Article Text

Abstract
Background Hamstring injury with intramuscular tendon involvement is regarded as a serious injury with a delay in return to play (RTP) of more than 50 days and reinjury rates up to 63%. However, this reputation is based on retrospective case series with high risk of bias.
Objective Determine whether intramuscular tendon involvement is associated with delayed RTP and elevated rates of reinjury.
Methods MRI of male athletes with an acute hamstring injury was obtained within 5 days of injury. Evaluation included standardised MRI scoring and scoring of intramuscular tendon involvement. Time to RTP and reinjury rate were prospectively recorded.
Results Out of 70 included participants, intramuscular tendon disruption was present in 29 (41.4%) injuries. Injuries without intramuscular tendon disruption had a mean time to RTP of 22.2±7.4 days. Injuries with <50%, 50%–99% and 100% disruption of tendon cross-sectional area had a mean time to RTP of 24.0±9.7, 25.3±8.6 and 31.6±10.9 days, respectively. Injuries with full-thickness disruption took longer to RTP compared with injuries without disruption (p=0.025). Longitudinal intramuscular tendon disruption was not significantly associated with time to RTP. Waviness was present in 17 (24.3%) injuries. Mean time to RTP for injuries without and with waviness was 22.6±7.5 and 30.2±10.8 days (p=0.014). There were 11 (15.7%) reinjuries within 12 months, five (17.2%) in the group with intramuscular tendon disruption and six (14.6%) in the group without intramuscular tendon disruption.
Conclusion Time to RTP for injuries with full-thickness disruption of the intramuscular tendon and waviness is significantly longer (by slightly more than 1 week) compared with injuries without intramuscular tendon involvement. However, due to the considerable overlap in time to RTP between groups with and without intramuscular tendon involvement, its clinical significance for the individual athlete is limited.
- hamstring
- muscle Injury
- mri
- tendon
Statistics from Altmetric.com
Introduction
Hamstring injury with involvement of the ‘intramuscular’1–4 or ‘central’5 tendon is regarded as a serious injury with prolonged recovery time and high reinjury rate. ‘Intramuscular’ and ‘central’ tendon refers to the part of the tendon to which muscle fibres attach. In the British Athletics Muscle Injury Classification,6 7 a lesion extending into the tendon is referred to as an ‘intratendinous’ or ‘c’ injury and therefore includes injuries of the free and intramuscular tendon.
Comin et al 5 initially proposed central tendon disruption as a prognostic factor for delayed return to play (RTP). In a retrospective cohort of 62 injuries among Australian rules football and rugby players, 9 biceps femoris injuries with central tendon disruption took a median 72 days to recover. Compared with a median 21 days for biceps femoris injuries with an intact central tendon, this is a threefold to fourfold increase in recovery time. Moreover, 25% of the central tendon injuries were surgically repaired. Pollock et al 7 retrospectively analysed outcome for track and field athletes with injuries graded according to the British Athletics Muscle Injury Classification.6 Compared with myofascial or musculotendinous injury, the 15 intratendinous injuries took significantly longer to return to full training and had a reinjury rate of up to 63%. Injuries classified as 3 c (longitudinal tendon disruption >5 cm and >50% of tendon cross-sectional area (CSA) with no evident discontinuity) had a mean time to return to full training (TRFT) of 84 days.
Understanding the role of intramuscular tendon involvement is limited by the retrospective study designs and relative small sample sizes—with a total of 27 published cases and the substantial risk of bias in both studies. The clinicians involved in the decision for RTP were not blinded to the MRI findings. Therefore, influence of MRI results (ie, the presence or absence of intramuscular tendon involvement) on progression through rehabilitation and the RTP decision cannot be ruled out. This phenomenon has been referred to as a potentially ‘self-fulfilling prophecy’8: the hypothesis that a certain type of injury takes longer to heal could potentially influence (ie, delay) the physician’s RTP decision, thereby prolonging time to RTP for this type of injury. Given these limitations, prospective studies with blinding are required to determine whether intramuscular tendon involvement may result in delayed resolution.
