Article Text

Abstract
Objectives: To determine the impact of the application of cryotherapy on nerve conduction velocity (NCV), pain threshold (PTH) and pain tolerance (PTO).
Design: A within-subject experimental design; treatment ankle (cryotherapy) and control ankle (no cryotherapy).
Setting: Hospital-based physiotherapy laboratory.
Participants: A convenience sample of adult male sports players (n = 23).
Main outcome measures: NCV of the tibial nerve via electromyogram as well as PTH and PTO via pressure algometer. All outcome measures were assessed at two sites served by the tibial nerve: one receiving cryotherapy and one not receiving cryotherapy.
Results: In the control ankle, NCV, PTH and PTO did not alter when reassessed. In the ankle receiving cryotherapy, NCV was significantly and progressively reduced as ankle skin temperature was reduced to 10°C by a cumulative total of 32.8% (p<0.05). Cryotherapy led to an increased PTH and PTO at both assessment sites (p<0.05). The changes in PTH (89% and 71%) and PTO (76% and 56%) were not different between the iced and non-iced sites.
Conclusions: The data suggest that cryotherapy can increase PTH and PTO at the ankle and this was associated with a significant decrease in NCV. Reduced NCV at the ankle may be a mechanism by which cryotherapy achieves its clinical goals.
- ANOVA, analysis of variance
- CON, control
- EMG, electromyogram
- EXP, experimental
- NCV, nerve conduction velocity
- PTH, pain threshold
- PTO, pain tolerance
Statistics from Altmetric.com
- ANOVA, analysis of variance
- CON, control
- EMG, electromyogram
- EXP, experimental
- NCV, nerve conduction velocity
- PTH, pain threshold
- PTO, pain tolerance
Cryotherapy has been accepted for decades as an effective, inexpensive and simple intervention for pain management after many acute sport injuries.1,2 It is widely believed that the therapeutic application of cryotherapy leads to a reduction in pain and swelling, but the physiological basis for this effect is still incompletely understood.3,4 Saeki5 and other authors concluded that pain relief with cold application could be due to many mechanisms including altered nerve conduction velocity (NCV), inhibition of nociceptors, a reduction in muscle spasms and/or a reduction in metabolic enzyme activity levels.6–8
NCV can be altered by gender, age and, more pertinently, skin temperature.9 On this basis it is plausible to propose that cryotherapy could reduce pain via an alteration in NCV. Alternatively, cryotherapy could also be effective as a counterirritant to pain via diffused noxious inhibitory controls, pain gate theory, suppressed nociceptive receptor sensitivity or via the analgesic descending pathway of the central nervous system such as endorphins.1,5,10,11 Evaluation of a counterirritant role is difficult to directly evaluate, but if cryotherapy can reduce pain threshold (PTH) and pain tolerance (PTO) independent of any effect on NCV then these processes may be more important.
The aim of the current study, therefore, was to assess changes in NCV, PTH and PTO concomitantly as ankle skin temperature was reduced via cryotherapy. We hypothesise that cryotherapy reduces skin temperature to a level that decreases NCV, and that changes in NCV, are associated with an increase in PTH and PTO.
METHODS
Subjects
A convenience sample of 23 volunteers from local sports clubs were informed individually about the purpose, nature and risks involved with the study. Written informed consent was obtained, and ethical approval was granted through the Manchester Metropolitan University, Manchester, UK. The study conformed to the Declaration of Helsinki. Inclusion criteria required the subjects to be young (20–29 years), male and physically active. Exclusion criteria prevented the recruitment of subjects who were having/had central and/or peripheral nervous system disorders, overweight (body mass index >30), skin problems and/or allergic response on to exposure cold conditions.
Research design
All subjects were fully familiarised before to testing, at which time the experimental (EXP; cryotherapy) and control (CON) ankles were determined randomly by the toss of a coin. All data collection occurred in one visit to the laboratory (ca 3 h) where the room temperature was held constant between 21°C and 24°C. Both ankles were subjected to the same measurement protocols at the same time, but the order of testing between EXP and CON ankle was again randomised by the toss of a coin. For the EXP ankle this meant measures of NCV, PTH and PTO at baseline before ice application and then at skin temperatures of 15°C and 10°C with ice cooling and a skin temperature of 15°C with re-warming after ice removal. Chesterton et al12 reported that to achieve a desirable physiological response (reduction in pain) with cryotherapy requires that the skin tissue is cooled to specific temperature levels (<13.2°C). This specifically drove the rationale for the choice of temperatures assessed in this research design.
