Article Text

Abstract
Poor frontal plane knee control has been shown to be a risk factor for anterior cruciate ligament injuries in ball/team sports. It is necessary to develop simple tests that can identify players with poor knee control and among other factors be able to optimise preventive training programmes. The present study investigated the correlation between a two-dimensional (2D) video analysis and subjective assessment performed by one physiotherapist in evaluating knee control. We also tested the correlation between three simple clinical tests using both methods. A cohort of 186 female elite team handball players completed three tests: single-leg squat (SLS), single-leg vertical drop jump (SLVDJ) and two-leg vertical drop jump (VDJ). Receiver operating characteristic (ROC) analyses showed good to excellent agreement between 2D video analysis and subjective assessment for SLS and VDJ (area under the ROC curve (AUC) 0.83–0.89), but not for SLVDJ (AUC 0.65–0.76). Poor knee control was detected in 25–40% of the players using SLS and VDJ. In contrast, poor knee control was identified in less than 1% of the subjects based on the SLVDJ test. This indicates that SLVDJ may be inadequate for evaluating poor frontal plane knee control. The correlation between the SLS and VDJ tests was found to be low, suggesting that these tests identified different subjects with poor knee control. These results indicate that subjective assessment can be used to screen for poor knee control and that both SLS and VDJ tests should be used in screening athletes for poor knee control.
Statistics from Altmetric.com
Introduction
Valgus collapse has been reported repeatedly as an injury mechanism for non-contact anterior cruciate ligament (ACL) injury.1,–,3 Several motion analysis studies have demonstrated that females develop larger knee valgus moments and knee valgus angles when performing different athletic tasks compared to males.4,–,8 Knee valgus moment is found to predict ACL injury with 73% specificity and 78% sensitivity.9 Specific training can reduce knee valgus tendency10,–,12 and reduce ACL injury rate.13 14 This strengthens the hypothesis of knee valgus as an important risk factor for ACL injury.
Three-dimensional (3D) motion analysis has been referred to as ‘the gold standard’ in screening athletes for lack of neuromuscular control,15 but it is not applicable on a large population of athletes. A two-dimensional (2D) test of frontal plane knee motion has been found to correlate with 3D motion analysis.15 However, an observer can possibly identify poor frontal plane knee control subjectively as the players are performing different tasks, and thus provide an easy, time- and cost-effective screening tool compared to 2D and 3D approaches.
The drop-jump test found to reveal poor knee control9 is a two-leg exercise, and thus side-to-side differences could be masked and additional tasks to detect neuromuscular deficits may be needed. Real injury situations show that ACL injuries generally occur when the load is primarily distributed to one leg.3 In a single-leg screening test, such as single-leg squat (SLS) and single-leg jump, support from the contralateral leg would be eliminated, and thus it may be easier to identify knee valgus. The kinematics and demands on muscle force and neuromuscular control are likely different in these tests and may therefore identify different athletes with poor knee control.
The first aim of the present study was to determine the correlation between 2D video analysis and subjective assessment performed by one observer in evaluating knee control among elite female team handball players. The second aim was to determine the correlation between three simple tasks using the two methods.
Materials and methods
Subjects
We tested 186 female handball players in the Norwegian elite series and the Norwegian national team (13 teams in total). Their mean age was 22±4 years, mean height was 173±7 cm and mean body mass was 70±8 kg. All players signed an informed consent form prior to participation. The Norwegian Social Data Services and the Regional Committee for Medical Research Ethics approved the study.
Procedure and measurements
This study was conducted as a part of the baseline testing for a prospective cohort study. The players completed three tests performed in the following order; SLS, single-leg vertical drop jump (SLVDJ) and two-leg vertical drop jump (VDJ). Prior to the tests they executed a standardised warm-up programme consisting of a series of two-leg squats (2×8 repetitions) and two-leg maximum jumps (2×5 repetitions), followed by stretching of the calf with straight and bent knee. Players were allowed to familiarise themselves with the test by performing two or three practice repetitions ahead of each test. A minimum of two, maximum of four, valid trials were completed. Small pieces of sports tape were attached to the left and right anterior superior iliac spine and the tibial tuberosities prior to the tests.
Tests
In preparation for the SLS test the players were asked to do a two-leg squat to 90° of knee flexion, measured with a standard plastic goniometer (GYMNA, Berlin, Germany). A thread connected to a metallic object was attached to the lateral aspect of the proximal thigh, just touching the ground as the knee was flexed to 90°. The players performed the test on a metal plate, and the sound from the metallic object when reaching 90° of knee flexion allowed the players to return to the starting point. They were instructed to hold their hands on their hips and focus straight ahead during the squat. A trial was not valid if the other leg was held in front of the body during the squat, if it touched the ground, if the hands were removed from the side of the body, or the player looked down or fell.