In this prospective study, our aim was to exclude the risk of bias by blinding the RTP decision-makers to MRI findings and determine whether intramuscular tendon involvement is associated with delayed RTP or elevated rates of reinjury. Our hypothesis was that injuries with intramuscular tendon involvement are associated with prolonged time to RTP and a higher reinjury rate.
Methods
Participants
Participants in this study were part of a double-blind randomised controlled trial on the effect of platelet-rich plasma (PRP) in hamstring injuries (ClinicalTrial.gov number NCT01812564).9 Eligibility criteria are shown in box 1. Participants were athletes with an acute hamstring injury (MRI-confirmed, grades I and II) that were randomised into three groups. Groups received a 3 mL injection of platelet-rich plasma, a 3 mL injection of platelet-poor plasma or no injection. All participants underwent a standardised criteria-based rehabilitation programme. There was no benefit of PRP injection over intensive rehabilitation in terms of RTP. For the current study, we only included participants with a complete dataset on completion of the rehabilitation programme and clearance by the treating physiotherapist.
Informed consent was obtained at inclusion, and approval was obtained from the Ethical Committee of Aspetar, Orthopaedic and Sports Medicine Hospital.
Eligibility criteria
Inclusion criteria
Age 18–50 years
Acute onset posterior thigh pain
MRI within 5 days of injury
Positive MRI for grade I–II hamstring injury
Male sex
Able to perform five physiotherapy sessions per week at the clinic
Exclusion criteria
Contraindications for MRI
Chronic hamstring injury or reinjury
Concurrent injury inhibiting rehabilitation
Unwilling to comply with follow-up
No available data on completion of rehabilitation programme
Needle phobia
Overlying skin infection
Diabetes, immunocompromised state
Medication with increasing bleeding risk
Medical contraindication to injection
MRI
All MRIs were performed within 5 days of the injury.
MRI protocol
Images were acquired with a 1.5T magnet system (Magnetom Espree, Siemens, Germany) and a body matrix coil. Coronal and axial proton density (PD) weighted images (repetition time (TR)/time to echo (TE) 3000/32 ms; field of view (FOV) 240 mm; slice thickness 5 mm; matrix, 333×512) were obtained. Subsequently, coronal and axial PD-weighted images with fat saturation (PD-FS) were obtained (TR/TE 3000/32 ms; FOV 240 mm; slice thickness 3.5 mm; matrix 326×512 for coronal and TR/TE 3490/27 ms; FOV 320 mm; slice thickness 3.5 mm; matrix 333×512 for axial).
MRI characteristics
MRIs were scored by an experienced musculoskeletal radiologist using standardised scoring forms including size and location of the injury. If more than one muscle was involved, the muscle with the primary (ie, largest) injury was determined. The radiologist was blinded to clinical details of the injury.
The intramuscular tendon was defined as the section of the tendon that extends along and into the muscle, thereby having muscle fibres attached to it. The free tendon (either proximal or distal) has no muscle fibres attached10 (figure 1).

Schematic overview of the free and intramuscular tendon.
We incorporated the components of the central tendon injuries5 and ‘c-injuries’ in the British Athletics Muscle Injury Classification6 into scoring of the intramuscular tendon. We recorded (1) the presence of tendon disruption (figure 2A), subdivided into <50%, 50%–99% and 100% of tendon cross-sectional area (CSA), (2) longitudinal tendon disruption and (3) the presence of waviness (figure 2B).
