Article Text

Abstract
Objective: To create a basis for prevention of modern skydiving injuries.
Design: Descriptive epidemiological study.
Setting: National total material.
Patients: Data on all reported injury events (n = 257) in Swedish skydiving 1999–2003 (total 539 885 jumps) were retrieved from the Swedish Parachute Association. Non-fatally injured skydivers were sent a questionnaire asking for event and injury details (response rate 89%), and supplementary hospital records were retrieved for the most serious injuries (n = 85). Human, equipment and environmental factors were assessed for risk.
Main Outcome Measurements: Frequency and severity of injuries.
Results: Incidence of non-fatal injury events was 48 per 100 000 jumps. The lower extremities, spine and shoulders were important regions of injury. The most serious injuries were experienced by licensed skydivers, but students in training had a higher injury rate and more often left the sport because of the injury. Of two student-training systems, one had an incidence less than half that of the other.
Conclusions: A basis for prevention was created, showing a potential for reduction of frequency and severity of injuries with training and technical interventions.
- AFF, accelerated free fall
- AIS, Abbreviated Injury Scale
- MAIS, maximum AIS
- SFF, Svenska Fallskärmsförbundet
Statistics from Altmetric.com
- AFF, accelerated free fall
- AIS, Abbreviated Injury Scale
- MAIS, maximum AIS
- SFF, Svenska Fallskärmsförbundet
Skydiving, sport parachuting from aircraft, engages >675 000 participants in 118 countries1 and has been noted as an expression of the human capacity to challenge limitations.2 Previous studies on skydiving have become dated because of developments in technique and advancements in technology—for example, the transition from round parachutes to wing parachutes during the 1980s. During the 1990s, speeds in skydiving increased dramatically (fig 1). New free-fall events evolved with skydivers falling at faster rates, and faster wing parachutes popularised radical parachute flying, including the steeply diving “hookturn”, performed to gain airspeed (regularly >100 km/h) to fly the wing parachute level to the ground for a prolonged distance; current world record 206.85 m.3

The sport of skydiving: jumpers exit the aircraft (A) at an altitude of 1–4 km above ground level, and fall freely (B) approximately 1 min. Free fall through the atmosphere feels somewhat like submersion in rapidly flowing water, with velocity ranges between 110 and 500 km/h vertically and 0 and 140 km/h horizontally. Each skydiver carries two parachutes, integrated into a single harness. Should the main parachute malfunction, it is manually disconnected and the reserve used. All student skydivers in training and most licensed skydivers in Sweden carry an automatic activation device that deploys the reserve at a preset altitude and vertical velocity, if the skydiver has lost altitude awareness or become incapacitated. Parachute deployment is initiated by releasing a small round parachute, called a pilot chute (C), that anchors into the airstream and pulls out the wing parachute. The main parachute is deployed usually at approximately 1 km above ground level. The wing parachute is subsequently piloted to a designated landing area called a drop zone. The transient wing parachute velocity ranges between 0 and 190 km/h vertically and 0 and 140 km/h horizontally. Wing parachute of an experienced skydiver (D) and of a student (E). (F) Shows forward landing speed by trace in snow. Photos courtesy of Hans Berggren and Marcus Runsten. Informed consent was obtained for publication of the photos.
Barrows et al4 investigated injuries treated at first-aid stations at skydiving conventions in the US between 2000 and 2001. They found a total injury rate of 170 per 100 000 jumps and a hospital admission rate of 18 per 100 000 jumps, and noted that comparative analysis of previous skydiving injury studies is confounded by discrepancies in methods. In Denmark, between 1979 and 1983, 140 per 100 000 jumps resulted in injuries requiring medical treatment,5 and a similar injury rate was reported in The Netherlands between 1981 and 1985.6 From Great Britain, injury rates of 120–360 per 100 000 jumps have been reported, with the risk of injury being up to 12 times higher for novices than for those having jumped at least once before.7–9 Several studies have investigated military parachuting,10–22 but armed forces parachuting differs from skydiving in important aspects such as demography, training, environmental conditions for jumping and parachute flight characteristics. Thus, no available literature on civilian or armed forces parachuting is suited to form a basis for prevention of modern skydiving injuries.
