Article Text

Abstract
Background Sport injury severity can be detected by duration of time loss and reduction of sporting performance.
Aim To detect injury type-specific time loss duration and sporting performance reduction in judo.
Methods An online survey of active and former judo athletes was conducted (exclusion criterion: incomplete questionnaire). Only injuries causing more than 3 weeks’ time loss were recorded. Athletes classified themselves into performance classes. Injury type-specific frequencies were recorded according to gender, age and performance level. Injury severity was assessed by time loss duration and performance reduction.
Results The study included 4659 athletes (65% male, 38% competitive sports). The most commonly injured body regions were the upper extremity (41%) and the lower extremity (39%). Anterior cruciate ligament (ACL) ruptures were the most severe injury type (time loss: 4% of cases 3–6 weeks, 6% 6–12 weeks, 26% 3–6 months, 32% 6–9 months, 18% 9–12 months, 14%>12 months; performance reduction: 32% same level, 39% slightly reduced, 24% strongly reduced, 5% stopped judo). The second most severe type of injury was a vertebral disc prolapse (time loss: 26% 3–6 weeks, 31% 6–12 weeks, 20% 3–6 months, 7% 6–9 months, 3% 9–12 months 13%>12 months; reduction of sporting performance: 39% same level, 34% slightly reduced, 20% strongly reduced, 8% stopped judo).
Conclusion Across genders and performance levels, ACL ruptures and vertebral disc prolapses were the most severe injuries with respect to time loss and sporting performance reduction.
- Sport injuries
- time loss
- reduction sporting performance
- judo
Statistics from Altmetric.com
Introduction
Judo is a popular sport, with approximately 20 million active participants worldwide.1
Kujala et al used insurance data to compare injuries sustained in judo with those in football, ice hockey, volleyball, basketball and karate in Finland and concluded that, after karate, judo had the second highest injury rate.2 Sports injuries can have serious consequences for injured athletes, such as post-traumatic degenerative joint changes or an inability to continue sports. The epidemiology of ball sports injuries has been investigated in numerous studies.3–6 Subsequent to their findings, sport-specific injury prevention programmes have been successfully introduced in many sports to reduce the risk of common injuries that have serious consequences for injured athletes.7–9
Effective injury prevention programmes are based on knowledge of sport-specific injury risk and the severity of common injuries in different sports. Sporting time loss is frequently used to assess the severity of sports injuries.10–14 In the definition of sports injuries, a distinction is made between injuries with and without time loss. Time-loss injuries are those that restrict participation in training or competition for at least 24 hours.13–16 Furthermore, the duration of time loss is considered a way of defining injury severity.11 12 In team handball, Olsen et al defined injuries with a time loss of >21 days as major injuries.17 Sport injury severity can also be measured by the effect on sporting performance. A recent meta-analysis on return to sports after an anterior cruciate ligament (ACL) rupture by Ardern et al showed that only 63% of affected athletes returned to their preinjury level following ACL reconstruction.18
In judo, the most common injuries reported in the literature are sprains and strains.19 However, whether these injuries lead to any time loss or a reduction in sporting performance has not been widely investigated. In a study by Barrault et al involving data from 154 judo competitions, 0.6% of athletes were sent to hospital after injury.20 Green et al reported an absence from competition of between 12 and 27 days for judo athletes who had an injury during competition and were unable to return to sports immediately.21 None of the study groups provided details about specific injury types.
To our knowledge, no data have been published analysing injuries across performance levels, with a serious consequence measured by time loss and reduction of sporting performance.
Therefore, our study aimed to examine the consequences of severe injuries among elite and recreational judo athletes with respect to time loss from sport and reduction in sporting performance across the genders and level of performance.
Materials and methods
Development of the survey and data collection
During the preparation for this cross-sectional study on severe injuries among national and international competitive and recreational judo athletes, 25 judo athletes contributed to the development of a pilot survey. After evaluation of this pilot, a final questionnaire with 139 questions was presented as an online survey using the software SurveyMonkey. The online survey was open for 90 days from October until December 2013. The survey was published in English, French and German on the homepage and the Facebook page of the German Judo Federation and the European Judo Union. Active and former judo athletes were asked to respond to the survey.
The survey comprised three sections. The first section contained questions on athletes’ competitive level and age when completing the survey. The athletes were also asked to classify themselves into five performance levels—international elite (place 1–5 Olympic Games, World Championship, European Championship), international (national team), national (national championships medal), regional (1 st or 2nd National League) or recreational sports—by marking for the highest level at which they had competed in their career.
