Article Text

Abstract
Objective: To investigate blood indices of muscle damage after a competitive rugby match.
Methods: Fifteen elite amateur rugby players volunteered to participate (mean (SE) age 26.6 (0.7) years, height 179.8 (1.0) cm, weight 87.4 (2.2) kg, and Vo2max 58.5 (1.2) ml/kg/min). The study was conducted after two competitive matches during the 1999–2000 season. Plasma concentrations of lactate, potassium (K+), sodium (Na+), and myoglobin, and the activity of creatine kinase were measured before and after the matches. In addition, the number of tackles by and on each subject and the average duration of the work and rest periods were analysed using video recordings of the matches.
Results: Myoglobin concentration and creatine kinase activity showed appreciable transient increases after the match. Peak values for myoglobin concentration (980 (166) μg/l) and creatine kinase activity (1081 (159) U/l) were observed 45 minutes and 24 hours after the match respectively. Positive and significant correlations were observed between the number of tackles and both peak myoglobin concentration (r = 0.85, p<0.01; n = 14) and peak creatine kinase activity (r = 0.92, p<0.01; n = 14). Plasma lactate and K+ concentrations also showed appreciable increases after the match, whereas plasma Na+ concentration showed a gradual decrease. The mean duration of the work and rest periods were 21.5 (2.2) and 24.3 (3.1) seconds respectively.
Conclusions: The rugby matches resulted in serious structural damage to the muscles, the extent of which was highly dependent on the number of tackles.
- muscle damage
- creatine kinase
- myoglobin
- rugby
- eccentric contraction
Statistics from Altmetric.com
Exercise induced muscle damage has been widely studied after various types of exercise in humans.1–6 Muscle damage after exercise results in a substantial increase in myocellular protein levels in the blood.7 Creatine kinase in the blood is often used as an indirect indicator of muscle damage, its release from muscle tissue into the blood being associated with disruption of the muscle cell membrane.8–10 The extent of muscle damage has been related to both the intensity and duration of exercise, with intensity playing the main role.11 For example, the peak activity of creatine kinase after a marathon race ranges from 500 to 3300 U/l,5,12 whereas its peak activity after exercise with high force eccentric muscle contraction can reach 25 000 U/l.13 Such severe muscle damage immediately results in a reduction in muscle strength of more than 50%, which is completely restored after about 10 days.4,14
Exercise induced muscle damage is mainly caused by strong muscle contraction during intense exercise. In addition to this endogenous factor, exogenous factors are considered to be an important. Direct excessive muscle damage occasionally leads to trauma graded as an injury. In multiple sprint sports such as soccer, rugby, and field hockey, muscle is often damaged by direct impact during exercise in which players contact or collide with each other, even without accompanying exogenous traumas. Zuliani et al15 reported that a normal boxing match of three three minute rounds with two intervals of one minute (real boxing) results in large increases in the serum concentration of creatine kinase and myoglobin, whereas the same exercises without direct contact (shadow boxing) do not, suggesting that the muscle damage observed after real boxing is mainly caused by direct punches to the body. There have been few studies on muscle damage after competitive matches in multiple sprint sports involving body contact such as soccer, rugby, and field hockey in which the relation between exercise with body contact and muscle damage has not been mentioned.
This study investigated muscle damage in rugby players after competitive matches involving fierce body contact.
METHODS
Subjects
Fifteen elite Japanese amateur rugby union players aged 23–30 volunteered to participate. Their physical characteristics were: mean (SE) height, 179.8 (1.0) cm; body mass, 87.4 (2.2) kg; maximal oxygen consumption (Vo2max) on a treadmill, 59.5 (1.2) ml/kg/min. Playing positions included two props, one hooker, two locks, three loose forwards, three centres, two wings, and two fullbacks. Written informed consent was obtained from each subject. The study was approved by the ethics committee for human experiments, University of Tokyo.
