Article Text

Abstract
Background: Conservative treatment of patellar tendinopathy has been minimally investigated. Effective validated treatment protocols are required.
Objectives: To investigate the immediate (12 weeks) and long term (12 months) efficacy of two eccentric exercise programmes for the treatment of patellar tendinopathy.
Methods: This was a prospective randomised controlled trial of 17 elite volleyball players with clinically diagnosed and imaging confirmed patellar tendinopathy. Participants were randomly assigned to one of two treatment groups: a decline group and a step group. The decline group were required to perform single leg squats on a 25° decline board, exercising into tendon pain and progressing their exercises with load. The step group performed single leg squats on a 10 cm step, exercising without tendon pain and progressing their exercises with speed then load. All participants completed a 12 week intervention programme during their preseason. Outcome measures used were the Victorian Institute of Sport Assessment (VISA) score for knee function and 100 mm visual analogue scale (VAS) for tendon pain with activity. Measures were taken throughout the intervention period and at 12 months.
Results: Both groups had improved significantly from baseline at 12 weeks and 12 months. Analysis of the likelihood of a 20 point improvement in VISA score at 12 months revealed a greater likelihood of clinical improvements in the decline group than the step group. VAS scores at 12 months did not differ between the groups.
Conclusions: Both exercise protocols improved pain and sporting function in volleyball players over 12 months. This study indicates that the decline squat protocol offers greater clinical gains during a rehabilitation programme for patellar tendinopathy in athletes who continue to train and play with pain.
- VAS, visual analogue scale
- VISA, Victorian Institute of Sport Assessment
- knee
- patellar tendon
- eccentric strengthening
- conservative treatment
- volleyball
Statistics from Altmetric.com
Patellar tendinopathy (jumper’s knee) occurs in several sports, with jumping athletes being the most susceptible.1 For example, the prevalence of jumper’s knee is 40–50% among elite volleyball players.2,3 This often recurrent condition can severely limit or even end an athletic career, and recovery from each episode can be prolonged.4 Importantly, the condition is not self limiting, and, although rest may offer symptomatic relief, pain often recurs on resumption of activity. Surgical options have provided limited success, with a retrospective study finding that only half of all athletes who had either open or arthroscopic patellar tenotomy were competing at their former sporting level at a four year follow up.5
Tendinopathy research to date has concentrated on the morphology and aetiology of this condition, with little focus on conservative treatment options. Although testing the efficacy of clinical intervention protocols does not identify the underlying pathomechanics, it does provide invaluable clinical information on the usefulness of these protocols.
Conservative treatment of patellar tendinopathy is empirically and clinically based, with progressive eccentric strengthening forming the cornerstone of most rehabilitation programmes. Despite this, there is little clinically relevant research on which to base an eccentric training programme, as there are few randomised controlled trials that have compared exercise based protocols for this condition.6,7 Although speed based eccentric exercise programmes proposed by Curwin and Stanish8 are in widespread use, the efficacy of these programmes for patellar tendinopathy has not been fully investigated.
The success of a pain based eccentric exercise programme has been demonstrated in the treatment of Achilles tendinopathy,9 but the effect of painful eccentric training during the rehabilitation of patellar tendinopathy is unknown. Furthermore, recent investigations have shown that squats performed on a 25° decline board target the knee extensor mechanism more specifically than the standard squat, and it has been suggested that this may be relevant in the management of patellar tendinopathy.10,11 Given these findings, a combination of squatting on a decline board and into tendon pain would theoretically provide an effective conservative treatment protocol for patellar tendinopathy.
The purpose of this study was to investigate the short and long term efficacy of two exercise programmes, one based on a traditional eccentric protocol (step group) and one based on more contemporary treatment options (decline group), for the treatment of patellar tendinopathy in volleyball players throughout a competitive season.
