Article Text

Abstract
Objective The study examined whether the addition of a night splint to eccentric exercises is beneficial for functional outcome in chronic midportion Achilles tendinopathy.
Design One-year follow-up of a randomised controlled single blinded clinical trial.
Setting Sports medicine department in a general hospital.
Patients 58 patients (70 tendons) were included.
Interventions All patients completed a 12-week heavy load eccentric training programme. One group received a night splint in addition to eccentric exercises.
Main outcome measurements Outcome scores were: Victorian Institute of Sport Assessment—Achilles (VISAA) score, subjective patient satisfaction and neovascularisation score measured with power Doppler ultrasonography (PDU).
Results For both groups the VISA-A score increased significantly (from 50 to 76 (p<0.01) in the eccentric group and from 49 to 78 (p<0.01) in the night splint group). No significant differences in the VISA-A score were found between the groups from baseline to one year (p = 0.32). The presence of neovessels at baseline did not predict a change in the VISA-A score after one year in the whole group (p = 0.71).
Conclusion Eccentric exercises with or without a night splint improved functional outcome at one year follow-up. At follow-up there was no significant difference in clinical outcome when a night splint was used in addition to an eccentric exercise programme. Between 3 months and one year follow-up, a continuing increase in the VISA-A score was found. Assessment of the neovascularisation score with PDU at baseline has no prognostic value on long-term clinical outcome.
Statistics from Altmetric.com
Achilles tendinopathy is the clinical term used when the triad of a painful, swollen tendon with impaired function is present.1 Achilles tendinopathy remains a serious injury for athletes, especially in running sports.1
Several Scandinavian studies have reported good results with eccentric exercises in the treatment of Achilles tendinopathy.2–4 Subsequently other studies showed only moderate results.5 6 More recently, a systematic review concluded that treatment with eccentric exercises possibly has no benefits compared with other forms of exercises.7
Morning stiffness is a common complaint in athletes with Achilles tendinopathy.8 9 It was hypothesised that a night splint would be effective in reducing morning stiffness.
Functional status and return to sports activity were not reported in many previous studies. In a systematic review Kingma et al10 stated that, besides pain, the functional outcome should be scored. The authors proposed to use the Victorian Institute of Sports Assessment—Achilles (VISA-A) score, which measures two factors: pain and physical activity.11 Several studies have used the VISA-A to assess outcome.6 12–15
In Achilles tendinopathy, colour and power Doppler ultrasonography (PDU) shows an increased vascularity with an increased number of blood vessels, which is referred to as “neovascularisation” in the literature.16 The pathophysiological mechanism of these neovessels is unknown.17 Several authors studied the presence of neovascularisation as a prognostic factor for the outcome of treatment of tendinopathy.18 19
The first aim of this single blinded prospective randomised trial was to compare the effects at oneyear follow-up of a heavy load eccentric exercise programme compared with a heavy load eccentric programme in combination with the use of a night splint. The second aim was to evaluate the change in neovascularisation score at one year follow-up.
Material and methods
This is a follow-up study of the randomised controlled trial that initially investigated the value of additional splinting to eccentric exercises with use of the VISA-A score and PDU.5 18
Patients
Patients were referred by a general practitioner, physical therapist or a medical specialist. Volunteers without referral were also allowed for inclusion. Inclusion and exclusion criteria are summarised in table 1. The diagnosis was established based upon clinical examination. When there was pain on palpation of the Achilles tendon, 2–7 cm proximal from the distal insertion, the diagnosis of midportion Achilles tendinopathy was made. If there was pain on palpation of the insertion, this was considered an insertional tendinopathy and the patient was excluded.
Inclusion and exclusion criteria Inclusion criteria
After informed consent was given all patients were included by a clinician and then examined by a single researcher. The study protocol was approved by the Medical Ethics Committee of the Hospital.
