Article Text

Abstract
Objective: To assess whether a rule change introduced in the Australian Football League (AFL) before the start of the 2005 season, to limit the run-up of ruckmen at the centre bounce, has been successful in reducing the incidence of knee posterior cruciate ligament (PCL) injuries
Design: Cohort study with historical control.
Setting: The AFL competition from 1992 to 2008 inclusive.
Assessment of risk factors: The presence of a rule change (four seasons) compared with the previous 13 seasons (divided into two eras of seven and six seasons).
Main outcome measure: Occurrence of knee PCL injury during a regular season or finals match, both from all causes and specifically from centre bounce ruck collision mechanisms.
Results: From 1992 to 1998 there were 11.0 PCL injuries per 10 000 player-hours, with 0.8 ruck injuries per 10 000 centre bounces. From 1999 to 2004, the rates increased to 12.9 per 10 000 player-hours and 5.6 ruck injuries per 10 000 centre bounces (p<0.01). The rates reduced to 5.9 PCL injuries per 10 000 player-hours and 0.9 ruck injuries per 10 000 centre bounces in the period 2005–2008 following the rule change (p<0.01). There was a lower relative risk in 2005–2008 than in 1999–2004 of incurring a centre bounce ruck PCL injury (0.16 (95% CI 0.04 to 0.69)) or of sustaining any PCL injury (0.45 (95% CI 0.28 to 0.75)).
Conclusion: A rule change in the AFL to limit the run-up of ruckmen at the centre bounce has successfully reduced the rate of PCL injuries with this mechanism, with the total incidence of PCL injuries also falling.
Statistics from Altmetric.com
Australian Football is a unique variety of football played mainly in Australia, with high rates of both contact and non-contact mechanism injuries. The game is played on larger size fields than other forms of football, and it combines strenuous running with ball-handling and player-to-player