The second section included questions about the athletes’ injuries. The athletes were asked to report only injuries that resulted in a time loss of >3 weeks. When a positive answer was given concerning an injury to a region of the body, an athlete was asked to specify the injury type. For each injury type, the duration of time loss, the sporting level following the return to sport and the age when the injury occurred were assessed.
The duration of time loss was measured according to the following intervals: (1) 3 to 6 weeks; (2) 6 weeks to 3 months; (3) 3 to 6 months; (4) 6 to 9 months; (5) 9 to 12 months and (6) >12 months. The athletes were asked to specify all the relevant injuries they had had during their career, according to the definition given below.
The reduction of sporting performance level after returning to sports was measured in the same way. The athletes classified themselves into four levels: (1) same level; (2) slightly reduced; (3) significantly reduced; (4) stopped practising judo.
In the third section, data on age when completing the survey, gender, weight class and number and duration of active judo training sessions per week were collected.
Definitions
Injury was defined as any musculoskeletal problem causing a break in training or competition for >3 weeks, in accordance with the definition for severe injuries published by Olsen et al 17 All injuries were self-reported, and no clinical verification was required.
Injuries that were acknowledged by more than 4% of all of the sampled athletes were defined as common injuries and included in the study.
In order to draw a clear boundary between competitive sports and recreational sports, athletes who classified themselves as regional level athletes were excluded from the group comparison. Athletes who classified themselves as competing at the international elite, international or national levels were grouped into the ‘competitive sports’ category, while athletes who stated their level as the recreational sports level comprised the ‘recreational sports’ category.