Standardised outcome measures were assessed: The VISA-A score was the primary outcome measurement to evaluate the results at follow-up. The VISA-A questionnaire was completed with minimal researcher assistance. The first question in VISA-A is related to morning stiffness (0 to 10). A higher score is associated with less duration of stiffness in the morning. Subjective patient satisfaction was scored as excellent, good, moderate or poor. PDU was performed and neovascularisation was scored according to the modified Öhberg score.18 A detailed exercise instruction was performed. Patients were randomly assigned into one of the treatment groups, using sealed envelopes. The researcher was blinded to this randomisation and patients were instructed not to inform the researcher. Patients who were randomly assigned to the night splint group received further instruction from their treating physician.
Both groups performed treatment for 12 weeks. The detailed description of the treatment has been described earlier.5 Outcome was evaluated by a blinded researcher at baseline, 3 months and one year. When patients needed surgery, the outcome was considered as poor patient satisfaction, the presurgical VISA-A score was obtained and the value used for the final measurement.
Ultrasound examination
On the first appointment Doppler ultrasonography was performed using a linear high frequency 8–13 MHz transducer with a pulse repetition frequency of 868 Hz. (Elegra; Siemens Medical Systems, Erlangen, Germany). At the one-year followup a linear high frequency 12–15 MHz transducer with a pulse repetition frequency of 500–1000 Hz (MyLab30; Esaote Piemedical, Maastricht, The Netherlands) was used. Patients lay prone during the examination, with their feet hanging over the edge of the examination table. The symptomatic Achilles tendons were observed in the longitudinal and transverse plane. On investigation, the researcher and the radiologists scored the neovascularisation of both Achilles tendons. This score was evaluated as 0 (no vessels visible), 1+ (one vessel mostly in the anterior part), 2+ (one or two vessels throughout the tendon), 3+ (three vessels throughout the tendon) and 4+ (more than three large vessels throughout the tendon).
Statistical analysis was performed using statistical package for the social sciences software (SPSS 12.0). To assess changes over time in the variables within groups the Wilcoxon signed rank test was used. The Mann–Whitney U test was used to detect changes over time between the two groups. The x2 test was used to evaluate differences in subjective patient satisfaction between the groups. Statistical significance was assumed when p values were less than 0.05. We calculated that the number of subjects to treat was 26 for each group. This sample size accounted for a 10% loss to follow-up, a significance level of 0.05 and a power of 80%. The assumptions of a delta of 10 points on the VISA-A questionnaire and a standard deviation of 12 were based on the data of previous studies.11 14