METHODS
This prospective randomised controlled trial used a parallel group, repeated measures design with an intervention period of 12 weeks and follow up at 12 months. Participants were recruited from the elite Victorian State League Volleyball (Australia) competition and clinically assessed (JC) on the last weekend of the regular season (2001). The La Trobe University Human Ethics Committee approved the project, and all participants provided written informed consent.
Participants had to be aged 18–35 years and present with proximal patellar tendon pain that limited sporting function. To be included, they had to have tendon pain on palpation, symptom reproduction on jumping, squatting, and/or stepping, absence of referred pain outside the tendon, a Victorian Institute of Sport Assessment (VISA) score less than 80 points, and an abnormal (hypoechoic) ultrasound. Participants were excluded if they had undergone any knee surgery in the preceding 12 months, patellar tendon surgery, corticosteroid injection into the tendon, or anterior cruciate ligament reconstruction (patellar tendon), presented with patellofemoral pain, or were receiving adjunct treatment for knee pain. Participants with bilateral knee pain were asked to select the most symptomatic knee for the purposes of the study.
Outcome measures
The primary outcome measure used was the VISA score, designed specifically to quantify knee function in athletes with patellar tendinopathy.12 Ranging from 0 to 100, the VISA score consists of eight questions assessing symptoms and simple tests of function and ability to play sport. A maximum score of 100 points represents full pain free function. Competing athletes with patellar tendinopathy commonly record a score of 50–80 points.4 The 100 mm visual analogue scale (VAS) was used as a secondary outcome measure for average tendon pain during weekly activity. Both measures have been shown to be valid and reliable.12–14
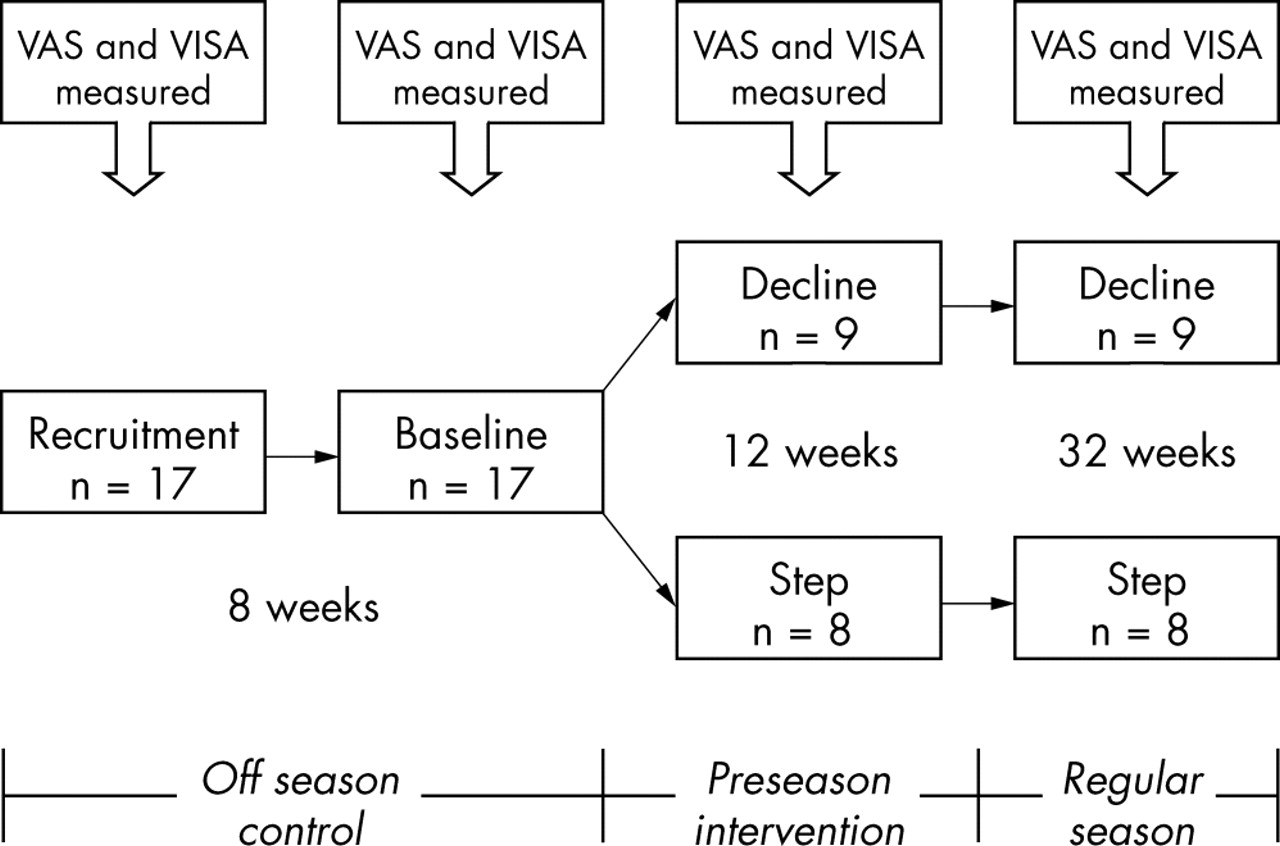