Study population
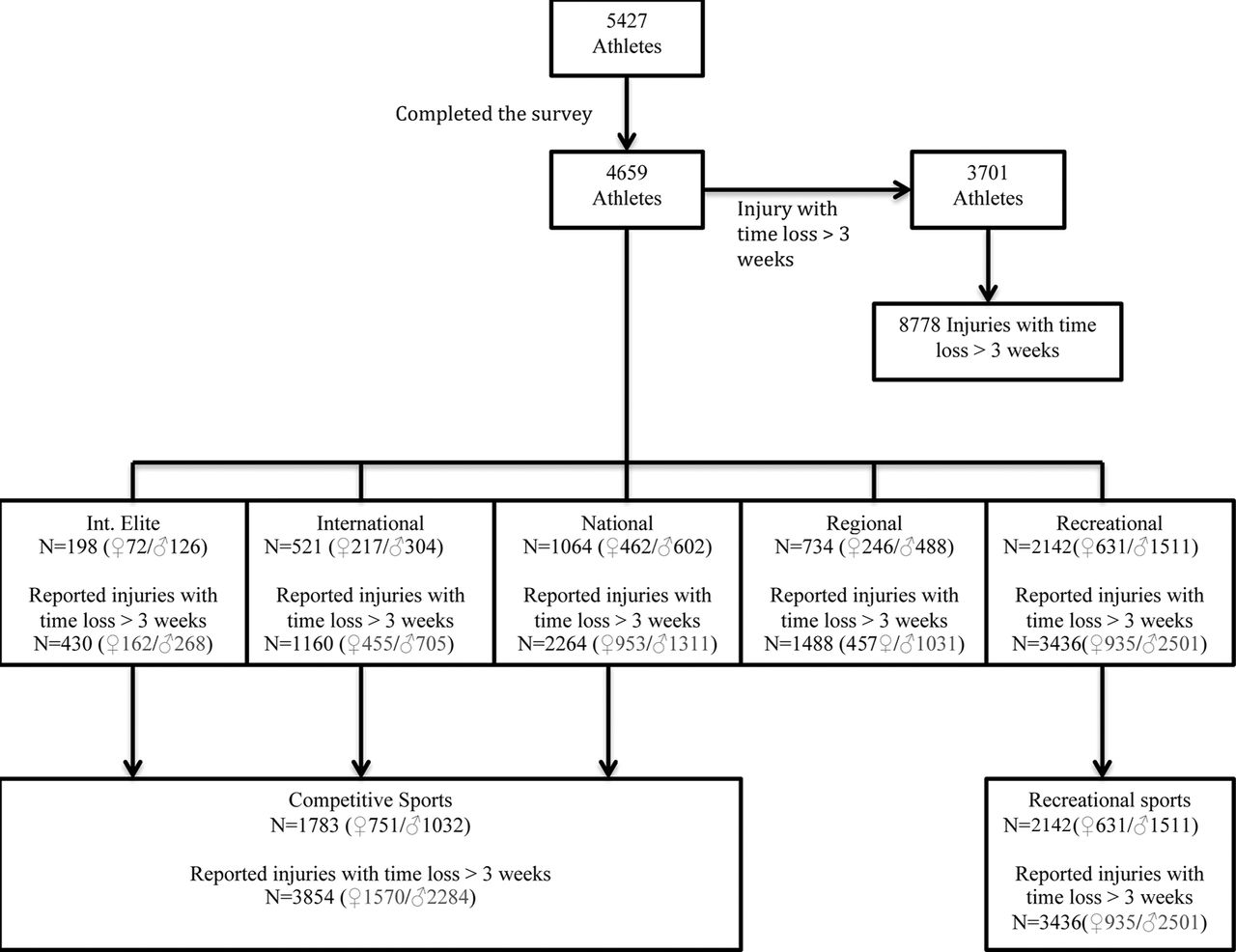
A total of 5427 participants took part in the survey. The exclusion criterion was an incomplete questionnaire. Ultimately, data from 4659 athletes who completed the survey were available for final analysis. The athletes included in the study, the performance level classifications and the numbers of reported injuries are shown in figure 1. Table 1 presents the distribution of the athletes with respect to sporting performance and weight class. Of the full sample, 1783 (38%), of whom 751 (42%) were female, were grouped as competitive athletes, and 2142 (46%), of whom 631 (29%) were female, were grouped as recreational athletes.
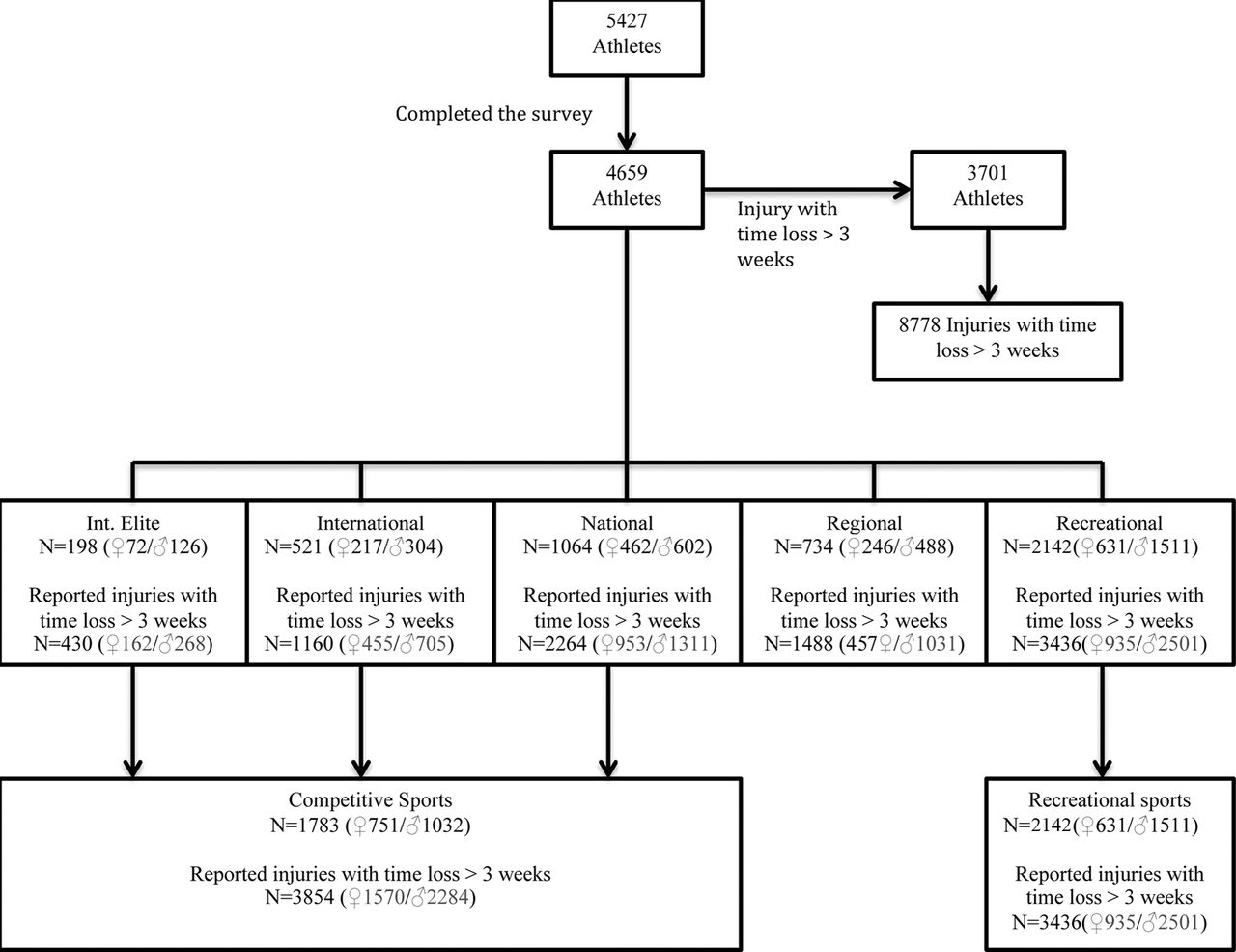
Flow chart of the included athletes, separated by performance level and number of injuries with a time loss of >3 weeks.
Study population number, percentage and weight category of all athletes, categorised by performance class
The mean age of the athletes when injuries occurred was 21.8±8.6 years (female 19.2±6.7; male 23.3±9.1); at the time of completing the survey it was 27.6±11.5 (female 24.6±8.9; male 29.7±12.3).
Statistical analysis
Statistical analysis was performed using the SPSS 22.0 software package (SPSS, Inc, Chicago, Illinois, USA).
To illustrate the most common injury types, specific injuries types are presented in absolute numbers and as percentages for all athletes, separated by gender and performance level. Each athlete’s age at the time of the injury was compared according to gender using Student’s t test. To assess differences between genders and sports categories (competitive vs recreational), risk relationships were analysed using χ2 and the OR. The OR was computed for each risk factor, and 95% confidence intervals (CIs) were constructed.
The intervals for time loss and reduction in sporting performance level after returning to sports for the specific injury types are presented as percentages. Differences for these intervals between genders and sports categories (competitive vs recreational) were analysed using the Mann–Whitney U test. A two-tailed p<0.05 was considered statistically significant.