Results
Patients
At baseline, 70 tendons of 58 patients met the inclusion criteria. Seventy tendons were randomly assigned into two treatment groups: 34 in the eccentric group and 36 in the night splint group. The mean age was 44.6 years (26–59), the mean body mass index was 25.1 kg/m2 (20.2–34.5). The mean duration of symptoms was 30.7 months (median 44, range 2–204). There were no significant differences in patient characteristics between the groups at baseline.
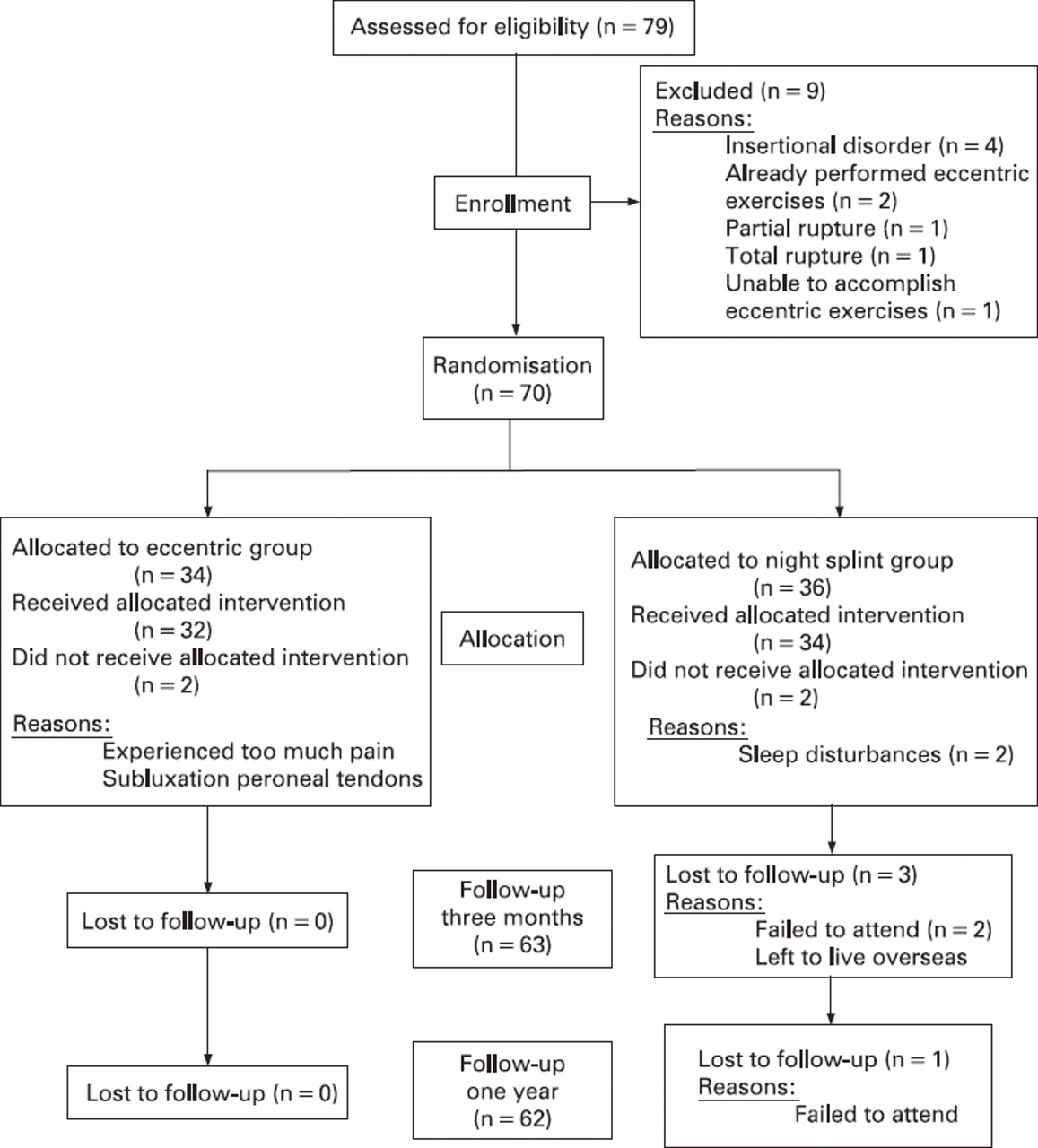
Fifty patients (63 tendons) could be included for follow-up at one year. One patient did not answer repeated phone calls and 10 patients were not able to visit our centre for PDU examination but did complete the VISA-A scores and patient satisfaction (fig 1).

Flowchart of patients in the study.
Between 3 months and one year follow-up, six patients (seven tendons) did not respond to conservative treatment. All had a poor/moderate patient satisfaction score at 12 weeks follow-up. These patients underwent surgical treatment after a mean duration of 9 months (6–12). In these patients, the presurgical VISA-A scores were obtained.
Eccentric training
Some patients continued the eccentric exercises at a lower level after the 12 weeks exercise programme. Eleven patients (14 tendons; 22.6%) continued for 1–6 months (mean 2.5 months). Eight patients (nine tendons; 14.5%) were still doing the exercises at the one year follow-up.
VISA-A score
The VISA-A score in the eccentric group increased significantly from 50.1 at baseline to 75.7 after one year (p<0.01). From 3 months to one year the VISA-A score also increased significantly from 68.8 to 75.7 in the eccentric group (p = 0.02). In the night splint group the VISA-A score increased from 49.2 at baseline to 78.2 at one year (p<0.01; fig 2). A significant increase was also seen from 3 months follow-up (65.9 points) to one year follow-up (p<0.01).

Changes in the Victorian Institute of Sports Assessment— Achilles (VISA-A) score in both treatment groups at baseline, 3 months follow-up and one year follow-up. No significant differences were found between the two treatment groups. A significant increase for the eccentric and night splint group between 3 months and one year followup was found.