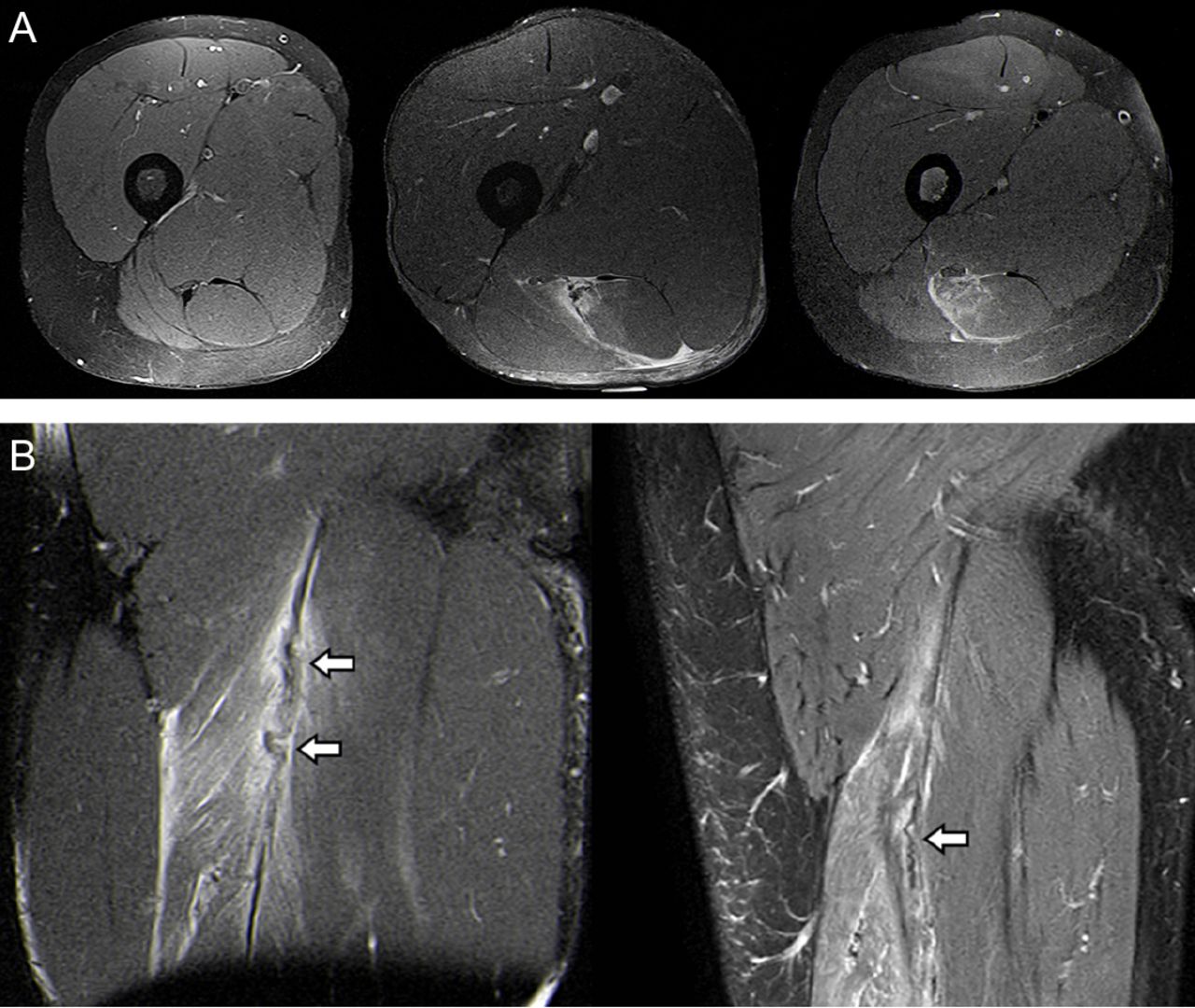
(A) Proton density with fat saturation (PD-FS) weighted axial MR images demonstrating no abnormality of the hamstring tendons (left), partial-thickness disruption of the intramuscular tendon with intrasubstance high signal intensity (middle) and full-thickness intramuscular tendon disruption (right). (B) PD-FS and T2-FS weighted coronal MR images demonstrating evident (left) and more subtle (right) waviness of the intramuscular tendon (arrows).