Experimental procedures
The study was conducted after two competitive matches in the East Japan Company Rugby Football League during the 1999–2000 season. The matches took place on 14 November and 28 November with no competitive matches between. The matches were played in good weather, and the outdoor temperature was 8–15°C. Plasma creatine kinase activity and plasma concentrations of myoglobin, lactate, potassium (K+), and sodium (Na+) were measured before and after each match.
Blood sampling
Venous blood samples (20 ml for each point of measurement) were obtained through an indwelling cannular in a superficial arm vein from the subjects seated in a slightly reclined position. All blood sampling was conducted at the same time of day (1200–1400 hours) to reduce effects of diurnal variation. A resting blood sample was obtained after the subjects had sat quietly in a slightly reclined position for 20 minutes 48 hours before each match. After each match, blood samples were obtained at 0 (immediately after the match), 45, and 90 minutes and at 24, 48, and 72 hours. All blood samples were processed and stored at −20°C until analysis. The subjects were asked to refrain from ingesting alcohol and caffeine and performing any strenuous exercise for 48 hours before and 72 hours after each match.
Biochemical analysis
Plasma concentrations of K+ and Na+ were determined by potentiometry (model 7450 autoanalyzer; Hitachi, Tokyo, Japan) with ion selective electrodes (Daiichi Pure Chemicals, Tokyo, Japan). Plasma concentrations of lactate and myoglobin were measured by spectrophotometry using a lactate dehydrogenase coupled enzymic system16 and radioimmunoassay using a test kit (Daiichi Radioisotope Laboratory Ltd, Tokyo, Japan) respectively. Plasma creatine kinase activity was determined by spectrophotometrically measuring NADPH formed by hexokinase and the d-glucose-6-phosphate dehydrogenase coupled enzymic system.
Match analysis
The number of tackles in which each subject was involved and the mean duration of the work and rest periods were investigated by analysing video recordings of the two matches. The number of tackles was defined as the total number of times that the player tackled or was tackled in situations in which the player was tackled from in front. The durations of the work and rest periods were defined respectively as the period from the beginning of a play to the interruption of that play by the referee, and the period from the interruption of a play by the referee to the start of the next play.
Statistical analysis
