Article Text

Abstract
Objectives: The cellular basis of painful tendon overuse pathology (tendinosis) is poorly understood. It has been suggested that because of the close anatomical associations between mast cells and vessels in connective tissues, mast cells may mediate the development of tendon hypervascularity or oedema.
Objectives: To examine the distribution of mast cells in men and women with patellar tendinopathy.
Design: Case–control study.
Methods: Tendinopathic tissue was collected at open debridement of the patellar tendon and a control tendon from patients undergoing intramedullary nailing of the tibia. The tendon was assessed immunohistochemically by evaluating the distribution of mast cells (AA1), and markers for T lymphocytes (CD3) and macrophages (CD68). The vessel-area fraction was quantified using computer-assisted digital image analysis.
Results: The prevalence of mast cells per mm2 (mean 3.3 (SD 3.0)) was greater in tendinosis tissue than in controls (1.1 (1.5); p = 0.036). In patients with tendinosis, mast cell density was moderately correlated with the vessel-area fraction (r2 = 0.49) and with symptom duration (r2 = 0.52).
Conclusion: Mast-cell prevalence in patellar tendinopathy was increased and was predominantly associated with vascular hyperplasia, particularly in patients with longstanding symptoms. Future research should investigate whether mast cells play direct or indirect modulatory roles in the development and progression of human tendinosis.
Statistics from Altmetric.com
Repetitive overuse tendon injury (tendinopathy) is a major burden on the healthcare system and a challenge to orthopaedic and sports medicine practitioners.1 Clinical symptoms include pain, swelling, and impaired function.1 2 Colour Doppler ultrasound reveals excessive vascular flow in tendinopathy and this finding has been associated with the presence of tendon pain.2 3
Despite the increased vascular flow and vascular hyperplasia that characterise tendinosis, an acute cellular inflammation (neutrophils, macrophages, lymphocytes) is rarely reported in the chronic stages. This lack of typical acute inflammatory cells has led to increasing adoption of the term “tendinosis” as opposed to “tendonitis”.4 Recently, Schubert et al5 compared the numbers of CD68+ macrophages, CD3+ T lymphocytes, CD20+ B lymphocytes, and granulocytes in 10 patients with Achilles tendinosis and 10 patients with an acutely ruptured Achilles tendon. In this study, patients with tendinosis displayed increased numbers of macrophages and lymphocytes in association with hypervascular tissue, whereas patients with acutely ruptured tendon displayed greater numbers of granulocytes.5 Thus, inflammatory and reparative cell types may play a role in the pathogenesis of tendinosis and the development of vascular hyperplasia in chronic tendon lesions.
Along with macrophages and lymphocytes, mast cell numbers are also known to be increased in a variety of chronic inflammatory or fibrotic disorders. In addition to their well known physiological role in triggering allergic reactions, mast cells release a variety of vasoactive, angiogenic and profibrotic substances that are either stored in granules or synthesised de novo in response to hypoxia, mechanical stimulation, or neurological and inflammatory mediators.6–8 Mast-cell products of potential relevance to overuse tendinopathies include histamine, prostaglandins, leucotrienes, growth factors and proteinases.9 10 Despite this, to our knowledge the distribution of mast cells has not been examined in tendinosis tissue. Therefore, in the current study we examined their distribution in both normal and chronically painful patellar tendons. We hypothesised that because of the anatomical proximity of vessels and mast cells in connective tissues,7 11 mast cells would be more prevalent in tendinosis than in control tendon tissue, and would be correlated with the vessel-area fraction.
METHODS
The study was approved by the university and hospital research ethics committees, and all patients provided written informed consent.
Participants
In total, 21 patients (18 men, 3 women; mean age 30.4 years, range 22 to 40) and 10 control subjects (7 men, 3 women; mean age 28.2 years, range 20 to 42) were included. Patients were athletes who had had at least 3 months of patellar tendon pain and tenderness that was sufficiently severe to prevent them from participating in sports. The mean symptom duration was 22 months (range 5 to 81). MRI confirmed high signal changes corresponding to the area of symptoms (infrapatellar pole). The control group consisted of patients treated with intramedullary nailing for tibial fractures with no current or previous knee pain.
