.3 ,10 ,12 ,21 ,29 The results point towards fitness, playing experience and skill as possible factors underlying the association between injury and level of play.30 ,31 The Colts competition provides an important transition from school based to fully open (age, region, ethnicity and socio-economic background) competitions. Gabbett32 suggested that running speed and strength increased progressively in players in this age group. This may be reflected in the higher upper limb injury incidence in Colts, where together with their increasing running speed and strength the players lack experience, skills and fitness, posing-specific injury risks.
Shoulder injuries were three times more frequent than the next most frequently injured region, the hand/finger. This result correlated well with previous studies that reported the shoulder as one of the top three injured regions, behind the head/neck/face and the lower limb.1–9 The IIR to the shoulder in the current study (6.46/1000 athletic exposure or an estimated 8.61 shoulder injuries/1000 player hours) was within the range reported in non-professional rugby union players (1.0–4.9/1000 player participation hours) and professional players (8.9/1000 player participation hours).10 ,11 ,17 ,18
A possible reason for the high incidence of shoulder injuries compared to other upper limb injuries is that the shoulder is involved as the point of body contact in skills such as the tackle, ruck, maul, scrum and lineout; where there could be as high as 456.8 contact events per game.33 Multiple, reinjury or recurrent shoulder injuries were another factor influencing the shoulder injury incidence with 51 players suffering at least two shoulder injuries, typically two shoulder sprains/strains, in a season. In four cases the second injury incident resulted in an extended absence from the game.
The tackle was identified as the mechanism of 79% of upper limb injuries, which is consistent with previous research.5–8 ,16 ,18 ,20 ,24 ,28 ,33 Regarding any injury, Garraway et al10 and Fuller et al8 reported a higher IIR for being tackled (or the ball carrier), compared to tackling (or the tackler). In this study and in agreement with Headey et al18 tackling had a higher shoulder IIR compared to being tackled. This corresponded well with Fuller et al33 who observed that in the tackle, the highest proportion of injuries to the tackler was the upper limb with shoulder injury being most common. In a separate study the authors measured the average impact load on the shoulder in the tackle to be 1997 N (SD=728).34 Improving the performance of shoulder personal protective equipment, such as shoulder pads which at present do little to manage impact forces, is another area that could be considered with regard to injury prevention.34
As reported in the results, there are some differences in the pattern of injury experienced by the ball carrier and tackler, for example, injuries to the ACJ and SCJ affected the ball carrier more than the tackler. It was difficult to interpret these data without the benefit of a clear mechanism for each injury, for example, the position of the shoulder when struck and whether the injury was caused by a direct impact to the shoulder or through an indirect impact (such as fall on an outstretched hand). The results highlighted the importance of developing better sport-specific understandings of injury mechanisms. Qualitative video analysis of injury events is an approach that has been applied to investigate injury mechanisms and has been successfully implemented in football (soccer) and rugby union.20 ,24 ,28 ,35–37 It is recommended that these methods are applied to study shoulder injury mechanisms in rugby.
A higher proportion of upper limb injuries were observed in forwards compared to backs, which was in agreement with Targett27; Jakoet and Noakes3; Brooks et al7 ; but not Brooks et al13 and Fuller et al.33 A statistical significant association was found for player position and shoulder injury with forwards experiencing a higher IIR compared to backs. In a rugby match, the forwards are usually engaged in more body contact phases in addition to skills involving placing the arm in an overhead posture.
Upper limb injuries caused players to miss the equivalent of 3.4% of the actual athletic exposures. Injuries to the forearm, typically fractures, had the highest average severity with 5.3 missed games per injury compared to the shoulder and hand/finger each with an average of 3.4 missed games per injury. This finding differed from earlier research which suggested that shoulder injuries were the most severe resulting in a higher proportion of days absent from matches and training compared to other injuries.7 ,15 However, in the cohort shoulder injuries were responsible for the greatest overall time loss from competition accounting for 65.3% of total time lost.