Of a total of 5.77 million sport jumps made worldwide during 2002, Sweden was the seventh largest country in number of sport jumps.23 Skydiving clubs in Sweden use two different training systems for students. The most common, henceforth called “conventional” systems (including subtypes static-line and instructor-assisted deployment), uses automatic immediate parachute deployment on exit of the aircraft during the first jumps. As the student develops proper skills, manual deployment and prolonged free falls are cautiously introduced. The conventional course is 24 levels (before a 2003 curriculum revision, it was 25 levels), usually completed in around 30 jumps. The other training system, called accelerated free fall (AFF), puts the student into a long free fall at the first jump itself, with two instructors alongside in free fall to instruct and assist. The AFF course comprises 10 levels. With both training systems, the student flies and lands the wing parachute unaided from the first jump. Tandem skydiving as an introductory experience to the sport is common in Sweden, but is not used in student training itself.
This study aimed to describe the epidemiology of non-fatal injuries in Swedish skydiving between 1999 and 2003, to create a basis for injury prevention.
MATERIALS
All skydiving events in Sweden between 1999 and 2003 took place in clubs affiliated to the Swedish Parachute Association (Svenska Fallskärmsförbundet, SFF). Incident reporting to the SFF is compulsory. In conjunction with an incident, individual and environmental data are collected, as is information about the equipment used. The SFF is the body responsible for issuing skydiving licences of levels A (inexperienced) to D (expert), and maintains a member registry with demographic data, as well as jump volume data for Sweden (tables 1 and 2). From 1999 to 2003, the number of Swedish skydiving clubs decreased from 24 to 22. Monthly jump volumes could be obtained for the largest skydiving club (Stockholm Skydive Club) between 2001 and 2003. Discrete jump volume could only be obtained for A–D levels of license as a group, henceforth described as “licensed skydivers”, to be distinguished from “student skydivers”. Jump volumes were not available at the individual level.
Demography and reported non-fatal injury events (n = 257) in the Swedish Parachute Association during 1999–2003
Incidence rates of reported non-fatal skydiving injury events in Sweden during 1999–2003
Inclusion and exclusion criteria
All reported skydiving incidents resulting in injuries in Sweden between 1999 and 2003 were included (n = 257). Four fatal incidents were excluded and analysed as part of a separate fatality study.24 Tandem jumps, military parachuting, skydiving airplane crashes and parachuting incidents in other countries involving Swedish skydivers were also excluded. Sport parachuting from fixed objects (BASE jumping) is not regulated by the SFF, and consequently not a part of this study. Compulsory reporting to the SFF may have missed some minor injuries, but reporting of cases who sought medical consultation was believed to be satisfactory. The injury and liability insurance coverage granted to SFF members is a reporting incentive. The nationalities of skydivers in the total 257 incidents were 251 Swedish, 4 Norwegian and 2 Danish. Foreign skydivers jumping in Sweden were included in the total jump volume.
METHODS
Total material
Injury severity was categorised using the Abbreviated Injury Scale (AIS),25 with every separate injury (n = 311) assigned an AIS value 1–6. Every separate incident (n = 257) was categorised by the maximum AIS (MAIS) value sustained in it. Incidence rates for the whole period (1999–2003) were calculated by experience level and training system. Descriptive statistics were produced on the distribution by gender and experience level of number of incidents, age, number of jumps, severity and phase of jump when the injury occurred. Pearson’s χ2 test was used to test for gender differences in the relative frequency of injuries related to landing, as opposed to other phases of the jump, as well as wing loading (ratio of total suspended weight to wing platform area of parachute <1.3 vs ⩾1.4 lb/ft2) as determinant of parachute airspeed was related to severity of incident (MAIS 1+2 vs 3). The latter was investigated for landing incidents with licensed skydivers where weight of skydiver and size of parachute were known (n = 61). Statistical analyses were performed using STATA V.9.0.