Results
Overall, the 4659 included athletes reported 8778 injuries (female n=2962, male n=5816). A proportion of 79% (n=3701) of all athletes reported one or more injuries with a time loss of >3 weeks, according to the definition of injury. On average, each athlete had had 1.9±1.6 (female 1.8±1.5, male 1.9±1.6) injuries leading to >3 weeks’ absence from sport. Athletes who performed judo at a competitive level reported a mean of 2.1±1.6 injuries, while those at the recreational level reported 1.6±1.3 injuries.
Across all performance levels, the most commonly injured body regions were the upper (41%) and lower (39%) extremities, specifically shoulder (23%) and knee (23%) injuries. Furthermore, 5% of the judo athletes reported head injuries, 8% reported spine/back and pelvis injuries and 8% reported injuries to the thorax and abdomen.
Frequently specified injuries
The most commonly detected injuries are shown in figure 2.

{kind=link}
{kind=link}
(A) Most common injuries of all participants. Injuries acknowledged by more than 4% of all athletes were included. (B) The most common injuries for male and female participants. AC, anterior cruciate; ACL, anterior cruciate ligament.
Mean ages of the athletes at the time of the injury
Head, spine, upper body and trunk
With respect to the athletes’ ages at time of their injuries, no statistical differences were found for concussions (18.5±7.2 vs 17.3±5.5 years, p=0.14), rib fractures (25.5±9.5 vs 20.3±8.9 years, p=0.1) or vertebral disc prolapse (25.5±9.5 vs 21.4±7.1 years, p=0.1).
Upper extremity
The mean age of the athletes on occurring an injury was significantly lower among women than men for AC joint dislocations (24.1±8.4 vs 20.4±6.3 years, p<0.01), clavicle fractures (17.6±5.9 vs 16.2±4.9 years, p=0.04) and ligament injuries to the elbow (20.9±8.0 vs 17.5±5.0 years, p<0.01).