contact. In terms of physiological demands, the code is similar to soccer, with repetitive kicking and running efforts. However, it differs from soccer in the type of body contact. Tackling around the body is allowed, but not to the legs, although incidental leg-lo-leg contact does occur. Games are played over four quarters lasting 20 min each, plus time added for breaks in play. The Australian Football League (AFL) is the top level professional competition of Australian football, with a previously published injury profile.1 Since 1995 it has administered a fixed single-grade competition with 16 teams participating in a regular season of 22 rounds. There are 18 players on the field from each team in an AFL match, with four players on an unlimited interchange bench (which was increased from three in 1998).
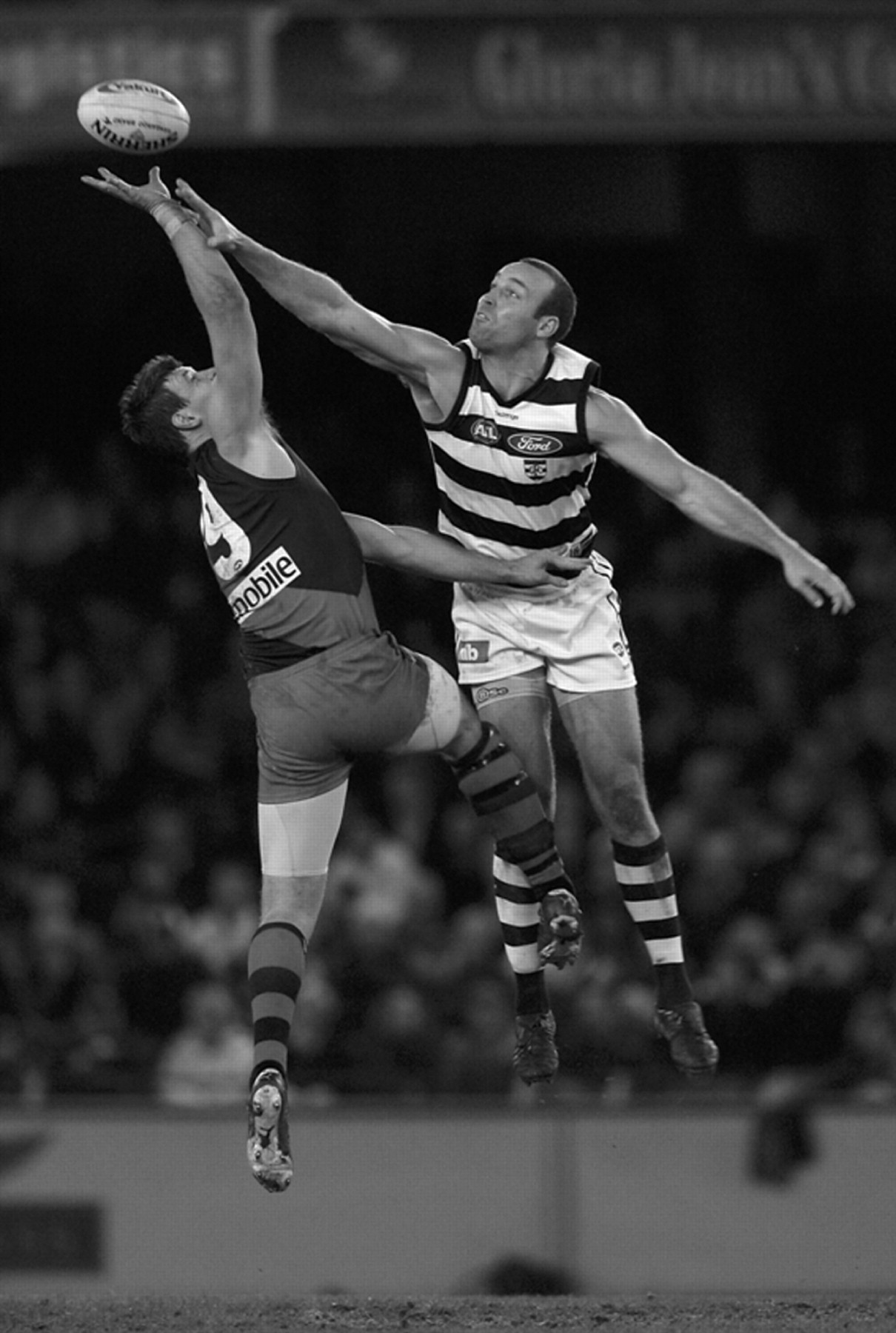
In Australian Football, play is started at the beginning of each quarter, or after a goal is scored, with a centre bounce contest. There are 30 centre bounce contests per match, on average. The umpire bounces the ball so it rises 5–8 m in the air. The two opposing ruckmen run from opposite directions and jump towards each other, competing to knock the ball to the ground or to their team mates (fig 1). The ruckmen are generally the tallest members of the team. Ruckmen also compete against each other in restarts of the game when the ball has gone out of play (boundary throw-in) or when a player has the ball trapped in possession with no opportunity to legally dispose of it (ball-up). The nature of the ruck duel is different in these situations from the centre bounce duel. At a ball-up, the ball is thrown up to a lower height and the ruckmen often wrestle, as there is less time to take a run-up. At a boundary throw-in, the ruckmen are standing side by side, both facing the oncoming ball, rather than running at each other from opposite directions.