Questionnaire
Skydivers included in the study were sent a questionnaire asking for injury details and permission to read medical records (table 3). Differences in age, gender, number of jumps and injury severity (MAIS category) between respondents and the total sample were tested for using Student’s t test (age and number of jumps) and Pearson’s χ2 test (gender and MAIS category). Local ethical committee approval was obtained (04-021 M).
Questionnaire sent to all living people who reported a skydiving incident with personal injury in Sweden during 1999–2003
RESULTS
Incidence rates, experience level and gender
The risk of an injury event of any kind was six times higher per jump for students than for licensed skydivers (table 2). Of the student incidents, 41%(44) occurred during the first two training jumps, and a majority of these (26) were miscalculations during wing parachute flight with fully operational equipment under normal environmental circumstances. AFF student training had an incidence rate less than half of the conventional student training (table 2). Two incidents with student skydivers in free fall were shoulder dislocations in the AFF training system, and in both cases, an instructor deployed the parachute for the incapacitated student. The other six AFF incidents were landing injuries.
Women were over-represented among injured skydivers, with an annual relative risk (RR) ranging between 1.4 and 2.7 during the years under study (table 1). Women also had a significantly higher proportion of landing injuries than men (RR 1.11 (range 1.01–1.23); table 4).
Gender and experience level (student–licensed) in reported non-fatal skydiving injury events in Sweden during 1999–2003 (n = 257), in relation to phase of jump when the injury occurred
Incident mechanisms, club and time of year
Miscalculations during wing parachute flight and turbulence were major risk factors, as were off-drop-zone landings (figs 2 and 3). The three largest clubs combined reported 48% of the total number of jumps during the time period, but their members reported only 27% of the injury events (fig 4). In Stockholm Skydive Club 2001–2003, the risk of injury was increased for the month of May, when skydiving activities resume after a 6-month winter break (fig 5).

Mechanisms in reported non-fatal skydiving injury events in Sweden 1999–2003 (n=257) in relation to phase of jump and experience level (student (Stud.) vs licensed (Lic.)). Miscalculations during “ordinary flight” included low turns, landings off headwind, and miscalculated horizontal levellings for landing, but excluded intentional low turns aimed at gaining landing airspeed (ie, “hookturns” referred to a separate group).
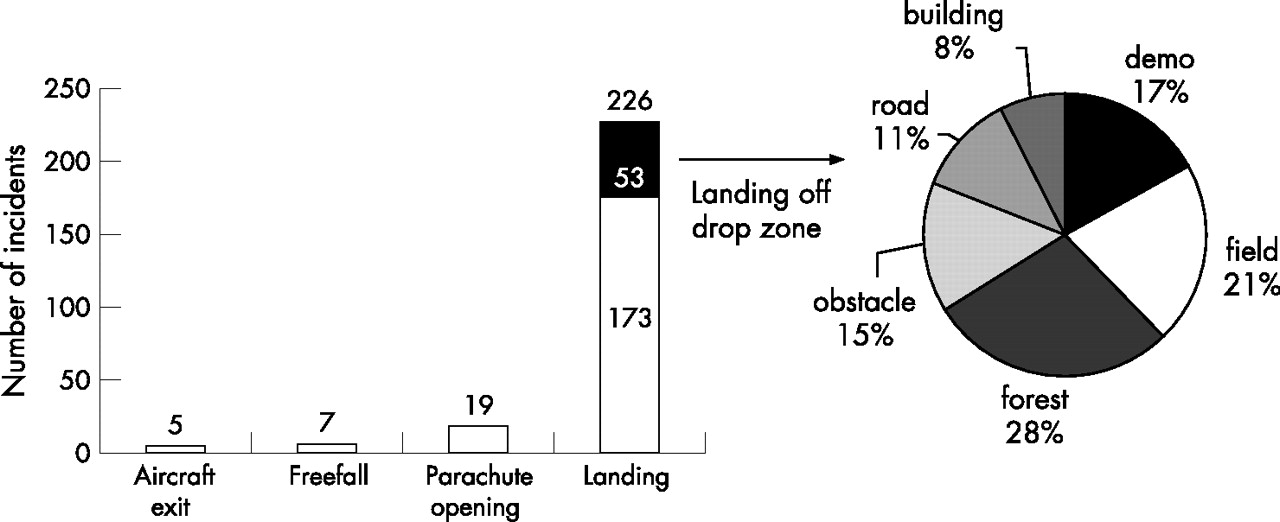
Reported non-fatal skydiving injury events in Sweden 1999–2003 (n=257) in relation to phase of jump when the injury occurred. Two hundred and sixteen of these landing injuries were categorised as a result of events during parachute flight (see fig 2). Pie chart shows 53 incidents related to landing outside regular skydiving drop zone. Of a total 94 landing incidents with student skydivers, 31% (29) were off drop zone. Demo, planned demonstration landing off drop zone (licensed skydivers only).