Disruption was defined as the presence of a focal tendon defect (% of CSA), characterised by loss of low signal intensity within the tendon. Longitudinal tendon disruption (in cm) was scored separately for injuries with partial-thickness and full-thickness tendon disruption. For injuries with partial-thickness tendon disruption, we measured the craniocaudal length of tendon disruption. For injuries with full-thickness tendon disruption, the distance between tendon ends, or retraction, was recorded.
Additionally, the injury was graded according to the modified Peetrons classification11 (grade 0: no abnormalities on MRI; grade I: oedema without architectural distortion; grade II: oedema with architectural distortion; grade 3: complete rupture of the muscle-tendon unit) and the extent of oedema was measured. Extent of oedema, defined as abnormal high signal intensity on fluid-sensitive sequences, was recorded (in cm) in craniocaudal, anteroposterior and mediolateral directions. Subsequently, cross-sectional area (in cm²) and volume (in cm³) were calculated. Distance of the cranial pole of the oedema to the caudal margin of the ischial tuberosity was also measured in centimetre. Excellent reliability has been reported for measuring these MRI parameters in acute hamstring injury.12 The British Athletics Muscle Injury Classification has been tested for intra-rater and inter-rater reliability, revealing at least substantial agreement in all groups.13 14
Outcome measures
Return to play
Time to RTP was defined as the number of days from injury to completion of a six-stage criteria-based rehabilitation programme, including three sport-specific training phases.15 Participants progressed from one phase to the next based on predefined clinical progression criteria, while the treating physiotherapist remained blinded to MRI results. The rehabilitation programme was successfully completed when sport-specific activities were performed unrestricted and pain free. Following completion, clearance to RTP was given by the treating physiotherapist.
As recently outlined, there is no uniform RTP definition following hamstring injury.16 Our chosen definition is an MRI-independent measure of clinical recovery and very closely related to the RTP decision used in clinical practice. For completeness, we also scored the number of days from the injury to clearance by the treating sports medicine physician (SMP), who was not blinded to the MRI results. Guidelines for discharge by the SMP included completion of the rehabilitation programme, results of an isokinetic assessment and clinical evaluation.
Reinjury rate
Reinjury was defined as acute onset posterior thigh pain occurring during competition or training in the same leg as the index injury within 1 year after RTP. These were subdivided into short-term (≤2 months after RTP), mid-term (≤6 months after RTP) and long-term (≤12 months after RTP) reinjuries. Participants were instructed to consult the hospital or study coordinator in case of any clinical suspicion of a reinjury and were contacted by telephone on a monthly basis.
Statistical analysis
Statistical analysis was carried out with SPSS V.23.0 (SPSS, Chicago, Illinois, USA).
We analysed differences in time to RTP between groups using a multiple regression analysis. In the multiple regression analysis, we controlled for treatment received, MRI grade, extent of oedema and distance of the lesion to the ischial tuberosity, since these have been associated with to time to RTP.3 9 17–23 Although a recent systematic review24 concluded that there is conflicting evidence for these parameters, these variables were included in the analysis to control for any potential effect on time to RTP.
We repeated the analysis to determine whether any effect of intramuscular tendon involvement would also apply to time to RTP if it were defined as the number of days from injury to discharge by the treating SMP.
Pearson correlation tests were carried out to detect a relationship between longitudinal tendon disruption and time to RTP.