There was no significant difference found in increases in VISA-A scores between both groups from baseline to one year (p = 0.36) and from 3 months to one year (p = 0.24; fig 2)
The score for morning stiffness increased significantly in the eccentric group from 5.8 at baseline to 9.1 at one year follow-up (p<0.01). In the night splint group the score for morning stiffness increased significantly from 4.7 at baseline to 8.7 at one-year follow-up (p<0.01). There was no significant difference in morning stiffness between both groups at baseline (p = 0.19), 3 months follow-up (p = 0.09) and one year followup (p = 0.12).
Subjective patient satisfaction
As described in table 2, patient satisfaction at one year followup in the eccentric group was excellent or good in 17 (53.1%) tendons and moderate or poor in 15 (46.9%) tendons. After one year the patient satisfaction in the night splint group was excellent or good in 21 (70%) tendons and moderate or poor in nine (30%). No significant difference in patient satisfaction was found between the eccentric group and the night splint group (p = 0.20).
Subjective patient satisfaction in both treatment groups at one year follow-up
Ultrasonographic neovascularisation
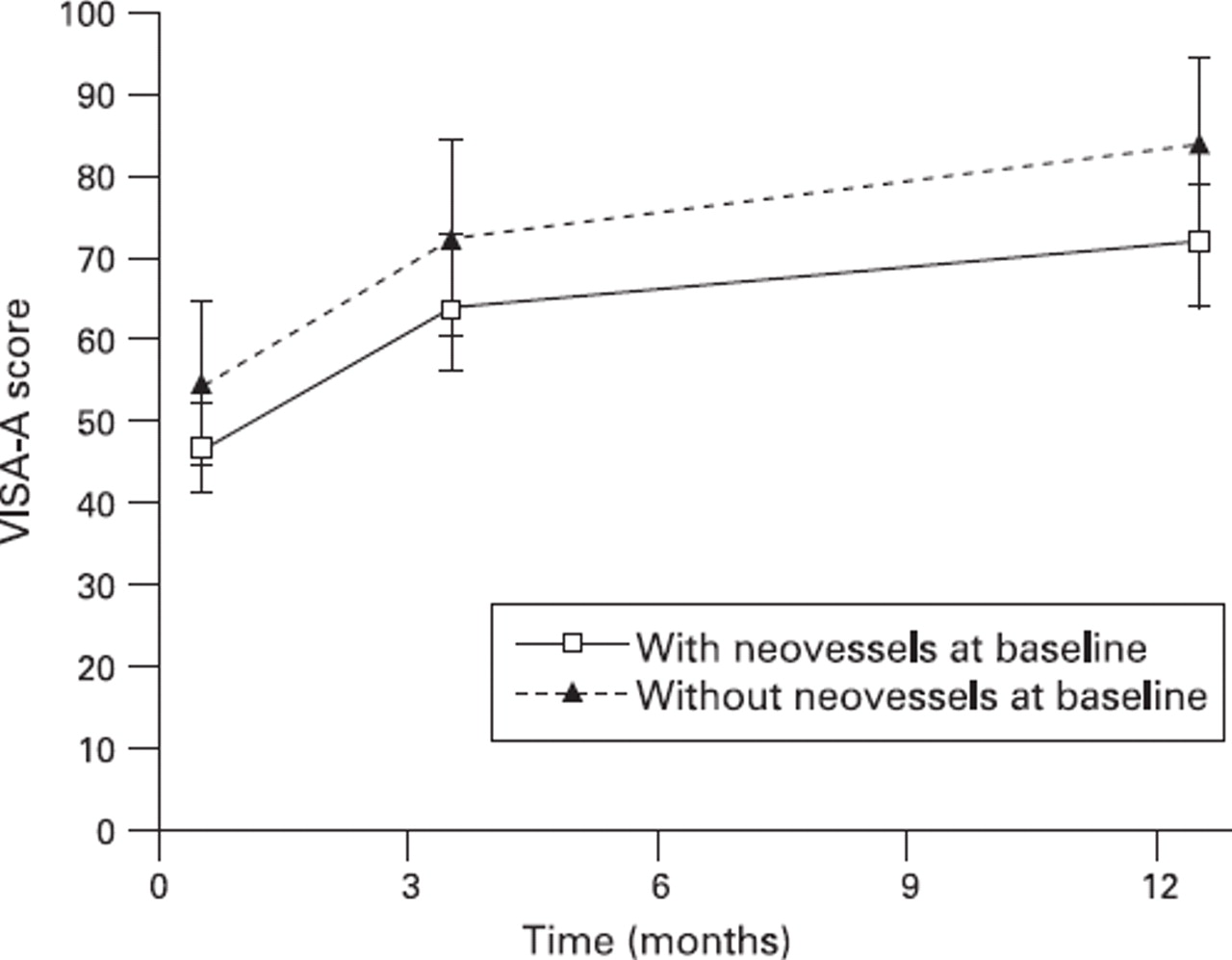
At baseline 40 (65%) of the 62 tendons showed some degree of neovascularisation. At one year 37 of 52 (71%) showed some degree of neovascularisation. Patients with neovessels at baseline (grades 1–4) showed a mean increase in the VISA-A score of 25.7 from baseline to one year follow-up. Patients without neovessels (grade 0) at baseline showed a mean increase of 30.1 in the VISA-A score. There was no significant difference in outcome measured with the VISA-A between patients with or without neovessels at baseline (p = 0.71; fig 3)
{kind=link}
{kind=link}
{kind=link}
Changes in the Victorian Institute of Sports Assessment— Achilles (VISA-A) score at baseline, 3 months and one year follow-up in patients with neovessels (grades 1–4) at baseline and without neovessels at baseline (grade 0). There was no significant difference in improvement inthe VISA-A score between these groups at 3 months and one year follow-up.
Discussion
This randomised trial shows that at one year follow-up there was no difference in functional outcome between treatment with eccentric exercise only or a combination of eccentric exercises and the use of a night splint in chronic Achilles tendinopathy. The improvement in the VISA-A score continued after finishing the 12 weeks of therapy. The presence or absence of neovascularisation within or around the Achilles tendon could not predict outcome at long-term follow-up.