The SLVDJ test comprised dropping off a 10 cm box with one leg before immediately performing a maximum vertical jump on the same leg, moving their arms freely. A trial was not valid if the player jumped off the box instead of just dropping, if the other leg touched the ground or if the player was clearly out of balance or fell during the test.
The VDJ test was based on the test described by Hewett et al.9 The player dropped off a 30 cm box with both legs, positioned 30 cm apart in the starting position and was instructed to perform an immediate maximal vertical jump. The players were instructed to attempt touching a handball hanging 260 cm above the ground with both hands. An extrinsic motivator, such as an overhead goal has been shown to alter lower extremity biomechanics, and increase performance.16 A trial was not valid if the player reached for the ball with only one hand or the player lost balance or fell during the performance.
Both legs were tested in the single-leg tests and with regard to the drop-jumps, rating was done in the jump contact phase. A single tester gave all the instructions regarding all three tests.
Subjective assessment
The ability to keep control of the knee during the performance of the tasks was assessed subjectively by a single observer (S.S.) from a frontal view. A graded scale from 0 to 2 was used, where 0 corresponds to ‘good performance’, 1 ‘reduced performance’ and 2 ‘poor performance’. This scale was created on the basis of a group consensus by physiotherapists with extensive experience in athlete screening. The score 0 indicated (A) no significant lateral tilt of the pelvis, (B) no obvious valgus motion of the knee and (C) no medial/lateral side-to-side movements of the knee during the performance. Players rated as 1 displayed (A) some lateral tilt of the pelvis, and/or (B) the knee moving slightly into a valgus position and/or (C) some medial/lateral side-to-side movements of the knee during the performance. Players rated as 2 displayed (A) lateral tilt of the pelvis, and/or (B) the knee moving clearly into a valgus position and/or (C) clear medial/lateral side-to-side movements of the knee (figure 1). The players were rated as 2 if only one of the two-to-four trials were assessed as ‘poor knee control’. At the VDJ test the players were rated as 2 if one or both legs displayed ‘poor knee control’ in the same trial.

Good knee control (A–C) and poor knee control (D–F) subjectively assessed by one physiotherapist during single-leg squat (A, D), single-leg vertical drop jump (B, E) and two-leg vertical drop jump (C, F).
Video analysis
Frontal plane knee angles were measured for each trial within each test. Two digital cameras recorded the motions: One camera (NV-DS65EG; Panasonic, Kadoma, Japan) captured the movements in the frontal plane and a second camera (DCR-HC42E; Tokyo, Japan) recorded sagittal plane motion and was used for validation of the maximal knee flexion angle (figure 2). The recorded videos were analysed on a computer using a commercial software program (Dartfish software 3.0.2.0; Fribourg, Switzerland). We identified the video image with the greatest knee flexion angle by assessing the player's pelvis height during the motion. A single experimenter estimated the frontal knee angles by marking the hip, knee and ankle joint centres directly on that video image (figure 3). We calculated the mean of frontal plane knee angles of the two to four valid trials within each test. For the VDJ test we calculated the mean of frontal plane knee angles for each leg. When comparing the VDJ frontal plane angles to the subjective classification, the mean for both legs was used.

Illustration of the equipment setup.

Estimating frontal plane knee angle during single-leg squat on the video image.
Reliability
Eighteen players from 12 different teams performed all three tests twice, to determine the combined test–retest reliability of player performance and measurement errors. The testing took place the same day, being the first and last test station for the respective players. Analyses were done using both subjective assessment and video analysis; the latter results are presented as absolute values between test and retest.
To assess intratester reliability for the accuracy of the 2D measurement, sequences of 20 randomly chosen players from three different teams were measured twice by the same observer. The time between measurements was approximately 30 days.
Knee flexion verification
Sagittal plane recordings were used to verify the knee flexion angle during the SLS test in a random sample consisting of 25 players.