Results
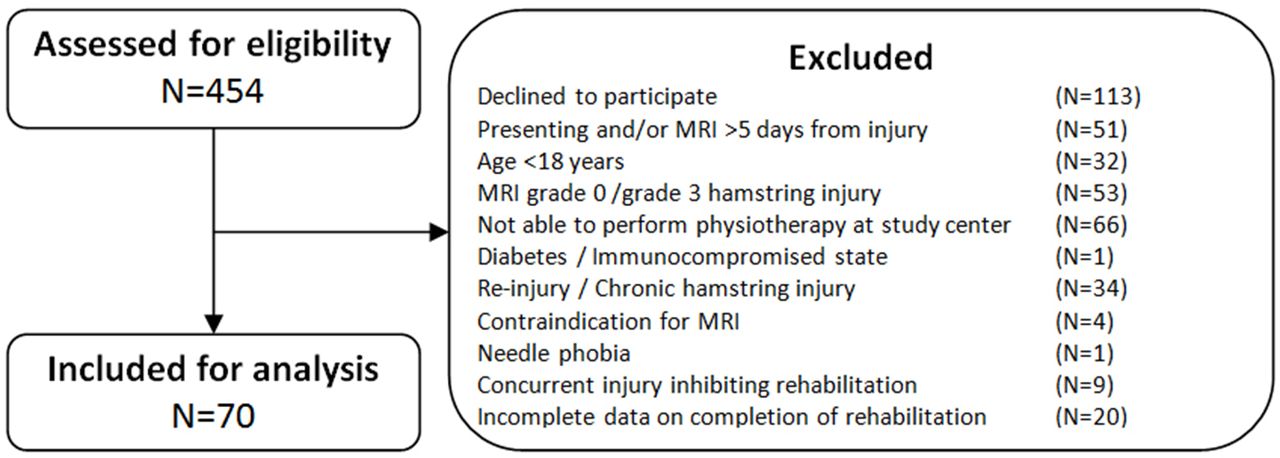
Seventy participants with a median age of 24 (IQR 21–30) were included in the analysis (figure 3). Baseline patient and MRI characteristics are shown in table 1. Twenty-nine (41.4%) hamstring injuries involved disruption of the intramuscular tendon, including 17 (58.6%) partial-thickness and 12 (41.4%) full-thickness intramuscular tendon injuries. Intramuscular tendon injuries were most often located in the biceps femoris (long head).

Flowchart of the inclusion process.
Baseline demographic and MRI characteristics. Values are presented as mean (±SD) or median (IQR) as appropriate for continuous variables and as frequency (%) for categorical variables
Of the 12 full-thickness intramuscular tendon injuries, six were located in the biceps femoris (long head), four were located in the common tendon of the biceps femoris (long head) and the semitendinosus and two were located in the semimembranosus. All 12 athletes were performing at the elite level in Qatar and included nine first division football players, one hockey player, one volleyball player and one decathlete.
Intramuscular tendon and time to RTP
Mean time to RTP was 24.5±8.9 days. Mean time to RTP in participants without and with intramuscular tendon disruption was 22.2±7.4 and 27.7±10.0 days, respectively. Only injuries with full-thickness intramuscular tendon disruption were correlated with a significantly longer time to RTP compared with injuries without intramuscular tendon disruption (F(9,58)=2.61, p=0.025, R²=0.29, R²adjusted=0.18) (figure 4A and table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Scatter plot of time to RTP (in days) for injuries without intramuscular tendon disruption and injuries with increasing degrees of intramuscular tendon disruption. (B) Scatter plot of time to RTP (in days) for injuries without and with waviness. CSA, cross-sectional area; RTP, return to play.
Time to RTP and reinjuries for injuries without intramuscular tendon disruption and injuries with increasing degrees of intramuscular tendon disruption
There was no significant correlation between longitudinal tendon disruption and time to RTP (Pearson correlation coefficient=0.125, p=0.632 for length of tendon disruption in partial-thickness tendon tears and Pearson correlation coefficient=0.114, p=0.724 for retraction in full-thickness tendon tears).
Waviness was present in 17 (24.3%) of all injuries and in 17 (58.6%) of the intramuscular tendon injuries. All injuries with the presence of waviness had either 50%–99% or 100% disruption of intramuscular tendon CSA. Eleven injuries (91.7%) with full-thickness disruption of the intramuscular tendon had the presence of waviness on MRI, compared with six injuries (50.0%) with 50%–99% disruption of tendon CSA. Mean time to RTP for injury without and with waviness was 22.6±7.5 and 30.2±10.8, respectively (F(7,60)=3.20, p=0.014, R²=0.27, R²adjusted=0.19) (figure 4B).