Exclusion criteria were age <18 years, previous knee surgery, corticosteroid injections in or around the knee, knee trauma requiring medical attention, and rheumatic or degenerative knee conditions.
Biopsy procedure
The surgical exposure was identical in the two groups, with a 5 cm longitudinal midline or lateral parapatellar incision, splitting of the paratenon and exposure of the patellar tendon. The paratenon was split longitudinally, any pathological paratenon tissue was removed and the tendon was fully exposed. In both groups, the biopsies were taken from the proximal bone–tendon junction. The tendon tissue was excised using a full-thickness, wedge-shaped incision, being widest at the patellar pole and narrowing distally. In the patient group, all abnormal tissue was removed. When abnormal tissue was not evident macroscopically, the excision was based on the location of MRI signal changes. Typically, the surgeon removed a wedge with a proximal base 1 cm wide and extending to an apex 2–3 cm distal from the patellar pole. In the control group, the biopsies were taken with a width of at least 5 mm and a length of at least 20 mm from the middle portion of the tendon starting at the bone–tendon junction. Immediately after the surgical procedure, biopsies were transferred to Zamboni’s fixative where they were stored for 4–24 h, and then washed in 0.1 mol/l phosphate-buffered saline (PBS) pH 7.2, with 15% sucrose (w/v) and 0.1% natriumazide. The biopsies were then stored in this solution at 4°C for a minimum of 48 h after which they were embedded in paraffin wax.
Appearance under light microscopy
Sections of 5 μm thickness were cut and stained routinely with H&E (general morphology) and alcian blue (sulphated glycosaminoglycans) and viewed at 100–630 times magnification (Zeiss Axioplan upright microscope; Zeiss, Berne, Switzerland). Areas of adipose or peritendinous tissue were avoided during analysis. Absence of visible tendon pathology with H&E staining was confirmed in each case in the control group. Tendinosis was defined according to the features of the Bonar histopathological scale.12 Briefly, this scale defines tendinosis according to the presence of four features; hypervascularity, collagen disorientation, tenocyte rounding (ie, chondroid metaplasia), and increased glycosaminoglycans.12
Labelling of cell types
The following mouse monoclonal antibodies were used to identify cell types: CD68 (Signet KP1 clone; Cedarlane Laboratories, Hornby, Canada) for macrophages, CD3 (clone F7.2.38; DakoDiagnostics, Glostrup, Denmark) for T lymphocytes, and mast cell tryptase (clone AA1; Dako) for mast cells.13–15 Processing for mast cell tryptase was carried out using an autostainer (Dako). The sections were cleared in xylene (3×15 min), steamed in sodium citrate for 3×5 minutes, incubated at 37° with 0.1% trypsin in 0.1% calcium chloride pH 7.3 for 5 minutes, quenched for 15 minutes in 3% hydrogen peroxide, incubated in protein-free blocking solution (Dako) for 15 min, then exposed to 100 μl of primary antibody diluted 1:50 in 0.1% bovine serum albumin in Tris-buffered saline for 1 hour. A secondary anti-mouse IgG antibody (Dako) was then added, followed by incubation with alkaline phosphatase–anti-alkaline phosphatase (Dako) for 30 minutes. The signal was visualised with new fuchsin (Sigma-Aldritch, Oakville, Canada) as the substrate. Identically fixed and processed tonsil tissue with or without the mast cell tryptase antibody was used as positive or negative control, respectively. CD68 processing was identical to the mast-cell protocol but without the trypsin pre-treatment. For T lymphocytes, the CSA II detection system (Dako) was used, with 3,3′-diaminobenzidine as the chromogen (Vector Laboratories, Burlingame, California, USA). Human tonsil was used as a reference for all cell types. Mast cells, lymphocytes and macrophages were found to be labelled only in the positive tonsil tissue controls.
Image analysis
Slides were examined with the patient/control identity code masked with black tape. For quantification of mast cell density, the 10 most proximal viewing fields at ×40 magnification were captured in a pre-determined raster pattern, and the number of positive cells per mm2 calculated. Vessel-area fraction was quantified on H&E sections (10 most proximal ×40 viewing fields) using image-analysis software (Northern Eclipse; Empix Imaging, Cheektowaga, New York, USA). Vessels were manually outlined onscreen using a mouse, and the area occupied by vessels was expressed as a percentage of the slide area.