To assess the stability of initial scores, participants were assessed before and after an eight week control period between recruitment and baseline testing (fig 1). After baseline testing, participants assigned themselves to a group by randomly drawing from a batch of sealed, shuffled envelopes. VISA and VAS scores were recorded every four weeks during the intervention period and at 12 months. Investigators were blinded to all VAS and VISA measurements throughout the study. Participants were required to complete a daily training diary during the intervention period. This diary was used to monitor compliance, additional activity, and any drugs used.

Progress of participants through the season and timing of interventions. VAS, visual analogue score; VISA, Victorian Institute of Sport Assessment.
Intervention
Participants were required to complete their exercises twice a day for 12 weeks. Both groups completed three sets of 15 repetitions during a session. All exercises were completed on a single (affected) leg to about 60° of knee flexion, with participants being taught 60° of knee flexion during their initial session. Both groups progressed load by adding weight to a backpack in 5 kg increments.
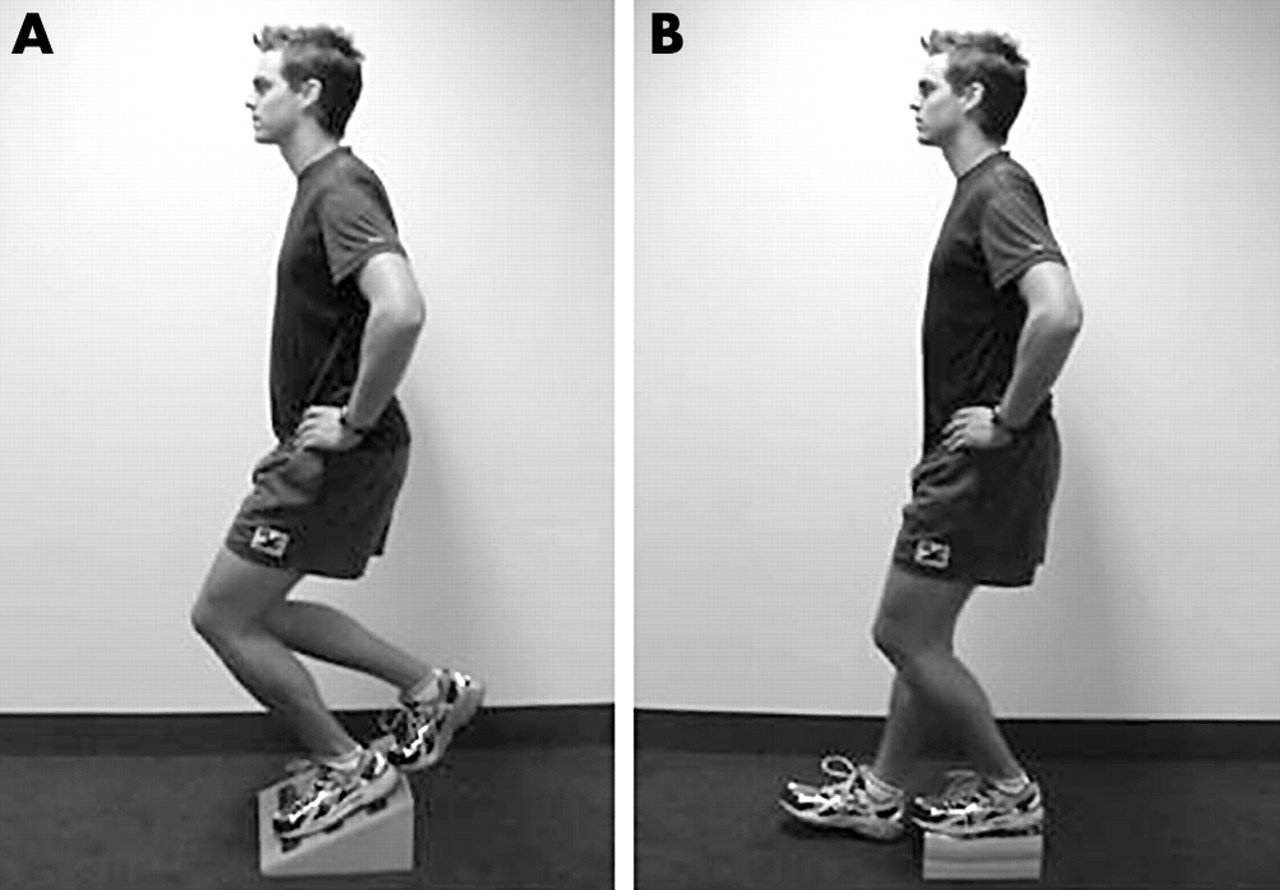
The decline group used a 25° decline board to perform their squats (fig 2A). They completed the downward component (eccentric phase) of the squat on the symptomatic leg, and the upward component (concentric phase) on the asymptomatic leg. They were instructed to exercise into moderate tendon pain and to progress by increasing load if this pain eased. Participants in the step group used a 10 cm step to perform their squats (fig 2B). They completed both components of the squat on the symptomatic leg. They were instructed to exercise with minimal tendon pain only and progress their speed from slow to fast, as outlined in the Curwin and Stanish protocol.8 When participants could complete their squats at a fast speed, they increased load.