Protocols
Skin temperature was measured using a Digital Thermometer (Chavin Arnoux, France). An electrode was placed on the iced area of leg where NCV, PTH and PTO were measured. The thermistor was applied directly to the skin so temperature measures reflected skin changes with heat loss rather than the direct effect of ice on the thermometer.
In this study, NCV measurement was acquired by using a portable electromyogram (EMG) system (Medtronic Keypoint, Copenhagen, Denmark). Anode and cathode electrodes were fixed to the fifth toe and the two EMG electrodes were placed over the tibial nerve. Proper placement of the EMG head would result in the contraction of muscles of the fifth metatarsal once stimulated. The active electrode was placed above the flexor retinaculum and medial to the medial malleolus for both medial and lateral plantar nerves. The ground electrode was placed on the dorsum of the foot. The stimulus intensity needed to obtain the maximal amplitudes is usually three times the sensory threshold. Lateral plantar stimulation was applied orthodromically by means of a ring electrode on the fifth toe. The EMG was set to a frequency of 8 Hz or 1.6 kHz with a sweep speed of 2 or 5 ms/div and a gain of 5–10 μV. NCV was then calculated by software inherent to the EMG as the time difference between the stimulation and the stimulation and onset of EMG activity divided by the distance (assessed by callipers) between the fifth-digit ring electrodes to the ankle pick-up.
Both PTH and PTO were assessed by a pressure algometer (Pain Diagnostic and Thermography, Great Neck, NY, USA) by a single investigator at two different sites of reference for the tibial nerve on the lateral aspect of both the treatment and control ankles. The first assessment site (PTH1, PTO1: iced) was located posterior to the lateral aspect of the lateral malleolus 1 cm to the lower tip of the lateral malleolus, where ice application and skin temperature measurements were made. The second assessment site (PTH2, PTO2: non-iced) was located on the lateral aspect of the shaft of the fourth metatarsal bone in close proximity to its head, distal to the first point. This was not iced but still served by the tibial nerve. The algometer has a force gauge (0–20 kg) fitted with a rubber tip with a 1 cm2 surface area13–15 that was mounted on a stand vertically above each of the two ankles. A lever arm on the stand allowed the circular probe head of the algometer to be lowered gradually to make initial contact with the skin and once in place, the probe head was further lowered at a steady rate until discomfort was reported (PTH) and removed at the point the pain became unbearable (PTO).
Ice application
After baseline measures, ice was applied to lower the tissue temperature on the EXP ankle. Crushed ice has been found to be most effective in reducing skin temperature compared with other cold modalities,12,16 and was hence used in this study. At the specific skin temperatures noted (15°C and 10°C), the ice pack was removed and all variables were reassessed.
Data analysis
Descriptive statistics (mean (SD)) were used to summarise the data for NCV, as well as for PTO and PTH, at both assessment sites on the EXP and CON ankles. Data for NCV, PTO and PTH at both iced and non-iced sites were analysed using repeated-measure two-way analysis of variances (ANOVAs) with the timeline (pre (baseline), 15°C, 10°C and 15°C) and ankle (EXP and CON) as repeated factors. For each significant F ratio, post hoc comparisons of group means were made using the Tukey honestly significant difference test. Pearson product–moment correlations were then performed on the association between changes (delta scores from baseline to 10°C) in NCV with PTO and PTH. For all statistical tests, differences were considered to be significant if p<0.05. Data analysis was performed using the SPSS V.10 software package.