No statistical differences between the genders were found for the proportion of shoulder dislocations (21.6±7.3vs18.9±5.0, p=0.26) and unspecified shoulder injuries (23.4±9.0 vs 21.2±8.0 years, p=0.22).
Lower extremity
A lower mean age for women was detected for unspecific knee injuries (24.0±10.0 vs 19.3±6.0 years, p<0.01), ACL ruptures (24.0±10.0 vs 19.3±6.0 years, p<0.01), foot and ankle ligament injuries (24.0±10.0 vs 19.3±6.0 years, p<0.01) and meniscus injuries (24.0±10.0 vs 19.3±6.0 years, p<0.01).
Gender comparison
Compared with their female counterparts, male athletes had lower injury rates for concussions, clavicle fractures, ligamentous elbow injuries, ACL ruptures and foot, ankle and ligament injuries. Male athletes also reported significantly higher injury rates than female subjects for rib fractures and AC joint dislocations. No significant gender differences were found for vertebral disc prolapse, unspecified shoulder injuries, shoulder dislocations, unspecified knee injuries or meniscus injuries (table 2).
Injury risk depending on gender and performance class
Competitive versus recreational sports
Compared with recreational-level athletes, significantly more athletes who practised judo at a competitive level reported one or more injuries with a time loss of >3 weeks (competitive sports 82%, n=1470; recreational sports 76%, n=1619) (p<0.01; OR=1.52; 95% CI 1.3 to 1.8).
With respect to level of sports performance in competitive versus recreational sports, significantly higher injury rates were reported for vertebral disc prolapse, AC joint dislocation, shoulder dislocation, ligament elbow injuries, ACL ruptures and meniscus injuries. No statistically significant differences in injury rates between competitive and recreational sports were reported for concussions, rib fractures, unspecified knee injuries, ligament injuries or ankle or foot injuries (table 2).
Duration of sporting time loss after the most common injuries
Across all performance classes, the greatest number of athletes reported that they lost >3 weeks after an ACL rupture. The second most commonly stated reason was a vertebral disc prolapse. After an ACL rupture, 64% of the athletes reported a time loss of >6 months, 32% reported a time loss of >9 months and 14% reported a time loss of >12 months. Furthermore, a high percentage of athletes reported a long time loss after a vertebral disc prolapse, with 23% reporting a time loss of >6 months and 13% reporting a time loss of >12 months.
After a shoulder dislocation, 20% of the athletes reported a time loss >6 months. After an unspecified knee injury, an AC joint dislocation, an unspecified shoulder injury, a clavicle fracture and a meniscus injury, nearly 90% of the athletes returned to sports within 6 months. Of the athletes who reported a ligament injury to the foot or ankle, a rib fracture, a concussion or a ligament injury to the elbow, nearly 90% returned to sports after 3 months (table 3).
Duration of time loss athletes needed to return to sports after the most commonly reported injuries
There were no significant differences between male and female participants in the duration of time loss. For performance level, time loss after an AC joint dislocation was significantly longer in recreational than in competitive sports (p=0.02)
Reduction of sporting performance
Across all performance classes, athletes with ACL ruptures were the least likely to return to their pre-injury sporting performance level (32%). Furthermore, athletes with ACL ruptures were also the most likely to report a significantly reduced sporting level (24%). Following an ACL rupture, 5% of the participants reported stopping judo. Athletes who had had a vertebral disc prolapse were most likely to stop practising judo after injury (8%).
Nearly 85% of athletes with a self-reported shoulder dislocation or a meniscus injury returned to the same or a slightly reduced sporting performance level. Following a concussion, a rib fracture, an AC joint dislocation, an unspecific shoulder injury, a clavicle fracture, a ligament injury to the elbow, an unspecific knee injury or a ligament injury to the foot or ankle, approximately 90% of athletes returned to the same or a slightly reduced performance level (table 4).
Reduction in sporting performance level on return to sports following the most common reported injuries
Sporting performance level was significantly lower among female athletes than male athletes following an AC joint dislocation (p=0.01) or a vertebral disc prolapse (p=0.01). For recreational sports, significantly lower sporting levels were reported after ACL ruptures (p=0.04), AC joint dislocations (p=0.01) and unspecified shoulder injuries (p=0.03).
Discussion
Major findings
To our knowledge, this is the largest dataset of elite, national, international and recreational judo athletes analysing the injury-specific duration of time loss and the reduction in sporting performance level.