Reported jumps and injury events in 21 Swedish skydiving clubs 1999–2003 in relation to national total. Clubs sorted by jump volume.

Reported jumps and injury events per month in the Stockholm Skydive Club 2001–2003.
Equipment
Equipment-related incidents including reserve activations accounted for 42 of all 257 (16%) cases (table 2). Of the 150 licensed skydiver incidents, 11 involved use of the reserve parachute. Two were a result of hard main parachute openings, when the abrupt deceleration injured both skydiver (neck sprain and rib fractures, respectively) and main parachute, necessitating use of the reserve. The other nine experienced hard reserve landings. Number of jumps with the equipment used was known in 140 incidents for licensed skydivers with a median of 70 (range 1–2000) jumps. There was no significant association between wing loading and severity of landing incidents in this material.
Of the 107 student skydiver incidents, 15 involved use of the reserve parachute. Of these 15 injury events, three occurred during main parachute opening, with two hard openings and one entanglement where the main parachute twisted the knee of the skydiver. The other 12 experienced hard reserve landings. Reasons for student reserve use included four low main parachute activations with subsequent automatic reserve activations and one premature automatic reserve activation.
Anatomical location, severity and most serious incidents
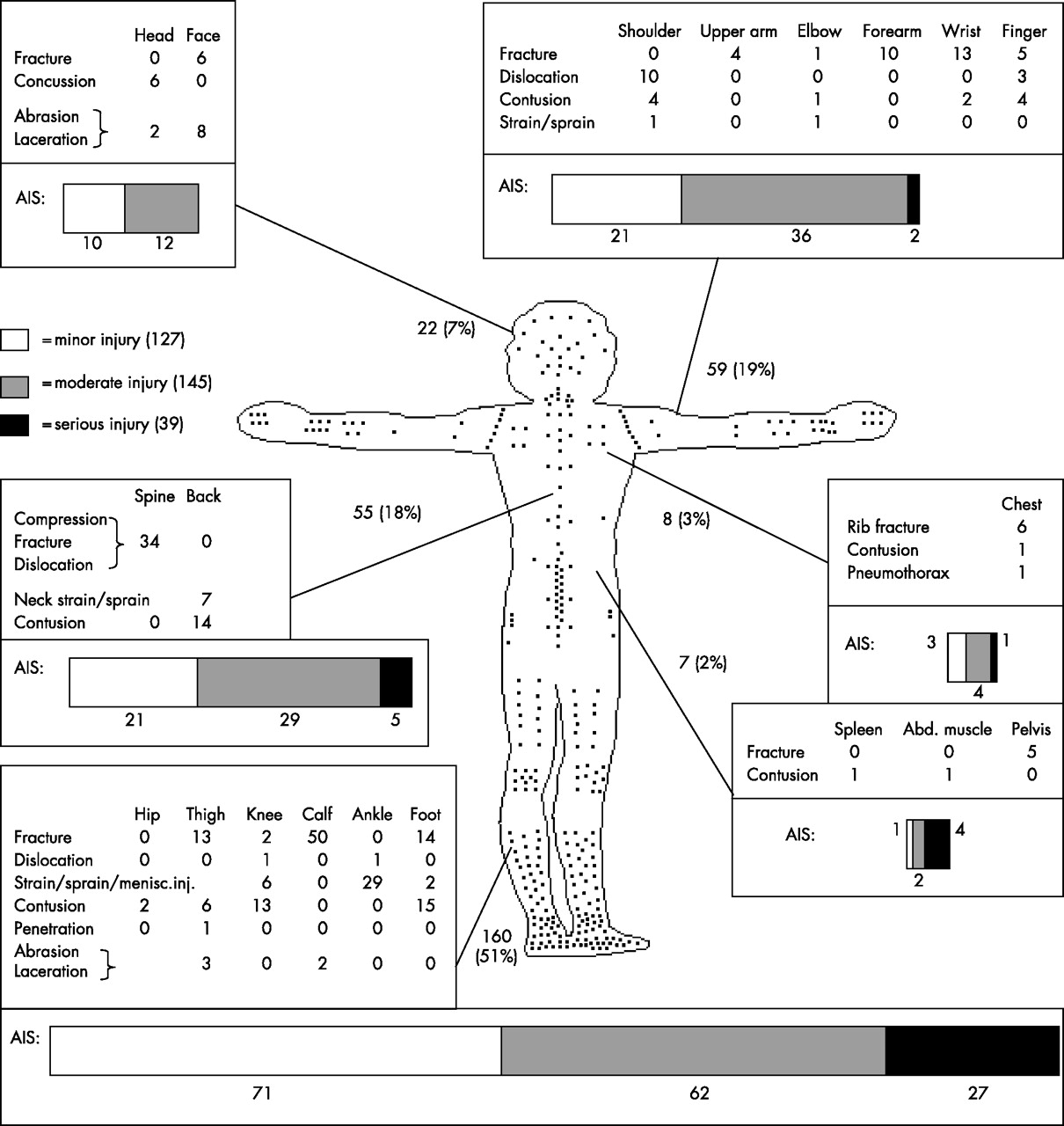