Statistical methods
Descriptive data are presented as the arithmetic mean, SD and range. Statistical analyses were performed using SPSS (SPSS Science, version 15.0 for Windows, USA). κ Tests were used to compare agreement between tests using categorical variables (degree of knee control). The strength of agreement can be classified as follows: poor (<0.20), fair (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80) and very good (0.81–1.00).17 To determine to what degree the 2D video analysis agreed with the subjective assessments, a series of one-way analysis of variance tests were performed for each test, with the subjectively assessed groups as the between-subject factor. Significant main effects were further analysed using Tukey's post hoc tests. In addition, receiver operator characteristics (ROC) analyses were performed. The ROC analysis tests the ability of the 2D measurements to distinguish the group subjectively assessed as poor from the rest (players with reduced and good knee control). Values range between 1.0 (perfect separation of the test values) and 0.5 (no apparent distributional difference).18 A rough guide for classifying the accuracy is the traditional academic point system: excellent 0.90–1 (A), good 0.80–0.90 (B), fair 0.70–0.80 (C), poor 0.60–0.70 (D) and fail 0.50–0.60 (E). Spearman rank was used to determine the correlation between tests using 2D recordings. Intraclass correlation coefficient (ICC) was determined to assess intratester and test–retest reliability, using a one-way random effects model formula 1.1. For all analyses, an α level of 0.05 is considered statistically significant.
Results
Correlation between tests using subjective assessment
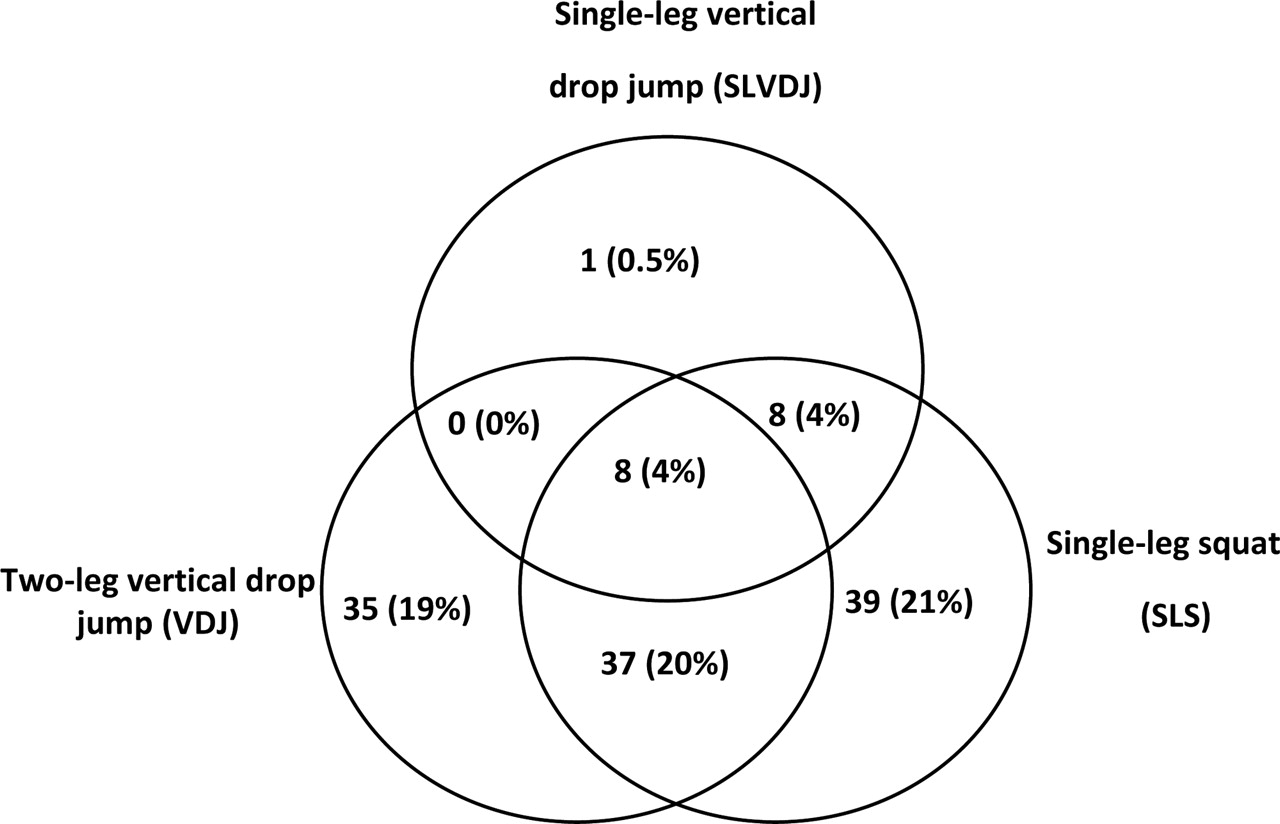
Less than 10% of the players were assessed as having poor knee control in the SLVDJ test, whereas substantially higher percentages were seen in the two other tests (table 1). Likewise, more players were assessed as having good knee control during the SLVDJ test compared to SLS and VDJ. Players assessed with poor knee control can be seen in figure 4. We found poor agreement between the three tests in terms of assessment of knee control (κ values 0.04–0.17).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution (n) of players with poor knee control subjectively assessed by physiotherapist during the three tests. In the single-leg tests the players included in the figure were assessed as having poor knee control in either or both legs.