RESULTS
Nerve conduction velocity
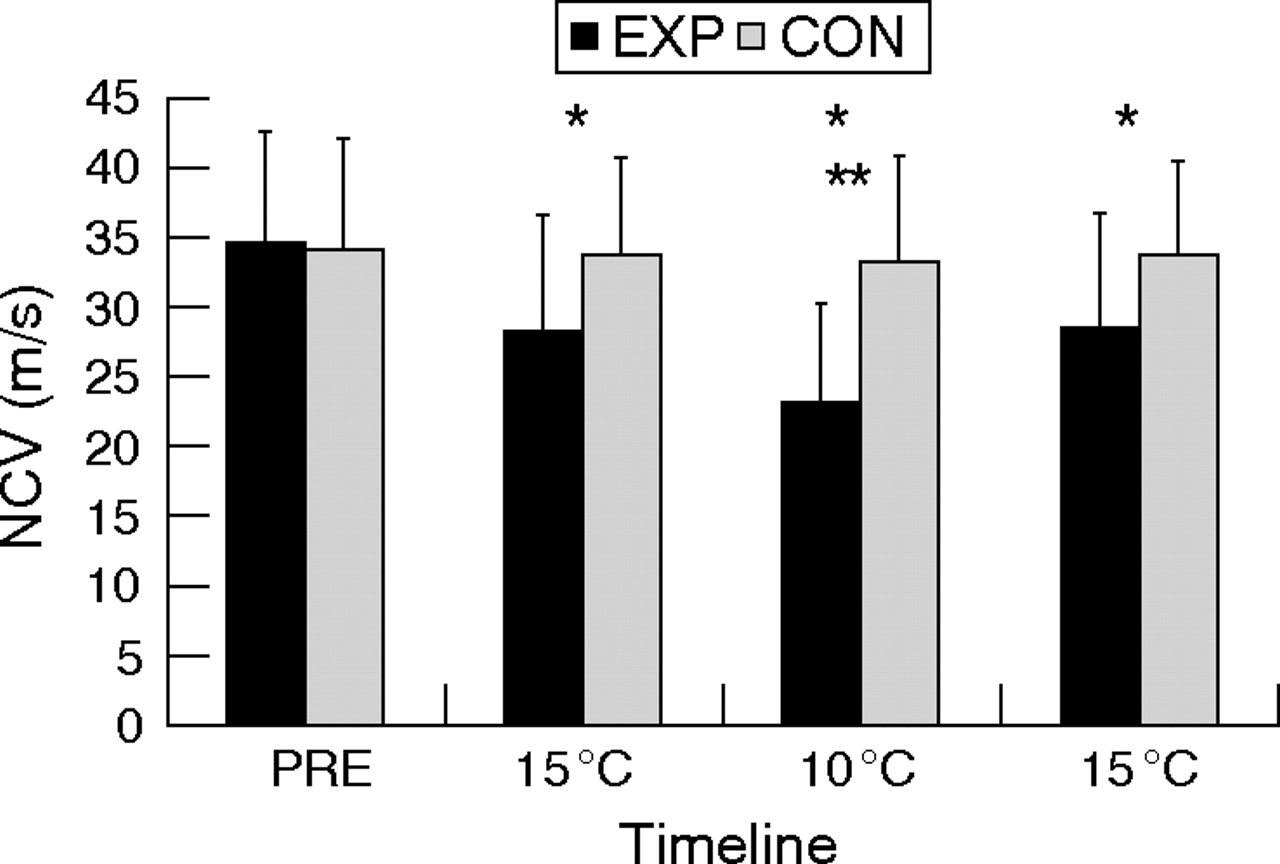
The average ice application time for skin temperature to reach 10°C was 26 min (range 20–31 min). For NCV, significant main effects for ankle (EXP vs CON: F = 5.4, p = 0.02) and timeline (pre, 15°C, 10°C and 15°C: F = 31.8, p<0.005), as well as the ankle–timeline interaction, (F = 27.8, p<0.005) were demonstrated. Figure 1 presents the pattern of response, and post hoc analysis stated that NCV for the EXP ankle was significantly depressed from baseline as ankle skin temperature decreased in a progressive fashion. At both 15°C and 10°C NCV was also significantly lower in the EXP ankle than in the CON ankle (p<0.05). Data for NCV did not differ across the timeline in the CON ankle (p>0.05; fig 1). The change in NCV with ice application from baseline (pre) to 10°C represented a 33% reduction.
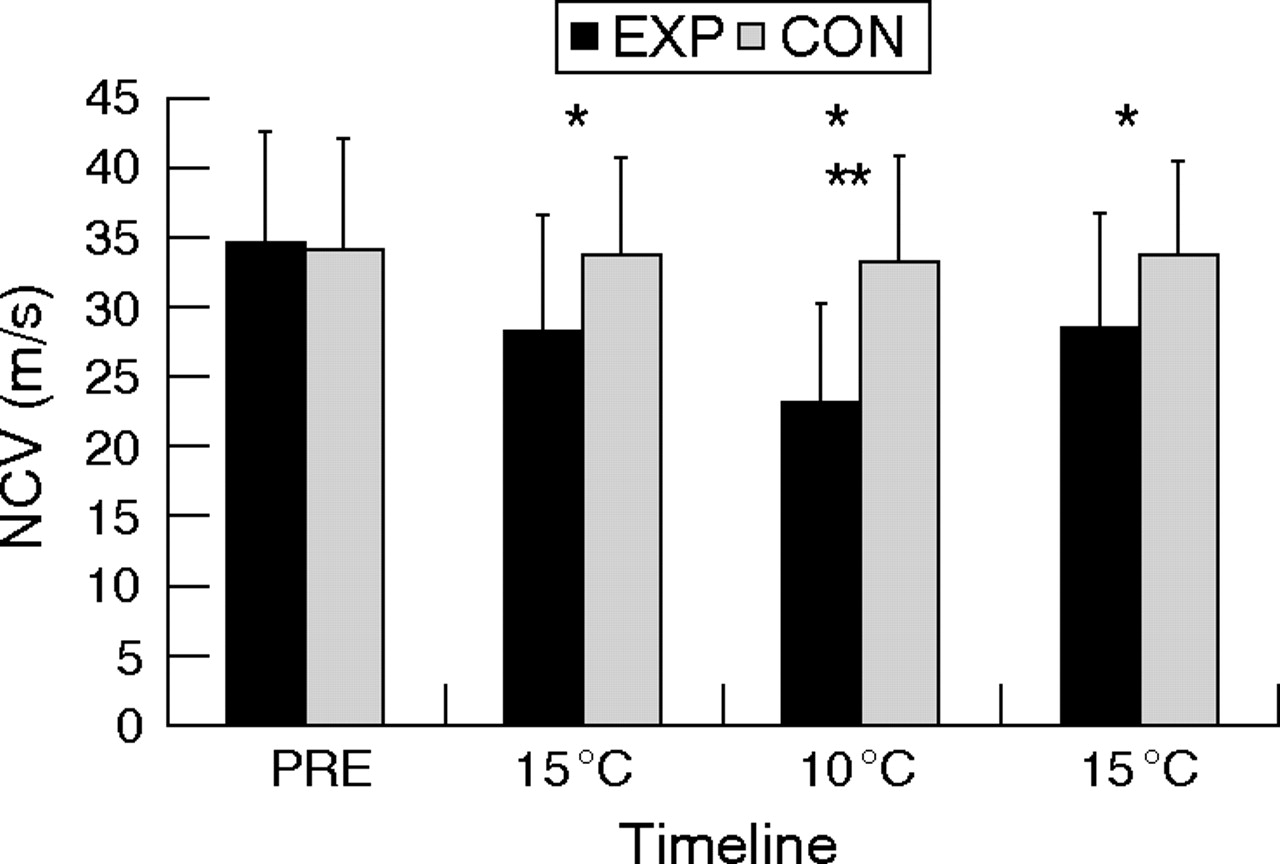
The impact of ice application on nerve conduction velocity in experimental (EXP) and control (CON) ankles (data are mean (SD)). Timeline: pre, baseline; 15°C, skin temperature cooling; 10°C, skin temperature cooling; 15°C, skin temperature with passive warming. *Significant difference between EXP and CON ankles as well as between pre and 10/15°C measurements in EXP ankle (p<0.05). **Significant difference between 15 and 10°C measurements in the EXP ankle (p<0.05).