All studies that compared short-term versus middle and longterm outcomes, showed an improvement in the results between 6–12 weeks and one year.9 12 20 It is questionable if the improvement after a period of 3 months eccentric training is caused by continuing the eccentric exercises after the prescribed 3-month period. In our population almost a quarter continued the eccentric exercises for 2.5 months on average after finishing the therapy programme. At one year follow-up 15% were still performing the eccentric exercises. This phenomenon has not been reported in previous studies.
Another explanation is the “slow” natural healing process of the tendon. The effect of natural healing examined with a wait and see policy, was recently studied by Rompe et al.14 They reported that an increase in the VISA-A score from 48 to 55 was found after 4 months without treatment. This improvement was not statistically significant. Another hypothesis is that eccentric exercises elicit longer term adaptations in extracellular matrix production. Tendons can adapt to enhanced loading conditions by changing tenocyte metabolism, leading to an alteration of structure and composition; however, the process of tissue degradation, and the synthesis and incorporation of new matrix components as well as the final crosslinking of the newly produced collagen network takes time. Altered biomechanical loading conditions can influence tendon cell (tenocyte) metabolic activities, altering the production and degradation of extracellular matrix components.21 In humans it has been demonstrated using a microdialysis technique that collagen type I synthesis is increased after 12 weeks eccentric loading of initially injured human Achilles tendons.22 From veterinary medicine we know that the tendon repair process in equine superficial digital flexors including the final remodelling phase takes many months.23 Therefore, it is likely that the remodelling of the tendon tissue will continue for a longer period even after ceasing the eccentric loading regime. Ultimately this might lead to tendon structure adaptation and improved tendon function at long term.24
What is already known on this topic?
▶. Eccentric exercises are widely used and are effective in pain reduction in the treatment of chronic Achilles tendinopathy.
▶. The role of neovascularisation as a prognostic factor remains questionable.