(A) Decline squat. (B) Step squat.
Analysis
Paired t tests were used to assess baseline differences within groups. Between group VISA and VAS scores were compared using repeated measures two way analysis of variance for group and time interactions. Alpha significance was set at 0.05.
A more contemporary analysis15 was used to determine the likelihood of obtaining a clinically worthwhile outcome. The smallest clinically important change in VISA and VAS scores was set at 20 points for both outcomes, as a 20 point improvement was considered to reflect a significant change in functional capacity.12 Clinical significance was calculated by considering the probabilities that the effect was clinically positive (greater than 20 points), trivial (20 to −10 points), or negative (less than −10 points) for each participant. To provide ease of interpretation, VAS scores were inverted for this analysis so that an improvement was signalled by a positive change, as with the VISA scores.
RESULTS
All participants (13 men, 4 women) completed the 12 week intervention and 12 month follow up (fig 1). There were no differences between the groups for subject age (mean (SD) 27.3 (1.8) years) or weight (82.5 (11.5) kg). There was a significant (p = 0.01) difference in height between the groups (decline group 178.3 (8.3) cm; step group 191.4 (9.1) cm). This is probably because three women were randomised to the decline group and one to the step group. There was no difference between groups for exercise compliance, with a mean compliance of 72 (18)% of total possible sessions.
Statistical analysis revealed no change in outcome measures between or within groups over the eight week control period from recruitment to baseline testing (fig 3). Both groups had improved significantly (p<0.05) from baseline in both outcome measures at 12 weeks and 12 months, but there was no difference between groups for either outcome measure at any time.