PTH and PTO at assessment site one (iced)
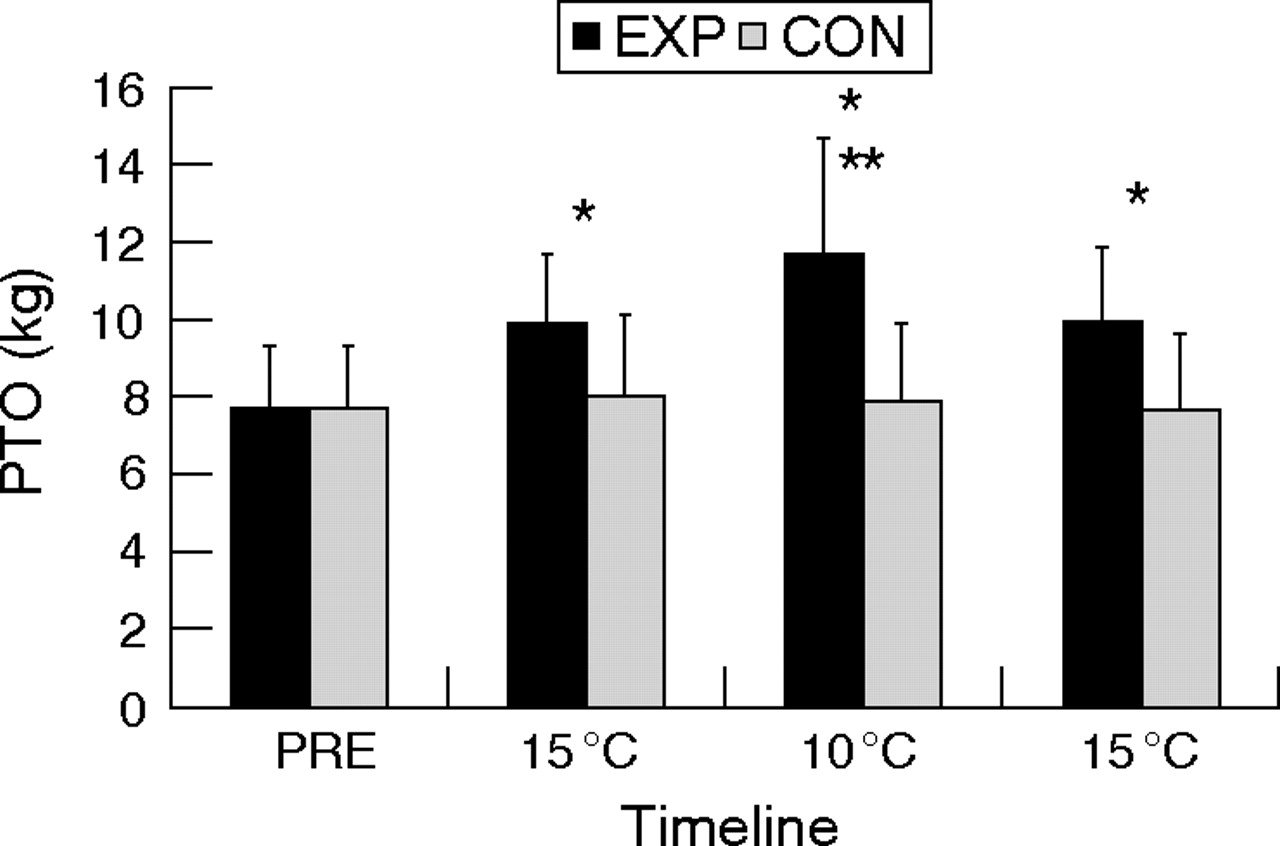
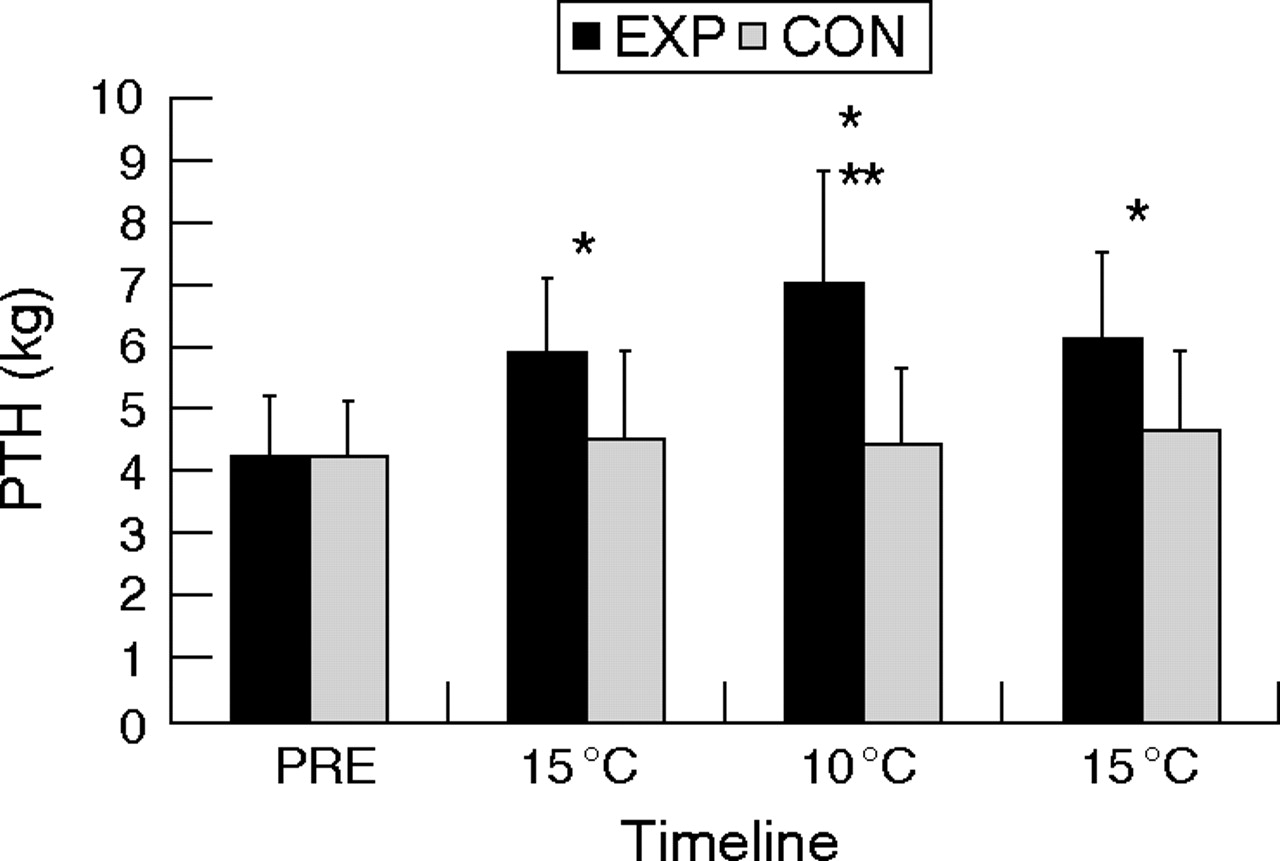
Both PTH1 and PTO1 were significantly altered by ice application (figs 2 and 3). For PTH1, significant ANOVA F ratios were reported for the main effects of ankle (F = 47.5, p<0.005), timeline (F = 56.7, p<0.005) and their interaction (F = 41.3, p<0.005). This was mirrored by statistical outcomes for PTO1 (ankle: F = 34.5, p<0.005; timeline: F = 53.2, p<0.005; interaction: F = 43.2, p<0.005). Data for both PTH1 and PTO1 represent a significant and progressive increase in threshold and tolerance for pain perception, with a decrease in skin temperature. In both cases, these changes in the EXP ankle were significantly different from the CON ankle, which remained unchanged across the timeline of repeat assessments. The relative percentage change in PTH1 from baseline (pre) to 10°C was 89% in the EXP ankle. Likewise, the relative percentage change in PTO1 from baseline (pre) to 10°C was 76% in the EXP ankle.