Data analysis
Results are presented as means (SD). Mast-cell density was counted on two separate occasions by a single observer (AS) and averaged (intrarater reliability, r2 = 0.75). Mast-cell density in normal and patellar tendinosis tendons was compared using the non-parametric Mann-Whitney U test for independent samples. Correlation between mast cell density and vessel-area fraction, and between mast cell density and symptom duration, were conducted using Pearson’s correlation analysis. All statistical tests were carried out using SPSS V.14.0
RESULTS
Light microscopic appearance
One control patient had tenocyte rounding in the proximal patellar tendon suggestive of chondroid metaplasia, but no other features of tendinosis pathology. All patients with tendinosis showed all four features of tendinosis pathology as defined by the Bonar histopathological scale:12 vascular hyperplasia, collagen disorientation, tenocyte rounding and increased glycosaminoglycan.
Prevalence of mast cells in patient biopsies
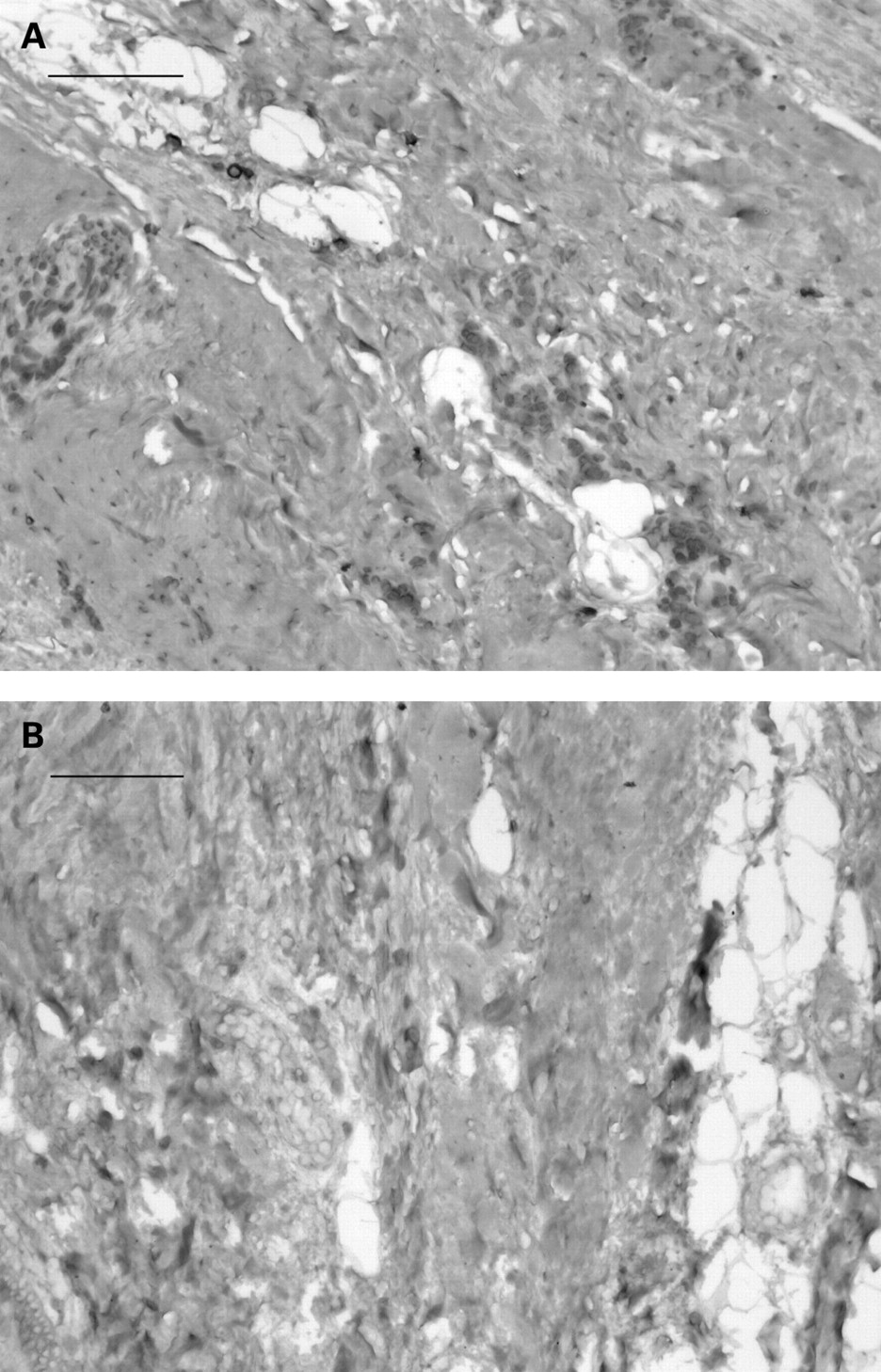
CD3+ lymphocytes and CD68+ macrophages were present too infrequently in either patient or control tendon tissue to be practically quantifiable, despite being readily identified in tonsil tissue. Conversely, there were a greater number of prominent mast cells in patient tendon biopsies. The mast cell density (mean 3.35 (SD 3.5) cells/mm2] was three times greater in tendinosis tissue than in control tissue (1.0 (1.5) cells/mm2) (fig 1). The mast cells were typically present in a perivascular distribution in areas of increased vessel density within the tendon proper (figs 2–5). In 5/22 cases of tendinosis, and 0/10 controls, mast cells were also occasionally observed within the tendon proper—that is, between longitudinal collagen bundles.





Correlation of mast cells with tendon vascularity
Capillaries, arterioles and venules were present in both patient and control biopsies. Patient biopsies consistently showed a greater number of vessels in the posterior, proximal substance of the tendon proper. However, the increase in vascular area (2.8% (3.2) in patients vs. 1.2% (2.2) in controls) was not significant. There was a moderate but significant correlation between mast cells and vessel-area fraction (r2 = 0.49, p<0.01).
Correlation of mast cells with symptom duration
Mast cells were found to be most prominent in biopsies from patients with a longer reported symptom duration. There was a moderate but significant correlation between symptom duration and numbers of mast cells in patients (r2 = 0.52; p<0.05).
DISCUSSION