The lower extremities suffered 51% (160) of the total 311 injuries (fig 6). There were no injuries of severity AIS ⩾4. Severities of the total 257 incidents were 105 (41%) MAIS 1, 122 (47%) MAIS 2 and 30 (12%) MAIS 3 (table 5).
Gender, age, experience level and severity of incident in reported non-fatal skydiving injury events in Sweden during 1999–2003 (n = 257), reported serious incidents of maximum Abbreviated Injury Scale ⩾3 severity (n = 30) and questionnaire responses (n = 229)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The injured skydiver: distribution of injuries (n=311) sustained in reported non-fatal skydiving incidents in Sweden 1999–2003 (n=257), every dot representing an injury. Bar diagrams show injury severity categorised with the Abbreviated Injury Scale (AIS). All numbers are absolute except where stated as per cent of total. Anatomical outline from parachute inventor Leonardo da Vinci.31,3231 32 Abd, abdominal; menisc inj, meniscus injury.
The 30 MAIS 3 cases produced a total of 55 injuries (1 AIS 1, 15 AIS 2 and 39 AIS 3), of which 49 (89%) were fractures, mainly located to the lower leg (14), thigh (13), spine (5), pelvis (4) and foot (4). Of the 30 MAIS 3 incidents, six cases had ⩾2 injuries of AIS 3 severity. All except one case of a knee injury (complete disruption of the posterior and anterior cruciate ligament) had been admitted to hospital inpatient care (table 6). Of the 30 MAIS 3 incidents, 27 occurred at landing and 3 during parachute opening. Six of these landing incidents were off the drop zone, including three planned demonstration landings.