Unless otherwise stated, variables are expressed as mean (SE). The Wilcoxon signed ranks test was used to compare differences between variables measured before and after the match within the same subjects. Correlation analysis was carried out by linear regression, and the Pearson correlation coefficient (r) was calculated. For all statistical analyses, p<0.05 was considered significant.
RESULTS
One subject was badly bruised on the right thigh and dropped out of the match on 14 November 15 minutes into the second half. The remaining subjects completed the match (80 minutes). Therefore all variables are expressed as mean (SE) for the remaining 14 subjects.
Match analyses
The mean (SD) number of tackles was 14.0 (7.4) per match. The relation between the number of tackles and any muscle damage after the match was investigated. The mean (SD) duration of the work and rest periods in the two matches was 21.5 (2.2) and 24.3 (3.1) seconds respectively.
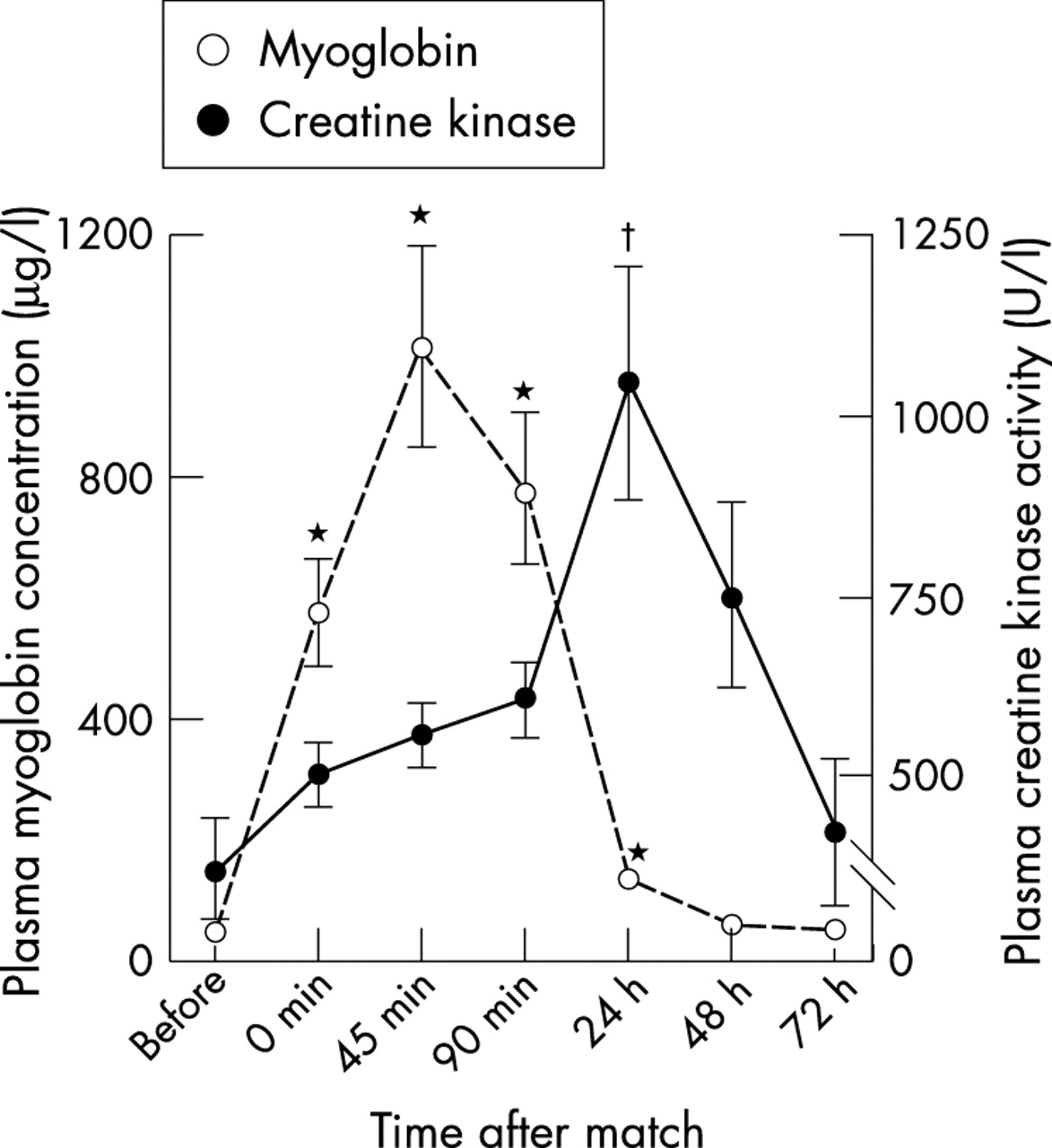
Myoglobin concentration and creatine kinase activity in the plasma
Figure 1 shows plasma myoglobin concentration and plasma creatine kinase activity measured before and after the two matches. Both had significantly increased after the matches. A peak was reached 45 minutes after the match for myoglobin and 24 hours after the match for creatine kinase. They then returned rapidly to their resting levels in an exponential fashion. Peak myoglobin concentration and peak creatine kinase activity in the subject with a bruised right thigh resulting from a tackle by an opposing player were 1641 μg/l (45 minutes after the match) and 2621 U/l (24 hours after the match) respectively. These values are much higher than in the remaining 14 subjects (myoglobin, 980 (166) μg/l; creatine kinase, 1081 (159) U/l). In addition, creatine kinase activity 48 and 72 hours after the matches was 1620 U/l and 1025 U/l respectively and remained at a much higher level than in the other subjects.

Changes in plasma myoglobin concentration and creatine kinase activity after the rugby matches. Values are mean (SE) (n = 14). *, †Significantly different from resting state within the same subjects (p<0.05, Wilcoxon signed ranks test).
The relation between the number of tackles and muscle damage after the match was investigated. Figure 2 shows the relation between the number of tackles and peak myoglobin concentration (45 minutes after the match) and peak creatine kinase activity (24 hours after the match). Positive and significant correlations were observed between both. These results suggest that the extent of muscle damage depends on the number of tackles.