In tendons obtained from symptomatic patellar tendinopathy, the mast cell density was three times higher than in control tendons and was positively correlated with symptom duration. In addition, mast cells were usually found in association with tendon vascularity. In support of this observation, mast cell density was significantly correlated with the vascular area fraction (r2 = 0.49). These findings suggest that the accumulation of mast cells in tendinosis may be a feature of the chronic stage of tendon pathology and in associated with vascular hyperplasia.
Novel findings of tendinosis cellularity
We identified a relatively high number of intratendinous mast cells, the first direct evidence that this cell type is over-represented in tendinosis tissue compared with control tendon. Classic descriptions of tendinosis tissue obtained from patients undergoing surgery for overuse tendinopathy have not reported prominent mast cells.16–20 Increased numbers of mast cells are common in many chronic inflammatory or fibrotic conditions, such as disorders of the joints, gastrointestinal tract, liver and respiratory system. Mast cells proliferate at sites of injury and in turn release a range of profibrotic factors including transforming growth factor (TGF)β and interleukins 1 and 4.6 Mast-cell tryptase can also act directly on fibroblasts by triggering proteinase-activated-receptor-2 (PAR-2), thereby inducing a cyclooxygenase-2-dependent proliferative and fibrotic response in fibroblasts.21 Thus, the potential exists for previously undocumented interactions between mast cells and tenocytes.
Potential role of cellular inflammation in tendinosis
Achilles tendinopathies with symptom duration <3 months have been found to have a favourable clinical responses to corticosteroids delivered by iontophoresis, including a reduction in pain and morning stiffness, suggesting the existence of an acute or subacute inflammatory phase that was not captured in the present study.22 In support of this clinical observation, several cellular and molecular features of tendinosis suggest the existence of a chronic inflammatory or fibrotic response including increased expression of TGFβ, increased levels of proteoglycan and collagen III, high intratendinous lactate levels, increased numbers of myofibroblasts, and increased fibroblastic turnover (apoptosis and proliferation).23–30 In keeping with these previous studies, the present data show that increased numbers of mast cells, a well-known component of soft tissues in the chronic inflammatory or fibrotic phase of injury, is indeed present in the patellar tendons of patients with symptoms of pain and swelling for >3 months, and that the mast cell number may be higher in patients with longer symptom durations.