The impact of ice application upon pain threshold (PTH) at point 1 (iced) in the experimental (EXP) and control (CON) ankles (data are represented as mean (SD)). PTO, pain tolerance. *Significant difference between EXP and CON ankles as well as between baseline (pre) and 10/15°C measurements in the EXP ankle (p<0.05). **Significant difference between 15 and 10°C measurements in the EXP ankle (p<0.05).

The impact of ice application on pain tolerance at point 1 (iced) in the experimental (EXP) and control (CON) ankles (data are represented as mean (SD)). PTH, pain threshold. *Significant difference between EXP and CON ankles as well as between baseline (pre) and 10/15°C measurements in the EXP ankle (p<0.05). **Significant difference between 15 and 10°C measurements in the EXP ankle (p<0.05).
PTH and PTO at assessment site 2 (non-iced)
Both PTH2 and PTO2 were significantly altered by ice application (figs 4 and 5). For PTH2, significant ANOVA F ratios were reported for the main effects of ankle (F = 19.1, p<0.005), timeline (F = 46.5, p<0.005) and their interaction (F = 30.0, p<0.005). This was mirrored by statistical outcomes for PTO2 (ankle: F = 14.4, p<0.005; timeline: F = 35.6, p<0.005; interaction: F = 21.7, p<0.005). Data for both PTH2 and PTO2 represent a significant and progressive increase in threshold and tolerance for pain perception, with a decrease in skin temperature. In both cases, these changes in the EXP ankle were significantly different from the CON ankle, which remained unchanged across the timeline of repeat assessments. The relative percentage change in PTH2 from baseline (pre) to 10°C was 71% in the EXP ankle. Likewise, the relative percentage change in PTO2 from baseline (pre) to 10°C was 56% in the EXP ankle.

The impact of ice application on pain threshold (PTH) at point 2 (non-iced) in the experimental (EXP) and control (CON) ankles (data are represented as mean (SD)). *Significant difference between EXP and CON ankles as well as between baseline (pre) and 10/15°C measurements in the EXP ankle (p<0.05). **Significant difference between 15 and 10°C measurements in the EXP ankle (p<0.05).
The impact of ice application on pain tolerance (PTO) at point 2 (non-iced) in the experimental (EXP) and control (CON) ankles (data are represented as mean (SD)). *Significant difference between EXP and CON ankles as well as between baseline (pre) and 10/15°C measurements in the EXP ankle (p<0.05). **Significant difference between 15 and 10°C measurements in the EXP ankle (p<0.05).