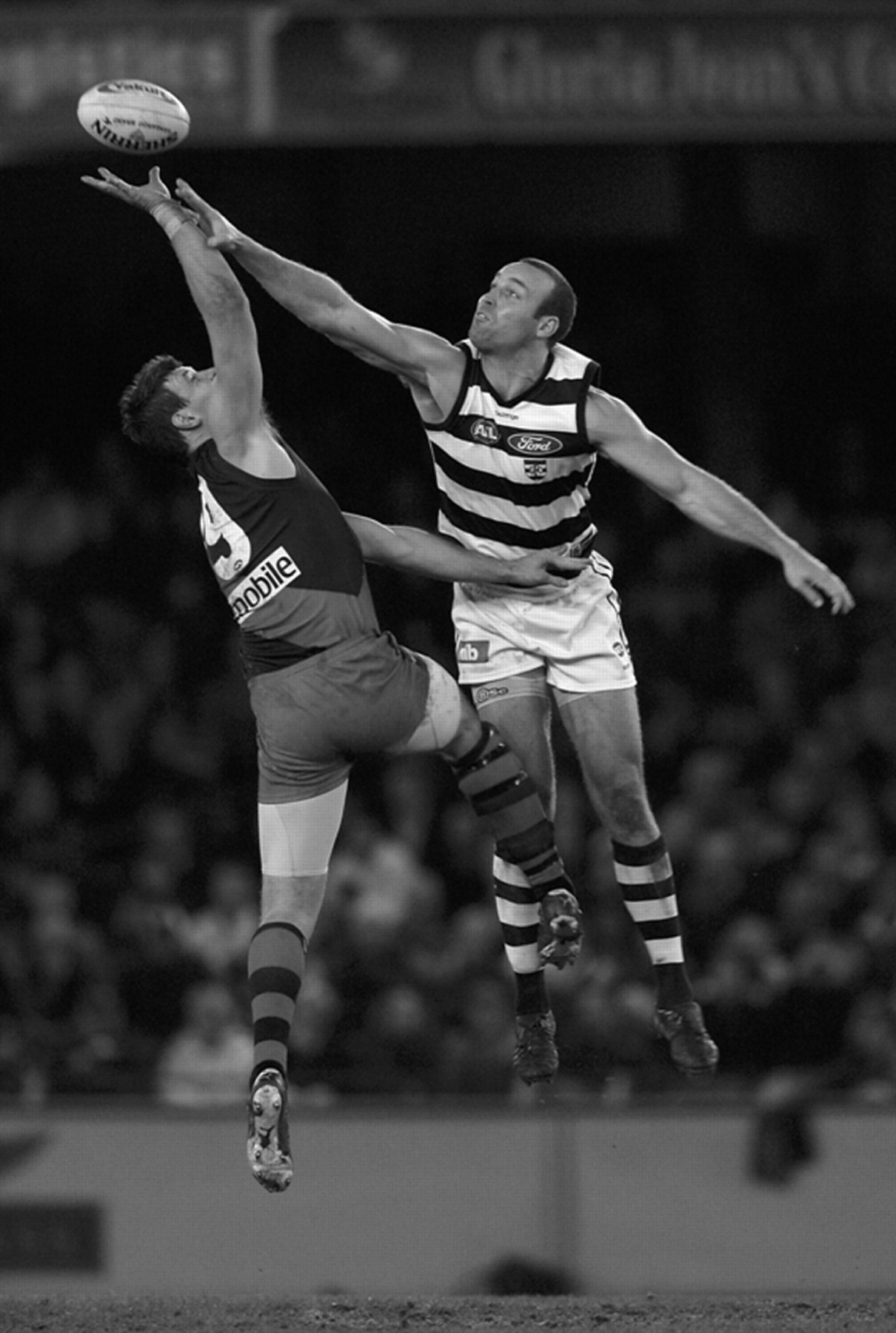
Typical ruck duel at the centre bounce in Australian Football. Note the potential for leg–knee contact (although injury susceptibility depends on the force of contact). No injury occurred in the ruck duel presented.
Since 1992, the AFL has conducted and published an annual injury survey every season.1 2 3 4 5 Injury surveillance is now widely considered to be an important obligation of professional sporting bodies.6 7 8 9 One of the major functions of an injury surveillance system conducted over a long period of time is to identify changing trends in injury incidence. In 2004, the AFL injury survey was able to identify and document an increase in knee posterior cruciate ligament (PCL) injuries over the previous 6 years compared with the preceding 7 years, involving a mechanism of contact between ruckmen at the centre bounce (video 1, supplemental file online).2 Further research was undertaken to identify the reasons for this increase. Findings highlighted risk factors and recommended possible rule changes to prevent further injury. At the start of the 2005 season, a rule change was introduced to limit the force of collision between ruckmen at the centre bounce by limiting, with a circle, the distance of their run-up (fig 2).

{kind=link}
{kind=link}
Centre bounce with 10 m outer circle (the limited distance for run-up lowers the speed at which the ruckmen can approach each other).