Healthcare consumption and impact on life in responses (n = 229) to a questionnaire sent to all living people having reported a skydiving injury event in Sweden during 1999–2003 (n = 257) (response rate 89% including serious incidents)
The MAIS 3 group showed a shift towards higher experience level. The median number of jumps was increased to six times that of the whole group, and 23 (77%) were licensed skydivers. The proportion of D-licensed (expert) skydivers was doubled from overall 67 (26%) to 15 (50%).
Five MAIS 3 incidents were miscalculated hookturns by licensed skydivers. Other MAIS 3 incidents experienced by licensed skydivers included miscalculated standard, straight-approach landings with fully operational parachute under normal environmental circumstances, miscalculated low turns performed without intent of gaining airspeed and turbulent air. Two MAIS 3 incidents with licensed skydivers occurred during parachute opening: one unstable parachute activation with the pilot chute line around the neck and one unintentional opening of the main parachute. Both cases involved relatively inexperienced skydivers (A-licensed) with few (2 and 12) jumps with the particular equipment used.
Two incidents of MAIS 3 severity were experienced by first-jump students, both sustaining lower leg fractures as a result of hard landings with operational wing (main and reserve, respectively) parachutes. Of the other five MAIS 3 incidents with student skydivers, two were miscalculated standard, straight-approach landings with fully operational parachutes under normal environmental circumstances, one had entangled an arm with the opening parachute and sustained an upper arm fracture, one landed in strong wind on a fence and one landed on grassy, uneven terrain.
Questionnaire responses
A total of 229 questionnaire responses were received, giving a response rate of 89% (table 5). The respondents did not differ significantly from the total group in age, gender, number of jumps and injury severity (MAIS category). Table 6 gives the results from questionnaire responses. On the basis of the Swedish Ministry of Health and Social Affairs assessment (Å Elffors, personal communication, 15 February 2006), healthcare costs in questionnaire responses exceeded 1 million euros.
Questionnaire non-responders
The median number of jumps by non-responders was lowered from 55 to 10 (range 1–1300). The student proportion increased and the proportion of D-licensed (expert) skydivers decreased. Gender and age were the same as for the total group. The proportion of MAIS 2 (moderate) incidents was increased and the proportion of MAIS 3 (serious) incidents decreased. The non-responder group contained five of the total six foreign skydiver cases.
DISCUSSION
Most injuries were caused by wing parachute pilot errors. A parachute (aerodynamic decelerator) slows down motion against air, whereas a wing slices through it with the ability to, given speed, deflect airstreams powerful enough to generate lift against gravity. When these two contrasting principles were synthesised into the wing parachute,26 it brought a paradigm shift to parachuting, promoting the parachutist from passenger to pilot. A correctly executed wing parachute landing is comfortable, but in contrast with the passive descent under a round canopy, a wing parachute must be actively flown. Prevention of these injuries requires training on wing parachute piloting, for both novices and experts.
The paratrooper boot has long been obsolete in skydiving. In Sweden, experienced skydivers may jump barefoot if they like. Students are advised to use shoes with lateral stability such as basketball shoes. Although military parachuting differs in many ways from sport parachuting, recent studies showing the effectiveness of outside-the-boot ankle braces10,20 merit a consideration of whether such protective gear could be of value also for civilians. Physical training and techniques to tolerate hard landings may reduce the number and severity of injuries. Such a landing technique exists: the parachute landing fall, distributing the forces of a hard landing through rolling. It has been part of parachuting for decades, but presently seems neglected.
It may be speculated whether some of the spinal injuries sustained during landing might have been prevented or moderated by use of protective equipment. Several spinal injuries were also sustained directly during parachute opening. Although the skydiver has some influence on opening shock with packing, body position and slowing down in free fall before deploying, part of the problem with injuries sustained during this phase of the jump seems technical. The relatively few head injuries may be an encouraging outcome of helmet requirements.