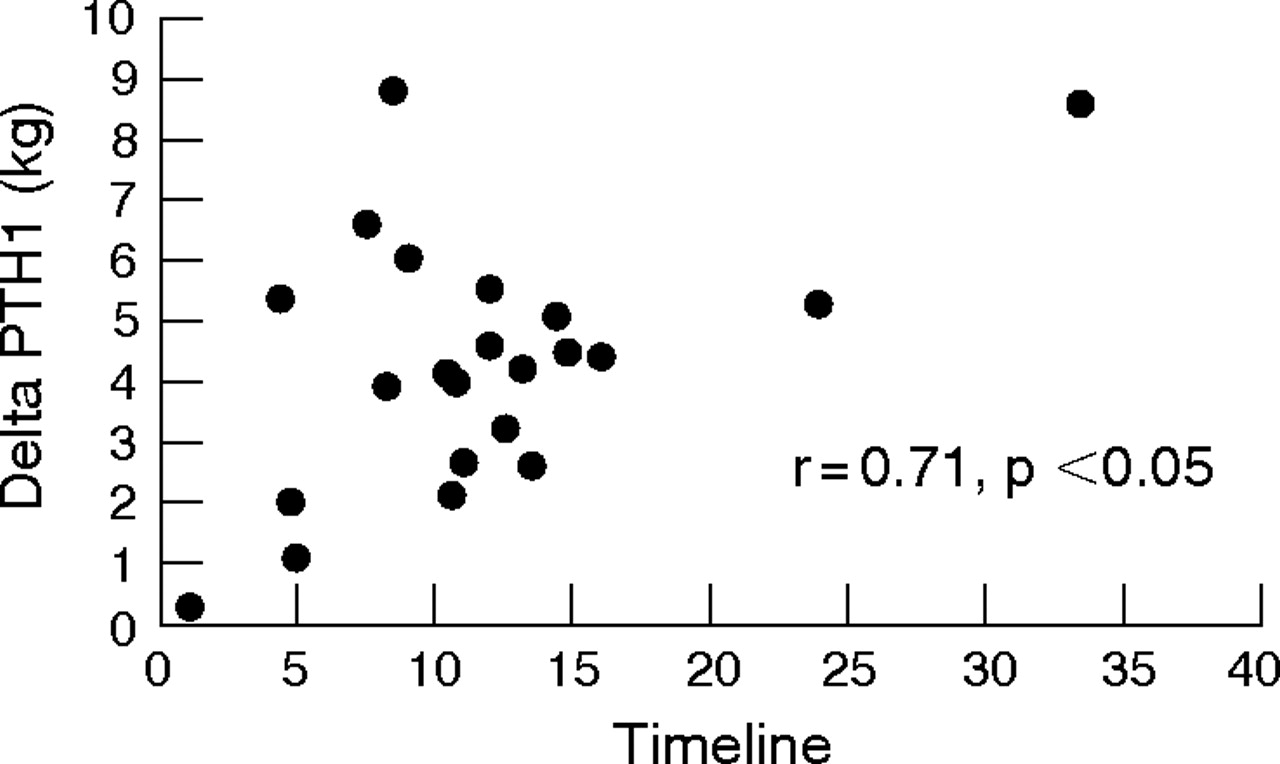
Delta scores for NCV, PTH and PTO from baseline (pre) to 10°C were correlated and all relationships were significant (NCV and PTO2 = 0.41, NCV and PTO1 = 0.55, NCV and PTH2 = 0.68, NCV and PTH1 = 0.71, all p<0.05). Figure 6 presents an exemplar scatterplot for the relationship between the change in NCV and PTH1 (r = 0.71). These data suggest a close association between the ice-induced alteration in NCV and the consequent changes in PTH and PTO irrespective of site assessed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The relationship between changes from baseline (pre) to 10°C in nerve conduction velocity and pain threshold (PTH) at assessment point 1 (iced).
DISCUSSION
Our data support the contention that cryotherapy is an effective, inexpensive and simple intervention for pain management,1,2 and uniquely provides some insight into the potential mechanisms by which this may be brought about. Specifically, NCV is significantly and progressively reduced concomitantly with skin temperature at the ankle during cryotherapy. Associated with the changes in NCV, we observed significant increases in PTH and PTO at both assessment sites on the ankle served by the same nerve, even though only the first site received direct ice application.
We reported an average reduction of 33% in NCV from baseline (pre) to 10°C, which equates to a 0.4 m/s decrease in sensory NVC for each 1°C fall in skin temperature (ca 31–10°C). This trend supports previous data.17 A drop in NCV with a reduction in skin temperature was also reported by Chesterton et al,12 although the magnitude of relative change in NCV was smaller than that observed in the current study. Specifically, Chesterton et al12 reported that a skin temperature of 13.5°C was required to reduce NCV by 10% compared with the 17% reduction in NCV at 15°C and the 33% reduction in NCV reduction at 10°C in the present study. The difference in magnitude of these changes may be due to a number of methodological differences between the studies, notably the site of the acquired temperature measurements.
Any specific explanation of the decrease in NCV with cryotherapy in the current study is purely speculative. However, previous research has suggested that temperature can affect the exchange between Ca2+ and Na+ in neural cells.17 Reid et al reported that low temperature could increase the friction between Ca2+ and its cellular “gate” during the exchange that could result in the delay of action potential generation.