The objectives of this study are (1) to document the frequency and incidence of PCL injuries in the AFL, both before and after the 2005 rule change, and (2) to discuss the process and rationale for the rule change and comment on its consequences.
Methods
AFL injury survey
The methods of the injury survey are now well established and have been previously described in detail.1 2 3 4 The definition of an injury for the survey is “any injury or other medical condition that prevents a player from participating in a regular season (home and away) or finals match”. All 16 teams provide contemporaneous recording of player status (for all contracted players) for each match (playing at either AFL or lower level; not playing because of injury; not playing for other reasons). The details of injuries that result in a status of being unable to participate in a match because of injury are then passed on to the injury surveillance coordinator at the end of the season for recording and analysis. These details include diagnosis, which is subsequently coded,10 11 and mechanism of injury. This definition and methodology has been chosen to promote consistency across the 16 AFL clubs and from season to season.12 This definition has allowed the injury survey to achieve “100% compliance” for all instances of missed player games since 1997,1 and therefore it can be argued that this survey is one of the most reliable sports injury surveillance systems in the world.12 It has been argued that this definition excludes valid injuries that do not cause a player to miss a match.13 However, for a longitudinal study such as the current analysis, if a broader definition was used, there may be a concern about changing thresholds for reporting an injury by team medical staff over time.12
The survey database allows deidentified player injury data to be extracted from the database for further analysis. The methods used for this study were non-interventional and conform to the Code of Ethics of the World Medical Association (Declaration of Helsinki) and Australia’s National Health and Medical Research Council (NHMRC) guidelines. They were approved by the AFL Research Board, which is the relevant institutional review board for this type of study.
Injury definition
For the purposes of calculating reliable match incidence rates, the injury definition for this study was “all instances of reported PCL injuries which occurred during a regular season or finals match (of any grade) that prevented a player from participating in a later regular season or finals match”. This excluded PCL injuries that occurred during training, pre-season, intra-club (non-scheduled) matches or outside football and those that did not cause a game to be missed. Recurrent injuries (exacerbations of a past PCL injury) were included as part of this study.
Injuries were extracted from the database in a deidentified manner, with the details extracted being diagnosis, mechanism (centre bounce ruck duel versus other), onset (match or other) and date (season).
Incidence rates
The number of matches played by players under survey each season was also extracted from the database. Each player’s last match of the season (whether this was a regular season or finals match) was excluded from the analysis, as injuries occurring during this match generally could not satisfy the survey definition of missing a further match.
Match incidence rates per 10 000 player-hours were calculated. Incidence rates were calculated for all PCL injuries, those injuries that occurred with a mechanism of ruck contact at the centre bounce, and those without this mechanism (most commonly landing directly on the ground with a flexed knee).
The number of centre bounces per game under survey was estimated as being four per match (for the start of each quarter) plus the number of goals scored in each game. This is an estimate only, as match footage was not viewed. The estimate is likely to be a fairly accurate one, probably within 2–3% of the “true” number of centre bounces. There are rare occasions when the number of centre bounces would differ from this formula (eg, if a goal is scored as the last play of a quarter or match or if the centre bounce is repeated because of an “unfair” bounce). These occasions could be determined only by studying video footage of every game. Because the number of centre bounces was estimated (albeit fairly accurately), the incidence rate of PCL injuries per 10 000 centre bounces is presented to one decimal place only.
Statistical analysis
The period of survey was from 1992 (the start of AFL injury surveillance5) to 2008. The 16 seasons were subdivided into three eras. The last era was clearly defined as 2005–2008 inclusive, which was the period under the new ruck rule. The previous years were divided into the eras of 1992–1998 and 1999–2004 inclusive. The decision to divide the earlier seasons into two eras was made because it was clear that the incidence of ruck mechanism PCL injuries started to increase in the 1999 season.
The injury rates between eras were statistically assessed with χ2 tests using the Yates correction with a p value of <0.05 chosen to represent significance. Confidence intervals to calculate relative risk were calculated with Taylor series expansions.