Among common judo injuries, an ACL rupture was the most serious injury with the longest time loss and markedly reduced performance following the return to sports. The second most serious injury was a vertebral disc prolapse.
Affected body location
In this study, the most affected body sites were the upper and lower extremities, especially the shoulders and the knees. In a prospective study of elite Korean judo athletes, Kim et al found a similar pattern, with 32% of injuries to the upper and 39% to the lower extremity.22 Their finding of a higher proportion of injuries to the lower extremity might be due to differing definitions of injuries. Kim et al classified injuries with 1–3 treatment days as grade 1, injuries with 5–7 treatment days as grade 2 and injuries with >8 treatment days as grade 3. Furthermore, Kim et al studied a smaller number of athletes. In a systematic review of the literature on judo injuries that did not consider performance levels, Pocecco et al also specified the extremities as the most affected regions of the body, especially the knee (28% of cases), shoulder (22%) and the hand and finger (30%).19 In our study, hand and finger injuries were not found to be common. This may be because these injuries do not tend to result in a time loss of >3 weeks, which was defined as a relevant injury in our study.
Several studies have indicated that the knee is the most frequently injured region of the body in judo.2 23 24 However, most studies have not conducted a deeper exploration of knee injuries. The most common knee injuries of our population were ACL ruptures and meniscal tears; however, Majewski et al and Miyazaki et al found that medial collateral ligament injuries were the most common judo knee injuries.25 26 Beyond the differing definitions of injuries, these variations in results might be due to the retrospective study design of our study. In our study, the medial collateral ligament injury of the knee was typically not considered a serious injury, which might have led the affected athletes to conduct less detailed diagnostic examinations. Therefore, a significant number of medial collateral ligament injuries might have been considered unspecified knee injuries.
Male versus female
In our study, female athletes suffered injuries at a younger age than men. Ristolainen et al reported identical results for 5- to 35-year-old cross-country skiers, swimmers, long-distance runners and soccer players.27 However, their study used different sets of age category definitions, with judo athletes older than 19 for women and older than 21 for men being considered ‘senior’. Subsequently, in 2013, the International Judo Federation equalised the age categories.
Female athletes were more likely to sustain injuries to the lower extremity, and male athletes were more likely to sustain injuries to the upper body, owing to the higher rates of ACL injuries among women and the frequency of rib fractures among men. While the risk of ACL ruptures is generally higher among women, until now, no gender-specific data have been available for risks of rib fractures, AC joint dislocation, foot and ankle ligament injuries, clavicle fractures, concussions or ligament elbow injuries in contact sports. These findings indicate a gender-specific injury risk for specific injuries.
Judo athletes who participated in competitive sports had more injuries than those who practised recreationally. Our data also indicated that competitive players had more severe joint injuries. Our results are in line with the results of Krutsch et al for ACL and posterior cruciate ligament injuries and Abrams et al for musculoskeletal injuries in tennis.28 29 These findings indicate that injury risk is dependent more on the intensity of judo participation than on the sporting level.
Judo injuries with long time loss and significant reductions in sporting performance
ACL ruptures and vertebral disc prolapses were found to be the injuries with the most cases of long time loss and significant reductions in sporting performance.
ACL ruptures in judo
In our study, ACL ruptures were more common among female athletes and athletes who practised competitively. These results mirror findings for other sports, where ACL ruptures have been found to occur more commonly among women.30 31 Until now, this gender-specific risk has been explored primarily in the field of non-contact sports.32 The higher risk for female athletes in judo, a contact sport in which most ACL injuries result from contact, indicates that there is no great difference in injury mechanisms for contact and non-contact ACL injuries. Until now, no studies have produced gender-specific ACL injury rates for judo.33 The higher rate of ACL ruptures in competitive sports shows that the risk involved in sustaining a pivoting knee mechanism increases with the athlete’s sporting level, a finding that has also been observed in other competitive sports.34 Until now, no studies have identified the recovery time needed by judo athletes before returning to sports. Particularly at the competitive sports/elite level, long recovery times are disadvantageous for athletes’ sporting careers. Furthermore, athletes who categorised themselves as recreational sports participants reported significantly lower sporting performance levels following ACL ruptures than athletes who categorised themselves as competitive players. It is likely that the driving force to continue judo after a serious injury is lower among recreational athletes, who may focus more on their education or careers. Higher-level athletes may also have access to better clinical services.