Relation between the number of tackles and (A) plasma myoglobin concentration and (B) plasma creatine kinase activity. Correlation analysis was carried out by linear regression, and the Pearson correlation coefficient (r) was calculated.
Plasma concentrations of lactate, K+, and Na+
Figure 3 shows plasma concentrations of lactate, K+, and Na+ measured before and after the matches. Plasma lactate and K+ were significantly increased after each match, whereas plasma Na+ gradually decreased. Lactate concentration peaked immediately after the match and K+ concentration 90 minutes after the match, thereafter returning rapidly to resting levels (figs 3A,B). Na+ concentration reached its lowest level 90 minutes after the match and thereafter returned rapidly to its resting level (fig 3C). These results suggest that Na+ ions move from the plasma into contracting muscle, and K+ and lactate ions exit contracting muscle. Such an ionic exchange is typical during intense exercise,17 indicating that the intensity of the exercise in these matches was generally high.

{kind=link}
{kind=link}
{kind=link}
Changes in plasma concentrations of (A) lactate, (B) K+, and (C) Na+ after the rugby matches. Values are mean (SE) (n = 14). *Significantly different from resting state within the same subjects (p<0.05, Wilcoxon signed ranks test).
DISCUSSION
The results show that competitive rugby matches induce serious structural damage to muscle tissue, the extent of which is highly dependent on the number of tackles. Plasma myoglobin concentration and plasma creatine kinase activity, indirect indicators of muscle damage, had increased significantly after each match. Peak creatine kinase activity 24 hours after the match was 1081 (159) U/l, which was almost as high as after a marathon race.18
Plasma lactate and K+ concentrations had significantly increased after the match, whereas plasma Na+ concentration gradually decreased. Such ionic changes are typically observed during intense exercise,17 indicating that the intensity of exercise during these matches was generally high. In addition, match analysis showed that the mean durations of the work and rest periods were 21.5 (2.2) and 24.3 (3.1) seconds respectively. On the basis of these results, activity of high intensity was performed intermittently more than 100 times a match. Such intermittent activity is usually accompanied by running independently of the mode.19 Rugby matches therefore involve considerable acceleration and deceleration of the centre of mass. In particular, the hamstrings work eccentrically to slow flexion of the hip and extension of the knee during the landing phase to decelerate the centre of mass.20,21 Eccentric muscle contractions, in which the muscle lengthens as it exerts force, generate greater tension per cross sectional area of active muscle than concentric contractions,7 resulting in considerable structural damage to muscle tissue.7,22 Therefore muscle damage observed after rugby matches is partially caused by intermittent repetitions of intense and eccentric muscle contraction during running, especially sprinting.
Thompson et al23 reported that intermittent high intensity shuttle running for 90 minutes in an activity pattern representative of multiple sprint sports such as soccer, rugby, and field hockey produced muscle soreness and damage, which was mainly caused by eccentric muscle contractions during the landing phase in the sprinting, as reported in this study. However, there is a considerable difference in the extent of muscle damage between findings in the present study and those of Thompson et al.23 Peak plasma creatine kinase activity in our study was 1081 (159) U/l, which is about 1.4-fold higher than that reported by Thompson et al.23 This suggests that there was an additional cause of the extensive muscle damage in the present study. However, peak plasma creatine kinase activity cannot be simply compared between the two studies because of experimental differences such as the characteristics of the subjects.
A competitive rugby match usually involves aggressive and forceful plays with body contact such as scrums, tackles, rucks, and mauls. The tackle causes the first contact with another player in the opposing team at every restart of any play in rugby matches, which is necessarily followed by other contact plays such as rucks and mauls. Tackling is one of the basic skills required to stop the ball carrier in the opposing team and is common to all playing positions. In particular, tackles from in front of the tackled player are carried out to stop the ball carrier, who is travelling with great momentum, usually resulting in greater force at impact and greater kinetic energy to the tackling player. However, if the tackling player has the greater momentum, the tackled player receives greater kinetic energy—that is, the tackled player receives more damage to his body. In any case, it is clear that the total momentum of the tackling and tackled players before body contact is redistributed between them at impact by the law of conservation of energy, and also the kinetic energy produced. The players involved in a tackle thus receive more or less damage to their body with respect to each other at impact regardless of whether tackling or being tackled.