In 48.6% of cases, participants were discharged by the SMP the same day the rehabilitation programme was successfully completed. The median number of days between completion of the criteria-based rehabilitation programme and discharge by the SMP was 1 (IQR 0–3) day. For completeness, an additional analysis was performed with time to RTP defined as the number of days from injury to discharge by the treating SMP. This revealed equivalent results.
Intramuscular tendon and re-injury rate
All 70 participants were available for the reinjury rate analysis. Reinjury rates are presented in table 2. In total, there were six (8.6%) recorded reinjuries within 2 months, eight (11.4%) within 6 months and 11 (15.7%) within 12 months. We refrained from further statistical analysis due to the low number of reinjuries.
Discussion
In the largest blinded prospective study on acute hamstring injuries with intramuscular tendon involvement, we found that full-thickness disruption and waviness of the intramuscular tendon are associated with increased time to RTP. Compared with injuries without intramuscular tendon involvement, these injuries take slightly more than a week longer to RTP. However, the considerable overlap between groups with and without intramuscular tendon involvement substantially limits the clinical (ie, predictive) value of intramuscular tendon involvement. No statistically significant differences were found between injuries without intramuscular tendon disruption and injuries with partial-thickness intramuscular tendon disruption. The low number of reinjuries does not allow for statistical comparisons.
The time to RTP for hamstring injuries with intramuscular tendon involvement is considerably shorter than previously reported. Comin et al 5 studied hamstring injuries in Australian rules football and rugby players. With a median RTP of 72 days, biceps femoris injuries with intramuscular tendon involvement took 51 days longer than biceps femoris injuries without intramuscular tendon involvement (median 21 days). In these groups, we have found a mean time to RTP of 28 and 22 days. Pollock et al 7 investigated hamstring injuries in track and field athletes and presented separate data for different grades with tendon involvement. They reported a mean TRFT of up to 84 days. To be exact, mean TRFT was 27 days for 2 c injuries (longitudinal tendon disruption <5 cm and <50% of tendon CSA) and 84 days for 3 c injuries (longitudinal tendon disruption >5 cm and >50% of tendon CSA with no evident discontinuity). Pollock et al reported no 4 c injuries (complete discontinuity of the tendon with retraction). In the present study, participants with an acute hamstring injury involving <50% of tendon CSA had a mean time to RTP of 24 days, and those with an injury involving 50%–99% of tendon CSA had a mean time to RTP of 25 days. Moreover, in the present study, injuries involving a full-thickness tear of the intramuscular tendon had a mean time to RTP of 32 days.
Differences in time to RTP between studies may be attributable to several methodological differences. First, an element of the RTP differences may be explained by the different sports of the participants, as different sports have different (functional) requirements. Second, it is highly unlikely that treatment protocols are identical across studies. However, a comparison is not possible due to a limited description of the rehabilitation programmes. Third, in each study, a different definition of time to RTP was used. Clear definitions enhance communication and comparison and are thus recommended. We refer to the consensus statement by Ardern et al.25 Comin et al used ‘recovery time’,5 which was not further specified. Pollock et al used TRFT, which represented unrestricted training sprint efforts at full pace.7 As both studies involve a retrospective review of medical records, the physicians involved in the RTP decision were not blinded to MRI characteristics such as intramuscular tendon disruption. This is where the possibility of the aforementioned ‘self-fulfilling prophecy’ is introduced, which may have caused a delay in RTP in cases with tendon disruption. Finally, the intratendinous (‘c’) injury described by Pollock et al 6 7 includes injury of the free tendon, which has been associated with longer time to return to preinjury level.19
Due to the large spread of time to RTP, it remains difficult to provide an accurate RTP prognosis for the individual athlete. The contribution of intramuscular tendon involvement on MRI to predicting RTP is limited considering the relatively small differences and substantial overlap between groups. This is in accordance with available evidence on the predictive value of MRI parameters for RTP. Despite a growing number of these studies, a systematic review24 concluded that there is currently no strong evidence to support that any MRI parameter predicts time to RTP. Wangensteen et al demonstrated that the additional predictive value of MRI was minimal compared with baseline patient history and clinical examination alone.26 Even with MRI included in the model, only 32% of the variance in time to RTP could be explained by the included parameters, indicating that it remains a major challenge to accurately predict RTP for the individual athlete. Even though intramuscular tendon involvement was not included as a parameter in Wangensteen et al’s assessment, our data do not suggest that their conclusion needs to be revisited.