In contrast to the current study, Schubert et al5 found an increased density of CD68+ macrophages and CD3+ T-lymphocytes in chronically painful Achilles tendons compared with ruptured tendons, which showed an increased density of granulocytes (ie, neutrophils). This suggests that tendinosis may be characterised by an evolving population of invading and locally proliferating cell types, with neutrophils predominant in the early phases, followed by macrophages and lymphocytes, and eventually mast cells and vascular cell types.6 Indeed, only a few of the patients in the study by Schubert et al had a symptom duration of >12 months, compared with the majority of patients in the current report. This may account for the discrepancy in terms of the number of observable macrophages and lymphocytes between the two studies. A further discrepancy between these two studies is that several of the patients in the Schubert et al study had received corticosteroid injections, which can potentially result in necrosis and focal inflammation.31 In contrast, no patient in the current study had received any corticosteroid injection in or around the patellar tendon.
Potential role of neurogenic inflammation in tendinosis
The mast cells observed in the current study were positive for mast cell tryptase, which is a potent angiogenic factor.11 Mast cells are also capable of producing a potent neurotrophin, nerve growth factor,32 which is an interesting feature given recent findings that, in addition to angiogenesis, neural sprouting is a prominent feature of tendinosis.5 Our cross-sectional study did not allow us to determine whether the prominence of mast cells is causally associated with the abnormal tendon vasculature and its accompanying sensory and autonomical innervation, which are strongly implicated in symptomatic tendinopathy.33–38 Nonetheless, the findings tempt speculation that mast cells may play proangiogenic and/or neurotrophic roles in tendinopathies. Because the potential exists for multiple paracrine intereactions between mast cells, nerves, endothelial cells, and tenocytes, much work will be required to determine the possible roles of mast cells at different stages in the development and progression of tendinosis. One possible set of interactions is presented in fig 6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is already known on this topic
Patellar tendinopathy is characterised by increased cellularity, increased vascular flow and angiogenesis.
In the chronic phase of tendinopathy lesions, acute inflammatory cells are minimally present.
Mast cells are known to play an important role in soft tissue healing and fibrosis, but their distribution in tendinopathy has not been examined previously.
What this study adds
Mast cells are present to a greater degree in patellar tendinopathy, usually in association with microvessels, and particularly in patients with longstanding symptoms.
Mast cells express tryptase, a potent angiogenic factor, and may therefore play a role in mediating the angiogenic process.
CONCLUSION
In summary, we have quantified the density of mast cells in human patellar tendinopathy tissue and found them to be significantly increased in comparison to healthy tendon. Further, we have found that raised mast cell numbers in the patellar tendon are correlated with both the symptom duration and the vessel-area fraction. These observations highlight the need for mechanistic and longitudinal studies to clarify the role of mast cells in tendinopathy.
Acknowledgments
We thank J McDonough for helpful suggestions and A Samrai for excellent technical services, both at the James Hogg iCapture Centre, Vancouver, British Columbia, Canada.
REFERENCES
Footnotes
Competing interests: None.
Funding: This work was funded by grants from the Canadian Institutes of Health Research (CIHR) (grant MOP-77551) and the Worker’s Compensation Board of British Columbia (grant RS0203-DG-13). The Oslo Sports Trauma Research Center has been established at the Norwegian University of Sport and Physical Education through generous grants from the Royal Norwegian Ministry of Culture, the Norwegian Olympic Committee and Confederation of Sport, Norsk Tipping, and Pfizer. The funding agents played no role in study design or manuscript preparation. AS is a recipient of a CIHR Post-Doctoral Fellowship. DAH is the Calgary Foundation-Grace Glaum Professor in Arthritis Research and supported by the Institute of Gender and Health of CIHR. VD is a recipient of a Michael Smith Foundation for Health Research Senior Scholar Award. KMK is a recipient of a CIHR New Investigator Award.
Ethics approval: Ethics approval was obtained from the university and hospital ethics committees.