A limitation of the study in terms of identifying risk mitigation strategies was the low completion of the classification of the injury event; 37% of the upper limb injury data were classified as ‘unknown’. Rectifying this in future studies may be challenging. Recorders, including team medical staff, are not able to observe closely the game and injured players may not recall exactly how the injury occurred. The use of qualitative video analysis methods is one option, although this is (A) time-consuming, (B) resource intensive and (C) does not always identify the detailed mechanism of injury.20 However, it may be necessary to assume that in the distribution of injury causation (event and mechanism) is the same in the cases where it cannot be coded as it is in the cases that were coded. Unlike professional teams, the injury status of players in other levels of play is difficult to ascertain on a daily basis. Therefore, the ‘missed game injury’ definition applied in this study was adopted across all levels to accommodate operational realities and to provide a basis for comparison. The definition also permitted quality checks to be conducted, for example, review of weekly team sheets, to identify player status. The use of athletic exposures reflects the lack of specific exposure time per player, except at the elite level. All games were 80 min, which provides a basis for comparing AE's to injury rates per exposure hours. For the purposes of the calculation of the IRR and statistical analyses, after a participant returned to competition any injury to the same anatomical region was considered to be a new injury. Some of the second injury incidents may have been a ‘reinjury’ or a recurrent injury, even though the participant was deemed fit to compete and they had participated in a number of games after returning to competition. Future shoulder injury studies in rugby, particularly non-professional rugby, will need to consider how to obtain objective information on shoulder recovery (not just deemed fit to play) and precise shoulder diagnoses in order to examine the issue of repeat shoulder injury. Such research would better inform shoulder rehabilitation and return to play guidelines.
Conclusion
The study highlighted the high incidence and potential severity of upper limb injury in rugby. This study brought new insights into upper limb injury risks in rugby union players. The highlights of the analysis were (1) the shoulder's high injury risk, (2) severity of forearm injuries and (3) association between level and injury risk. Further research is required to explain the high incidence of upper limb injuries in under-20-year-old Colts players and to reduce shoulder injury risk.
-
Shoulder injuries in rugby are associated with a high risk due to their likelihood and severity.
-
The upper limb injury incidence rate (IIR), in general, and the shoulder IIR, in particular, decreased as the level of play increased. This suggests that age, skill, fitness and playing experience could be potential risk factors. Of those, only skill and fitness are modifiable.
-
The tackle and playing position were observed to be potential risk factors for upper limb injuries, in general, and shoulder injuries, in particular.
Acknowledgments
Many people assisted in undertaking the study that deserve acknowledgement. These include: at UNSW—Trevor Savage, Dara Twomey, Maria Romiti and Rebecca Dutfield, and at the ARU—John Searl, Martin Raftery, John Best, Ian Alker, Geoff Shaw and Matt Grimison. In addition the team doctors, physiotherapists, trainers, team management, players and their families from many teams provided immense support during the study. We are extremely grateful for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Contributors Data extraction, analysis and preparation of the paper were undertaken by the authors. The Rugby Union Injury Surveillance Study (RUISS) was conceptualised, coordinated and directed by the author AMc. Data collection and entry were coordinated by a number of project officers employed at UNSW during the course of RUISS, including Trevor Savage, Dara Twomey, Maria Romiti and Rebecca Dutfield.
-
Funding The project was funded by the Australian Rugby Union. No investigator's salary was funded by the sponsor. JU was supported while undertaking this research by a scholarship from the Ministry of Higher Education Malaysia and the University of Malaya, Malaysia.
-
Competing interests None
-
Ethics approval Ethics approval for this study was received from the University of New South Wales Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All data are stored according to the University of New South Wales approved policies and procedures. AMc is the data custodian and chief investigator. Other unpublished data arising from this study, for example, injuries to other body regions and in other cohorts, are being analysed under the supervision of AMc. These data are not available publicly.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com