Associated with the drop in NCV was an increase in PTH and PTO at both assessment sites. As with the changes in NCV, the significant increases in PTH and PTO were progressive with the decrease in skin temperature recorded at assessment site 1. Previous studies have documented an increase in both PTH and PTO with the use of cooling.5 The fact that PTH and PTO were increased in a similar manner at both assessment site 1 (iced) and site 2 (non-iced) as well as the fact that PTH and PTO were significantly different between the EXP and CON ankles, may provide some mechanistic insight into the change in pain perception with ice application. Interestingly, some investigators have reported that with exposure to a cold environment (19°C) for 30 min, plasma β-endorphin levels doubled.18,19 In this case, β-endorphin should affect the organism as a whole and increase PTH and PTO throughout the body. In the EXP and CON ankles different PTH and PTO responses were noted, suggesting no general β-endorphin effect. Although we did not assess β-endorphin levels in this study, it does not seem to be a plausible theory. For a similar reason, the role of any higher nervous system activity in explaining the current data can also be largely discounted.
The diffuse noxious inhibitory control theory, the pain gate theory and the theory of suppression of nociceptive receptor sensitivity can be largely discounted as these would predict a different PTH and PTO response at the two assessment sites (iced and non-iced). The diffuse noxious inhibitory control theory suggests that responses to noxious stimuli applied in the excitatory receptive field are inhibited by other noxious stimuli applied to parts of the body distant from the excitatory receptive field. Assessment site 2 was distal to the ice application, but PTH and PTO responded similarly to changes seen at site 1. In the pain gate theory, pain pulses transmitted by A δ fibres and C fibres are inhibited by various inputs conducted by A δ to dorsal horn cells, leading to the regulation of pain perception by a gate that may be opened or closed.20 In the present study, assessment sites 1 and 2 would have their own neural pathways or gates (spinal cord level). When site 1 was iced, on the basis of the pain gate control theory, the pain signals from the iced site should be blocked at the spinal cord level but not at the non-iced site. This does not coincide with the data obtained for PTO and PTH at both sites.
Changes in PTO and PTH at both assessment sites could, therefore, plausibly be explained by the reduction in NCV of the tibial nerve. At the site on the treatment ankle that was not iced a decrease in NCV was still apparent, as were changes in PTO and PTH, even though no local cooling had taken place. This viewpoint is indirectly supported by the work of Walmesley et al,21 who reported that the application of transcutaneous nerve stimulation to relieve pain was associated with a significant reduction in median NCV.
As with any study, it is pertinent to note some limitations and suggest future research to address these and other issues. The current study used cooling during a completely non-active timeline and thus the generalisability of the influence of ice application on pain perception within a sporting context may be limited. Indeed, not all sports-injury related cryotherapy can be applied for the same time period. In these circumstances, skin cooling may be interspersed with periods of muscle activity producing localised heating. Such interactions may be worthy of further research. Future studies may examine the responses of different sensory fibres to cooling. It is pertinent to note that the tibial nerve is superficially located and, as such, the use of cryotherapy at other sites/injuries would probably lead to a different relationship between skin temperature change and an alteration in NCV. This would result in different skin temperature changes and thus mediate a range of responses in NCV.
What is already known on this topic
-
Cryotherapy is routinely used in the frontline treatment of a large number of sports injuries, although its mechanism of action is unclear.
What this study adds
-
We have shown that in a specific model of ankle cooling the association between changes in pain sensation and nerve conduction velocity (NCV) suggests a role for NCV in mediating the clinical impact of cryotherapy.
In conclusion, the present study revealed that ice application to the ankle resulted in an increase in PTH and PTO at the point of ice application as well as at an assessment site distal to the ice application but also served by the tibial nerve. A significant decrease in NCV was also observed with a decrease in ankle skin temperature. It is, therefore, plausible in the current study to suggest that cryotherapy at the ankle exerts its clinical effect, a reduction in pain, primarily via altered NCV in the tibial nerve.
REFERENCES
Commentary
Cryotherapy is often used in the treatment of sports injuries. The paper presented demonstrates that the mode of action of cryotherapy is likely to be related to the diminishing of nerve conductance velocity. This findi]ng is of great significance to those treating soft-tissue injuries and may also influence decisions relating to return to play after the use of this treatment modality.
Footnotes
-
Published Online First 15 January 2007
-
Competing interests: None.
-
This work was completed while Amin A Algafly was studying for an MSc in Sports Injury and Therapy at Manchester Metropolitan University.