If miscalculated, the steeply diving hookturn manoeuvre will produce a high-speed glide path into the ground. This was a common mechanism for licensed skydivers and the cause of death of one Swedish skydiver in 2005. High-speed landing approaches can also create traffic disturbances. The chain of events that led to the most severe incident (pelvis fracture, bilateral femur and tibia fractures) was initiated by one skydiver hookturning into another before landing. High-speed landing approaches should receive recognition as advanced manoeuvres, and be separated from other parachute traffic. Definitions of the experience levels required to fly fast wing parachute models should include the ability to perform advanced manoeuvres with slower wing parachutes before upgrading. Work in this area has started in the SFF, and existing regulations regarding experience level and the use of fast-flying wing parachutes for licensed skydivers may have contributed to the present injury rate being the lowest described for skydiving.
The lower injury incidence for the AFF student training system seems favourable, but present data could not give any indications as to how AFF students fare as new license holders, when left alone with fewer training jumps than other skydiving alumni. As most students were injured at landing, when no AFF instructors were alongside to assist, the AFF advantage may lie in better teaching of wing parachute piloting. Free-fall tumbling leading to unstable parachute activation with subsequent line entanglement is a risk factor for a student’s death24 where AFF may offer protection. Both students who dislocated their shoulders in free fall were in acute danger, as reserve parachute emergency procedures require bilateral hand and arm function, and a non-functional arm can render an inexperienced skydiver unable to maintain a stable body position in free fall. The importance of shoulder stability in skydiving27 must be considered by medical doctors performing precourse examinations.
Efforts should be undertaken to minimise the risk for off-drop-zone landings. Half the total Swedish area is forest,28 and unintentional water landings have been a mechanism in skydiving deaths.24 It has been claimed that the wing parachute has eliminated the risk of future drownings, but the numerous present student off-drop-zone landing incidents do not support that view. Many Swedish clubs abandoned ground-to-student radio instruction during the 1990s, mainly because of poor technical quality. A radio reconsideration may be called for. Turbulent air collapsing or deforming the textile wing can be avoided by parachutists who are aware of this invisible enemy, and parachutes can be designed to minimise susceptibility to it.
What is already known on this topic
-
Skydiving has evolved in technique and technology.
-
Most previous studies of skydiving injuries have become dated.
What this study adds
-
Suggestions for the reduction of frequency and severity of modern skydiving injuries.
-
Healthcare consumption and impact on life estimates.
During 2002, the Swedish urban centre of Umeå (population 138 313) had 22% MAIS 2 and 2% MAIS 3 vehicle-related incidents,29 whereas Swedish skydiving during 1999–2003 had 47% MAIS 2 and 12% MAIS 3 incidents (including cases who never sought medical consultation). With a proportion of non-minor injuries more than double that of road traffic, it is imperative that injured skydivers receive fast and adequate care. One of the present cases had an obstructed airway and was saved by a skydiving friend.
A general instruction for students to activate the reserve on any uncertainty about main parachute integrity may have exaggerated the equipment-related incidence. In future studies on skydiving, it would be desirable to obtain license-level and gender-specific jump volumes. The larger landing injury proportion within the female group is intriguing. Some skydiving equipment in the early 1970s was unsuitable for women.30 Is there a modern gender pattern for skydiving injuries?
Acknowledgments
We thank Ann Lindberg, Ola Jameson, Arne Nilsson and Jesper Löfberg of the Swedish Parachute Association and Ann-Sofie Hjelm of Umeå University Hospital.
REFERENCES
Commentary
This study is the most comprehensive and clear assessment of the mechanisms of injury in sport parachuting to date. Owing to the impressive amount of data collected by the Swedish Parachute Association, the author is able to make a lucid depiction of the recent history in parachuting in Sweden that can be reasonably extrapolated to the global environment. The thorough analysis and clear arguments for specific areas of change make this a must-read for any parachuting instructor, safety adviser or government aviation agency representative.
Footnotes
-
Published Online First 15 January 2007
-
Funding: This study was funded by the Stenholm, Kempe and Cederberg research grants.
-
Competing interests: None declared.
-
Informed consent was obtained for publication of the photos.