Therefore it is reasonable to suggest that the tackle is representative of plays involving body contact in rugby, and attention should be focused on both tackling and tackled players. In this study, the relation between the total number of tackling and tackled plays, and the extent of muscle damage after competitive rugby matches was investigated to help to clarify the cause of muscle damage. There was a significant correlation between the number of tackles and both peak myoglobin concentration (fig 2A; r = 0.85, p<0.01) and peak creatine kinase activity (fig 2B; r = 0.92, p<0.01). Therefore muscle damage is dependent on the number of tackles during a match. In addition, the small intercept values of each regression equation exhibited in fig 2 suggest that the direct impact of the tackle was the major cause of muscle damage.
The subjects were highly experienced, technically skilled rugby players (more than 10 years of playing), who were familiar with activity patterns found in rugby such as intermittent running or sprinting through either daily practice or matches over many years. Contact plays such as tackles, which are also activity patterns representative of rugby, are not usually experienced at such a severe level in daily practice as in competitive matches. Therefore, the highly technical skills and familiarity with typical activity patterns found in rugby, except for hard tackles, in the present subjects is probably the main reason for the reduced muscle damage induced by the repeated eccentric muscle contractions, despite the considerable intermittent running/sprinting during the matches.
In summary, the direct impact of tackles on the body is probably the major cause of muscle damage observed after a competitive rugby match, in addition to the repeated eccentric muscle contractions involved in the intermittent running/sprinting of rugby matches.
Muscle damage immediately after strenuous exercise has been observed as disruptions in the A band and localised dissolution of Z lines24 by electron microscopy,8,25 which was found to be associated with the structural damage of the contractile apparatus due to mechanical stress. This repeated micro-damage to muscle fibres is suggested to cause muscle strains or tears graded as injuries. In addition, the capacity of the damaged muscle to generate force is greatly reduced,4,14 and this reduction in muscle function not only prevents a stable rugby performance during a match, but also increases the risk of injuries such as strained or torn ligaments of the knee joint because of increased joint laxity.26 Indeed, most injuries in rugby players are sprains, strains, and ruptures of muscles, ligaments, and joints in the lower limbs.27 The incidence of these injuries increases with the increased number of tackles during a match, which clearly increases the extent of muscle damage. This is supported by the findings of previous studies27,28 showing that many injuries occurred when players were hit by each other in tackling situations.
In Japan, the competitive rugby season is between September and January. Between seven and fourteen matches are generally played in league and elimination tournaments. It is of paramount importance that players stay in good physical condition throughout the season for good results to be achieved. Therefore injury prevention and rapid recovery from muscle damage is very important. In general, severe muscle soreness and decreased muscle strength are induced by unaccustomed strenuous exercise, regardless of training status.6 However, the extent of muscle damage is significantly influenced by training status.6,29,30 Vincent and Vincent6 reported that mean peak creatine kinase activity in trained subjects after intense weight training for leg muscles was about 60% lower than that in untrained subjects, suggesting that training allows muscles to become more resistant to damage by exercise. In addition, damage to a trained muscle is repaired at a faster rate.6,29,30 Indeed, the second and third bouts of the same exercise one week after the first bout of severe unaccustomed eccentric exercise was found to induce considerably less muscle damage and loss of strength even in untrained subjects, and this training effect was found to last about six weeks, suggesting a considerable and long lasting adaptation.4,31,32 These results suggest that introducing hard tackles, which are the main cause of muscle damage in rugby matches, into daily rugby training during the preseason may reduce the extent of muscle damage during matches in the competitive season. However, further studies are required to elucidate this possible effect.
Take home message
Competitive rugby matches cause serious structural damage to muscle tissue, the extent of which depends on the number of tackles. The direct impact of the tackle on the body is the major cause of muscle damage.