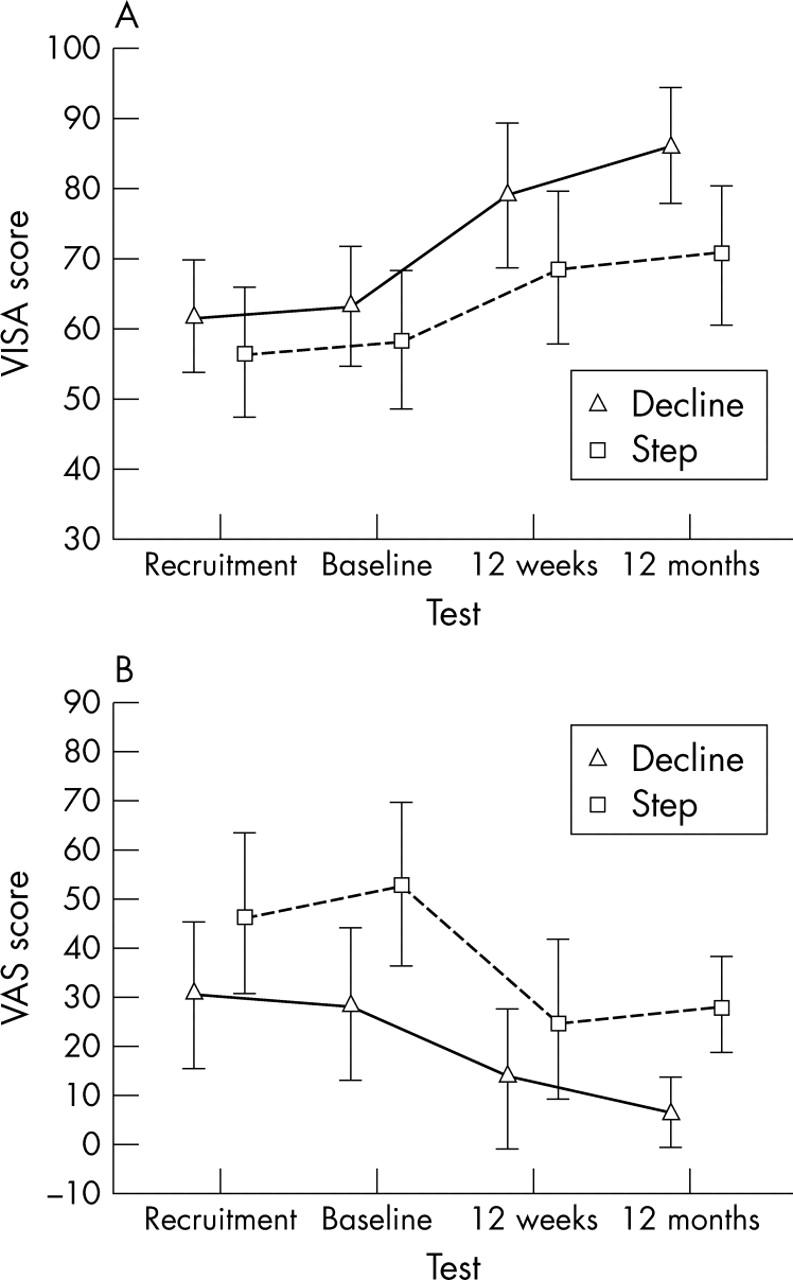
Mean (SD) change in (A) Victorian Institute of Sport Assessment (VISA) scores and (B) visual analogue scale (VAS) scores over 12 months.
Analysis of the likelihood of obtaining a clinical improvement in VISA scores at 12 weeks revealed no difference between groups. At 12 months, however, the decline group displayed a considerable difference in the likelihood of improvement in VISA scores (fig 4A). With the smallest practically important increase in VISA score set at 20 points, there was a 94% chance that the decline group would have a positive result at 12 months, compared with a 41% chance in the step group. Analysis of VAS score improvements revealed that the step group had an increased likelihood of reduced pain on VAS scores at 12 weeks compared with the decline group (fig 4B). There was no difference in improvement between the groups at 12 months.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Likelihood of clinical outcomes for (A) Victorian Institute of Sport Assessment (VISA) scores and (B) visual analogue scale (VAS) scores at 12 weeks and 12 months (mean change (95% confidence interval)). VAS scores are inverted so that an improvement is signalled by a positive change.