Subjective assessment of knee control. Distribution of good, reduced and poor control (%) within the different tests
Correlation between tests using 2D frontal plane video analysis
Frontal plane knee angles were smaller in the SLVDJ test than in the other tests (table 2). There were statistically significant correlations (p<0.01) between all tests, with Spearman rank ranging from 0.24 to 0.53, indicating a low to moderate agreement in the ranking of the frontal plane knee angle between the tests.
Frontal plane knee angles (°)
Agreement between subjective assessment and 2D frontal plane video analysis
Players subjectively assessed as having reduced or poor knee control showed increased frontal plane knee angles compared to players subjectively assessed as having good knee control (table 2). Statistical analyses comparing the subjectively assessed groups within each test revealed significant differences, and all groups were significantly different between those with different frontal plane knee angles, except the groups ‘reduced’ compared to ‘poor’ for the SLVDJ test right and left leg. The ROC curve analyses showed a good and excellent ability for the SLS and VDJ 2D frontal plane knee angles to distinguish the subjects classified as having poor knee control, while for SLVDJ it showed fair to poor ability (table 3).
AUC with 95% CI for the three tests
Intratester reliability for 2D frontal plane video analysis
The knee angle difference between the first and second video analysis measurement of the same trial was found to be 3.3° (±2.9) for SLS (n = 100), 2.5° (±2.9) for SLVDJ (n = 79) and 3.0° (±2.4) for VDJ (n = 84), respectively. The ICC1.1 values were 0.92 for SLS, 0.89 for SLVDJ and 0.95 for VDJ.
Test–retest reliability for the different tests
For the subjective assessment, we found good and very good agreement between the first and second test during SLVDJ and VDJ, with κ values of 0.71 (SLVDJ right leg), 0.80 (SLVDJ left leg) and 0.90 (VDJ). κ Values of 0.43 and 0.32 were found between the first and second test during SLS, right leg and left leg, respectively, indicating a fair and moderate agreement. Test–retest reliability for the 2D data is presented in table 4. The smallest test–retest differences were observed for SLVDJ and VDJ.
Difference in frontal plane knee angles (°) between first and second trial for test/retest
Verification of maximal knee flexion angle
The players squatted down to 90.2° (±2.8°) of knee flexion during the SLS test.
Discussion
It is thought to be important to identify poor frontal plane knee control in order to correct an athlete's inappropriate technique. We have seen that subjective assessment could provide similar information as 2D video analysis in terms of identifying elite female team handball players with poor frontal plane knee control, and thus provide a time- and cost-effective screening tool. Further, the results in this study indicate that both SLS and two-leg VDJ may be helpful when screening athletes for poor knee control.
The mean frontal plane knee angles within the three groups (good/reduced/poor) showed an increase with reduced knee control (table 2), indicating a good agreement between the subjective assessment and the 2D analysis. This was confirmed by the ROC analyses. In contrast, the poor agreement that was found between subjective assessment and 2D frontal plane angles in SLVDJ indicates that one or both methods for assessing knee control using this test are unreliable.
The correlation between the tests was found to be poor whether using subjective assessment or 2D frontal plane knee angles, indicating that the three tests challenge different aspects of the athletes' physique and motor control. Subjective assessment of SLVDJ was found to reveal few players with poor knee control compared to SLS and VDJ (table 1). Correspondingly, the 2D analyses showed low mean frontal knee angles during SLVDJ, compared to SLS and VDJ (table 2), suggesting that the sensitivity of SLVDJ, as it was carried out in this study, is likely too low for detecting poor knee control. A possible reason is the motion pattern that was observed during this test. Generally, players performed the SLVDJ in an upright position, with the knee close to full extension. This motion pattern has previously been reported during single-leg landing, described as a ‘stiff’ manoeuvre.19 Such small flexion angles will likely also limit the magnitude of possible knee valgus angles, and thus prevent poor knee control from being detected. In this present study, the SLVDJ test was performed from a box 10 cm in height. Greater peak knee flexion angles during the ground contact phase of single landings from higher jumps have been reported,20 and could to a greater extent reveal true knee control. However, females jumping from a platform 20 cm in height are found to lack sufficient strength to decelerate the body by eccentric quadriceps mechanism in a single-leg landing,21 and this increased demand on the musculoskeletal system could potentially involve risk of injury. The findings, that females landed in an extended knee position and maintained this position rather than absorbing the impact with controlled knee flexion, agree well with the observations of the present study.