Results
From the 17 seasons from 1992 to 2008 inclusive, data from 4092 players were imported in a deidentified fashion. In a typical season there were 16 teams playing 22 rounds of matches in the regular season, with eight teams playing four rounds of finals. Tables 1 and 2 summarise the incidence of PCL injuries from the various mechanisms on an annual basis (table 1) and when grouped by eras (table 2).
Posterior cruciate ligament (PCL) injury frequency and incidence
Comparison of eras
Changes occurring from season 1999
During the period 1999–2004, there was a significant increase in the incidence of ruck duel mechanism PCL injuries in the AFL compared with the previous period of 1992–1998 (χ2 = 11.2, p<0.01). This was quite a rare mechanism of injury in 1992–1998, but became relatively more common in the following six seasons. Trends were also noticed that ruckmen had, from the late 1990s, started to take longer and longer run-ups at the centre bounce and were lifting their knees more in the ruck contest.
The overall incidence of PCL injuries between these two eras did not significantly change (χ2 = 0.7, p = 0.40), registering only a slight increase. This appears to have been because ruck duel mechanism PCL injuries (despite the increase) only made up a minority of total PCL injuries and PCL injuries due to other mechanisms fell slightly over the same time period.
Rationale behind the rule change
A number of processes were followed to investigate the factors that may have led to the increase in ruck-related PCL injuries and to define the risk factors. Focus group discussions and expert interviews with coaches, players, administrators and media commentators were undertaken. Video footage of centre bounce ruck contests over 20 years was analysed.
The major possible contributing factors identified were:
Increasing length of run-up and subsequent momentum of impact.
Increasing use of a raised knee that strikes the opponent.
Increasing tendency for direct front-on collisions between ruckmen.
Slightly increased height of ball bounce.
Increasing use of ruck coaches training ruckmen to use their knee as a lever and aiming to disrupt their opponent.
During the period 1999–2004, it appears that there had been an administrative change in coaching through the competition where clubs had appointed specialist ruck coaches. This increased focus on technique and performance was thought to have contributed to some of the changes.
Several rule changes were considered including:
Limiting the length of the run-up using a 10 m circle, with ruckmen to start their run-up from within the circle.
Outlawing the raised knee at contact.
Eliminating the centre bounce and replacing with a ball-up.
Attempting to train umpires to reduce the height of the ball bounce.
Outlawing all but inadvertent contact when the ball is in reach.
Current rule interpretation and umpire positioning were also reviewed, to more aggressively penalise ruckmen who do not keep their eyes on the ball and thus collide with their opponent.
Coaches and administrators were given the opportunity to comment, and then the AFL Rules Committee determined that the first option would be the preferred rule change. This change was the simplest to introduce without significantly altering the popular gladiatorial jumping character of this particular contest.
Changes occurring from season 2005
After the new rule change, from the 2005–2008 period the incidence of PCL injury from ruck duel mechanisms fell dramatically, when calculated both in terms of injuries per 10 000 player-hours (χ2 = 6.9, p<0.01) and injuries per 10 000 centre bounces (χ2 = 6.7, p<0.01). There have only been two ruck duel mechanism PCL injuries in AFL matches during this subsequent 4-year period, and one injury was a recurrence of a past PCL injury, suggesting that previous trauma was a predisposing factor. Of further interest is that both PCL injuries as a whole (χ2 = 9.4, p<0.01) and PCL injuries from other mechanisms (χ2 = 3.7, p<0.06) fell over this time period. There was lower relative risk (RR) in 2005–2008 compared with 1999–2004 of incurring a centre bounce ruck duel PCL injury (RR 0.16 (95% CI 0.04 to 0.69)) or of sustaining any PCL injury (RR 0.45 (95% CI 0.28 to 0.75)).