What this study adds?
▶. There is no benefit of adding a night splint to eccentric exercises in the treatment of Achilles tendinopathy.
▶. There is a continuing improvement in pain and function between 3 months and one year follow-up of conservative treatment.
▶. The neovascularisation score at baseline has no prognostic value for clinical outcome.
It may also be that patients might notice an initial relief and symptomatic recovery, which frequently precedes a functional recovery. It has been described that an initial symptomatic recovery reached shortly after the eccentric exercises does not automatically lead to a long-term functional recovery.25 A postponed or extended period of restoration of tendon tissue structure and function might be responsible for the continuing increase in the VISA-A score after the eccentric exercises.
Few studies reported the functional results of more than one year follow-up. In a study in non-athletes with a mean followup of 15 months, Sayana and Maffulli6 have shown the VISA-A scores of 34 patients after a 12-week heavy load eccentric exercise programme. In their population a significant increase in the VISA-A score from 39 to 50 was found, which was a smaller improvement than in this study. A possible explanation is the difference in the study population. In the study of Sayana and Maffulli6 the patients were non-athletes, whereas in this study the included patients were all participating in sports. It could be postulated that active individuals do have a better compliance for the prescribed exercises. The VISA-A scores after one year in the study of Brown et al12 are more comparable with the present study. Those authors showed an improvement from 62 to 95 in 18 patients treated with eccentric exercises plus an injection of aprotinin or placebo. Other studies also showed an increase in VISA-A scores after finishing the eccentric programme.5 14 15
In contrast to the hypothesis that a night splint would reduce morning stiffness, the results in the present study did not show a significant benefit of using a night splint for the duration of stiffness in the morning.
There is conflicting evidence on the significance of neovascularisation in Achilles tendinopathy.26 Peers et al27 found a correlation between neovascularisation and pain scores and Reiter et al28 reported a relationship between the presence of neovascularisation and a worse VISA-A score. However, these data were not supported by Zanetti et al,19 and de Vos et al18 found no relationship between the visual analogue scale score or the VISA-A score and the presence of neovascularisation.
In this study there was no relationship between neovascularisation at baseline and clinical outcome at one year. Zanetti et al19 and de Vos et al18 analysed the presence of neovessels at baseline related to outcome after 3 months of conservative treatment and reported similar results.
The use of a night splint in Achilles tendinopathy has been studied by Roos et al.9 They reported a pain reduction of 35–42% at one year follow-up in all patients treated with eccentric exercises, a night splint or a combination of both. There was no significant difference in pain reduction between these groups after one year.
At one-year follow-up another PDU device was used. Although the pulse repetition frequency did not differ much, comparison between baseline and one-year follow-up could be unreliable. Another weakness of this study is the high number of patients who were not able to attend for PDU examination at one year follow-up. An intention-to-treat analysis was used for the patients who received conservative treatment to avoid bias. However, because some patients received surgical treatment they were not comparable with the group of patients treated conservatively. Therefore, these tendons were scored as poor patient satisfaction with the presurgical VISA-A score. A type II error may have occurred in the present study; however, with a total of 62 patients analysed at follow-up a high power was achieved.
Conclusion
Eccentric exercises, with or without a night splint, improved functional outcome after one year follow-up in patients with chronic Achilles tendinopathy. At follow-up there was no significant difference when a night splint was used in addition to an eccentric exercise programme.
There was a continued improvement in functional outcome between 3 months and one year. Thirty-seven per cent of the patients treated with eccentric exercises continued to perform them after the 3 months prescribed duration.
The presence of neovascularisation at baseline did not predict pain and functional outcome at one year follow-up. Seventyone per cent of the tendons still showed some degree of neovascularisation at follow-up.
Acknowledgments
The authors would like to thank Ms M de Mos (PhD student, Orthopaedic Research Laboratory, Erasmus Medical Centre, Rotterdam, The Netherlands) for her contribution in the field of basic biological response to exercise.
References
Footnotes
-
Competing interests None.
-
Ethics approval The study protocol was approved by the Medical Ethics Committee of the hospital.
-
Patient consent Obtained.