DISCUSSION
Both the decline and step protocols were effective in the treatment of tendon pain and sporting function in athletes with patellar tendinopathy. Clinicians can confidently use both conservative protocols investigated in this study to positively affect pain and, more importantly, the ability to play sport in jumping athletes. However, over a 12 month period, the decline protocol gave a considerably greater likelihood of a 20 point or more improvement in VISA score.
A major strength of this study is that we recruited athletes who continued to compete with continuing tendon pain at an elite level during the previous season. Previous tendinopathy research has recruited participants who have disabling tendon pain,9 often to the extent that they have ceased or considerably reduced sports participation and are awaiting surgery. Athletes who continue to train and play with moderate tendon pain comprise a large contingent of the population who suffer from patellar tendinopathy. Thus the results of this study are particularly applicable to clinical sports medicine practice. After the preseason intervention, the athletes were then tracked for a full 12 month season with no further intervention. By following this group through an entire competitive season, we were able to examine the long term efficacy of the interventions within a more practical scenario rather than a more artificial, short term period, which has been a limitation of previous studies.6,7
Although a non-exercising control group was not used in this study, the use of an eight week control period assessed the stability of the outcome measures before the intervention began. The VISA and VAS scores taken at recruitment were compared with scores taken at baseline testing, with no intervention being administered during this control period. There was no significant change in outcome measures between or within groups over the eight week control period, and this supports clinical experience that suggests rest alone will not alleviate patellar tendinopathy pain.
The step group had a greater likelihood of reduced pain on VAS scores at 12 weeks than the decline group. This outcome was expected, as the decline group were training into tendon pain whereas the step group were avoiding tendon pain. An initial increase in tendon pain is expected during any pain based eccentric programme,9 and this possibility was explained to the participants at the beginning of the study. To ensure this expected increase in tendon pain did not interfere with the ability to maintain participation throughout the competitive season, all interventions were completed in the preseason period. There was no difference between groups in VAS scores for average tendon pain at 12 months, and both groups completed the season with similar reductions in pain.
What is already known on this topic
There is little clinically relevant research on which to base a conservative rehabilitation programme for patellar tendinopathy.
What this study adds
Clinicians can confidently use the decline squat protocol investigated in this study to positively affect pain and, more importantly, the ability to play sport in jumping athletes.
The purpose of this study was to compare contemporary treatment options (decline protocol) with a traditional eccentric programme (step protocol). Our ability to specify which component of the protocols was responsible for differences in improvement between treatment groups is limited because there was more than one variable between groups in this study design. Differences between groups were: squatting on a decline board or level ground, loading the eccentric phase only or both phases, exercising into tendon pain or short of pain, and progressing with speed then load or simply load. Comment on which aspect of the decline protocol was most effective in causing change in sporting function and tendon pain is reserved for more specific studies with greater numbers.
CONCLUSIONS
In active jumping athletes with patellar tendinopathy, both exercise protocols improved pain and sporting function. This study shows that the decline squat protocol presents a much greater chance of clinical improvement in VISA scores over a 12 month season than the step protocol. Therefore we recommend the use of the decline squat protocol during a rehabilitation programme for patellar tendinopathy in athletes who continue to train and play with pain. Further studies with larger numbers are required to confirm and further explore these findings.
Acknowledgments
We sincerely thank Peter Blanch, Dave Martin, Andrew Chapman, and Greg Lovell for their comments on this manuscript.
REFERENCES
Footnotes
-
Patient consent has been obtained for figure 2
-
Competing interests: none declared
Linked Articles
- Correction