We reported lower reinjury rates for injuries with intramuscular tendon involvement compared with those reported by Pollock et al 7 (up to 25% and 63%, respectively). Any explanation for this difference would be pure speculation at this point. Future research should investigate reasons for these differences.
Strengths and limitations
To our knowledge, this is the largest cohort with hamstring injuries involving the intramuscular tendon. The main strengths are the prospective study design, blinding of MRI results and the controlled rehabilitation parameters. Moreover, the multivariate analysis allowed us to control for potential covariates.
There are limitations to this study. First, the cohort is relatively homogeneous with predominantly professional football players, potentially reducing the external validity of this study. Twenty athletes were excluded due to incomplete data on completion of rehabilitation, which introduces risk of bias. Second, images were acquired by a 1.5T MRI. It is conceivable that greater diagnostic accuracy might be achieved by using a 3.0T MRI. Third, the number of injuries among different degrees of intramuscular tendon involvement is small. Moreover, the low number of reinjuries does not allow for description of this subgroup. For reinjury analysis, to detect moderate-to-strong associations, more than 20 (re-)injuries would be required27 We recorded a total of 11 reinjuries.
Clinical relevance
Following standardised criteria-based rehabilitation without specific adjustments for intramuscular tendon involvement, injury with partial-thickness intramuscular tendon disruption is not associated with prolonged RTP. Time to RTP for injuries with full-thickness disruption and waviness is significantly longer (by slightly more than 1 week) compared with injuries without intramuscular tendon involvement. Based on the differences in time to RTP between groups in this study, intramuscular tendon involvement alone does not warrant surgical intervention. Tendon waviness observed on MRI was only seen in those injuries involving intramuscular tendon injuries with more than 50% of tendon CSA.
Conclusion
In acute hamstring injuries among athletes, full-thickness disruption of the intramuscular tendon and waviness are associated with a longer time to RTP. Compared with injuries without intramuscular tendon involvement, these injuries take slightly more than a week longer to RTP. Partial-thickness and longitudinal intramuscular tendon disruption were not significantly associated with time to RTP. Due to the considerable overlap between groups with and without intramuscular tendon disruption, the clinical significance of intramuscular tendon involvement for the individual athlete is limited.
What are the new findings?
The clinical significance of intramuscular tendon involvement for the individual athlete is limited.
Using clinical criteria for progression through a criteria-based rehabilitation programme resulted in good outcome in terms of time to return to play (RTP) and reinjury rate.
Full-thickness disruption of the intramuscular tendon and waviness were associated with increased time to RTP. Differences between injuries with and without intramuscular tendon involvement were considerably smaller than previously reported.
Partial-thickness intramuscular tendon disruption was not associated with increased time to RTP.
Waviness was only present in intramuscular tendon injuries with >50% disruption of tendon cross-sectional area.
Acknowledgments
The authors would like to thank Ms. Jolyn Waij for drawing figure 1 and Mr. Jake Bambrough for his help with preparation of the manuscript. Furthermore, we want to express our gratitude to Mr. Nuno Rui Cools Paulino Pereira for his contribution to the statistical analysis.
References
Footnotes
Contributors AM was involved in study design, data collection, data analysis, data interpretation and drafting. EA was involved for radiological expertise, evaluation of MRI scans and drafting. RW, BH, CE and FH were involved in data collection and drafting. JT was involved in study design, data interpretation and drafting.
Funding Internally funded by Aspetar.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical Committee of Aspetar, Orthopaedic and Sports Medicine Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.