VDJ test has been used in several studies with the purpose of examining gender differences and investigating the risk of injury.5 9 22 In comparison with a unilateral step-down task, the bilateral VDJ test has been shown to produce greater knee valgus kinematics in both genders,23 and may therefore be a more suitable test for revealing poor knee control. SLS is another useful clinical measure used in several studies.24,–,26 It is a dynamic task that relates to different functional activities such as landing, running and cutting. It is a controlled movement that puts great demands on strength and balance, and is normally associated with deeper degrees of flexion when compared to a drop jump. It is also more capable of picking out variations between the legs, in comparison to the VDJ test. In the present study 90° of knee flexion were chosen in the SLS test, knowing that squats to approximately 60° of knee flexion were suggested to be insufficient to elicit gender differences in frontal plane knee motion.24 Approximately the same percentage (40%) of players revealed poor knee control on either leg using this test compared to the VDJ test. When comparing these players, only 20% were found to have poor knee control in both of the tests (figure 4), indicating that approximately 20% of the players with poor knee control would not be detected using only one of the tests.
Limitations of the study
A significant limitation of the subjective assessment is the lack of an inter-rater reliability test, making it difficult to predict whether similar results would be achieved by other observers. The test–retest reliability was found to be good and very good in the drop jump tests, but only fair and moderate in the SLS test, findings consistent with the 2D video analysis. However, the good intratest scores suggest that the observed test–retest difference is likely more dependent on subject performance than on measurement error. This variability could possibly be decreased by applying even stricter criteria for upper body posture. It may also be that fatigue has influenced the result, since the players underwent several maximal strength tests of the lower extremity before executing the retest.
In addition, the video analysis has limitations. First, the frontal plane angular measurement does not necessarily represent true knee valgus. Several players rotated their whole body during performance and by doing this a pure knee flexion would give high frontal plane knee angles. Second, only knee angles at maximal knee flexion were assessed. During the SLS several players displayed large lateral-medial fluctuations of the knee qualifying them for the poor knee control categorisation, while the maximally flexed position coincided with a lateral position of the knee. Third, in cases where the players used an excessive upper body forward lean strategy, their hip-joint positions were more difficult to assess as the pelvis position was occluded by the upper body. More advanced 3D analysis could therefore possibly have resulted in better agreement with the subjective assessments.
The comparison between the methods may in some cases be difficult. The players were rated as 2 if only one of the trials were assessed as ‘poor knee control’, while the mean of three trials was chosen in the 2D video analysis to minimise the measurement error. This could lead to a discrepancy between the measurements if the variation between the three trials was large. For the VDJ we calculated the mean frontal plane angles of each leg for comparison with the subjective assessment. In cases with large differences between legs, this could mask a possible excessive valgus motion in one knee. However, in most cases such side to-side differences originated from rotated landings rather than differences in valgus angles.
Conclusions
This study suggests that screening tests can be performed using only visual assessment from an observer. This provides an opportunity for a much more time- and cost-effective way to screen athletes. SLS and VDJ are suitable tasks in tests for assessing knee control in elite, female team handball players, and both should be considered when screening athletes. However, large prospective cohort studies in athlete populations are necessary to investigate whether players subjectively assessed as having poor knee control are in fact at greater risk of sustaining ACL injury.
What is already known on this topic
Knee valgus during sports movements is found to predict anterior cruciate ligament (ACL) injury risk and a three-dimensional motion analysis provides a “gold standard” in screening athletes for knee control. A two-dimensional video analysis method has been shown to successfully screen subjects at increased risk of ACL injury arising from large valgus motions.
What this study adds
This study shows that simple screening tests in evaluating knee control can be performed using only visual assessment. This provides a time- and cost-effective way to screen athletes and can be used in clinical practice to assist practitioners with identifying those most at need of ACL prevention programmes.
Acknowledgments
The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the Norwegian Olympic Committee & Confederation of Sport, Norwegian South-Eastern Health Corporate and Norsk Tipping AS. We thank all the teams and players who participated in this study, and are grateful for the statistical advice of Professor Ingar Holme, PhD.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Norwegian Social Data Services and the Regional Committee for Medical Research Ethics.
-
Provenance and peer review Not commissioned; externally peer reviewed.