ACL ruptures caused the greatest proportion of athletes to experience significantly reduced level sporting performance after returning to sports. Ardern et al found similar results for athletes from different kinds of ball sports, 61% of whom had attempted to return to their preinjury level.35 For judo athletes, it has been suggested that ACL rupture is the most serious knee injury.23 Until now, this suggestion has not been confirmed by the literature.2 19–22 36 37 Our study is the first to show that the ACL rupture is the most serious knee injury in judo, but also the most serious injury of all frequent judo injuries. Our data strongly suggest the importance of developing a prevention programme for judo similar to those that have been successfully introduced in other sports.8
Vertebral disc prolapse in judo
Another major finding of our study was that vertebral disc prolapse is the injury that causes the highest proportion of athletes to stop judo and the second highest proportion of athletes (after an ACL rupture) to require a recovery time of >12 months. Other studies have also reported injuries and overuse syndromes of the back. Kim et al reported that 17% of injuries dealt with the thoracic back/upper spine and the lumbar spine/lower back.22 Okada et al reported a prevalence of unspecific low back pain in 35% and radiologically abnormal findings in 82% of a group of Japanese college judo athletes. Of this same group of athletes, 56% had degenerative intervertebral disc degeneration.38 In other contact sports, the relevance of vertebral disc prolapse is known. Grey et al examined disc herniation in professional football players and found that the mean time loss from playing was 63 days (SD±74 days).39 Until now, the relevance of these findings to judo had not been identified.2 19–21 36
Limitations
One of the limitations of the retrospective data used in this study is that the injuries and their severities were self-reported. Gabbe et al observed that football players exhibited a recall bias 12 months after injury: they could recall their injury locations with high accuracy at that time, but only 61% could accurately recall their injury diagnosis.40 Although this limitation implies a potential for over- or under-reporting of specific diagnoses, the primary aim of our study was to present ratios of region-specific frequencies of sports injuries. Hence, rather than detecting specific incidences, our study sought to report injury proportions and injury-specific time losses and sporting performance reductions. Any recall bias would have affected all factors mentioned above in the same way.
The injury frequencies were not related to a defined period of time. For this reason, only injury proportions (and not injury rates) could be reported. Other epidemiological studies on judo injuries that have referenced periods of time loss have struggled to determine injury rates and have reported a wide range (25.2–148) of overall rates per 1000 athlete exposures.19 33 The best way to assess athletic exposures would be a prospective analysis. However, our study did not seek to compare judo injury rates with the rates of other sports; instead, it sought to perform a cross-sectional analysis of severe judo injuries. Therefore, this study may serve as a basis for further prospective research on athletic exposures and possible prevention strategies.
Conclusion
The upper and lower extremities, especially the knees and the shoulders, are the most injury-prone areas in judo. For most injuries, the absence from sports participation and the reduction in sporting performance level are low. The most serious injuries for judo athletes are ACL ruptures and vertebral disc prolapses, which cause lengthy time losses and significantly reduced sporting performance levels following the return to sports. Further research should focus on developing better treatment options and prevention strategies for these injuries.
What are the findings?
Anterior cruciate ligament ruptures and vertebral disc prolapses are the most serious judo injuries with the greatest time loss and the most significant reduction in sporting performance level.
How might it impact on clinical practice in the future?
Prevention programmes to deal with these injuries, as have been established in other sports, are necessary in judo. Further research should focus on developing appropriate programmes.
Acknowledgments
The authors also thank Youssef El Quadoudi and Rolf Lefering for supporting the statistical data analysis throughout this study and Rolf Lefering and Matthias Krause for reviewing the paper.
References
Footnotes
Contributors RA, CL and JH designed the study. RA and JH directed its implementation and wrote the paper. CL performed the data collection. MB, KHF and BB helped to design the study’s analytic strategy. KHF and MB reviewed the paper. All authors read and approved the final manuscript.
Funding The authors declare that they have no competing interests.
Funding The study was sponsored by the ARAG insurance company (Düsseldorf, Germany) and Verein zur Förderung der Forschung und Weiterbildung in der Sportraumatologie e.V. The study sponsors had no influence on the collection, analysis or interpretation of the data or on the decision to submit the work for publication.
Competing interests None declared.
Ethics approval Ethical committee of the Witten/Herdecke University (Application 96/213).
Provenance and peer review Not commissioned; externally peer reviewed.