Discussion
This paper describes an example of van Mechelen et al’s7 often quoted process of generating a safer sporting environment through (1) injury surveillance, (2) identification of risk factors, (3) risk factor intervention and (4) further monitoring to identify improvement. It incorporates Finch’s TRIPP paradigm6 in that the AFL injury survey and injury rates are discussed on a regular basis in the Australian media, which increased the perceived need for a timely rule change once the trend for increased PCL injuries in centre bounce ruck contests became apparent. The use of rule changes to reduce mechanisms of susceptibility to injury has previously been described by Bahr and others.14 15 Rule changes have previously been used, for example, to lower the rate of catastrophic head injury in American football with the outlawing of spear tackling16 and in rugby union to try to reduce injuries related to scrummaging.17
The long-term nature of the AFL injury survey, with its reliable data collection identifying gradual trends, avoids the potential risk of attempting to introduce changes prematurely with only short-term information. It demonstrates that an injury surveillance system serves as an identification tool requiring further specific research to establish confirmatory data and identification of risk factors. It also shows the benefit of involving experts and focus groups to supplement data collection, to produce a sport-specific, relevant and acceptable intervention. It further illustrates that providing administrators with a variety of interventions allows them to choose the optimal intervention, when they have to consider many facets of the game that may conflict with their choice. They have to manage the subsequent intervention, particularly a rule change, and answer any criticism during the implementation phase as coaches and players adapt to the change. When the ongoing surveillance proves the benefit of the intervention, it is then rewarding for all involved, particularly the players who avoid injury.
The most common cause of PCL injury remains the considerable backward force transmitted to the tibia when a player lands on the ground on his knee. The second most common cause is the upper tibia striking a part of the opponent, usually the knee or hip, producing a posterior force in a jumping context, either when marking or in the centre bounce ruck contest. The injury is usually a single incident, but we suspect that repeated minor trauma can predispose the ligament to a rupture incident. This particular study does not have the scope to determine whether the decrease in non-ruck mechanism PCL injuries was due to: (1) reduced trauma from ruck collisions leading to lower susceptibility of ruckmen’s PCLs to trauma from other causes; (2) decreases in ground hardness,18 which may have reduced the risk from landing directly on a flexed knee; or (3) a combination of these, chance and other confounders.
The rate of centre bounce ruck mechanism injuries basically returned, in seasons 2005–2008, to the rate observed before 1999. Pleasingly, the overall rate of PCL injuries has fallen since 2005 compared with both previous time periods studied (1999–2004 and 1992–1998).
Since 1992, the AFL injury survey has provided reliable injury surveillance data in one of Australia’s most popular sports. In 2004, it was able to demonstrate that, over the preceding 7 years, a particular type of contest during the game—the centre bounce ruck contest—was causing a high rate of PCL injuries. Further investigation resulted in the implementation of a rule change to reduce the injury risk. Subsequent injury surveillance shows that this particular injury mechanism has been almost eliminated from the game.
What is already known on this topic
Posterior cruciate ligament injuries in sport most commonly occur with a mechanism of a player falling to the ground on a flexed knee.
What this study adds
Posterior cruciate ligament (PCL) injuries can also occur from player-to-player collision in mid-air.
This mechanism is unlikely to result in sufficient force to injure the PCL if the collision is at low speed, but is much more likely at high speed.
Therefore the rule change in Australian football to limit the speed at which ruckmen can approach each other has successfully lowered the risk of PCL injury.
Acknowledgments
We acknowledge the medical officers and physiotherapists who provided data for the AFL injury survey and the AFL football administration for both supporting the injury survey and for implementing the rule change. Sean Garnsworthy and Geoff Slattery are acknowledged for providing the photograph used in fig 1, for which they have provided permission. (The photograph in fig 2 was taken by the first author.) Adam Goodes (Sydney Swans player) and Nathan Gibbs (Sydney Swans doctor) are acknowledged for allowing use of the video illustrating the mechanism of a ruck-related PCL injury before the introduction of the centre-circle rule. Andrew Morris (medical student) is acknowledged for helping to provide a report on the issue to the AFL football administration in 2004.
REFERENCES
Footnotes
▸ A video can be accessed online only at http://bjsm.bmj.com/content/vol43/issue13
Funding The AFL conducts and funds an annual ongoing injury survey recording injuries for all players. JO is a contractor for the AFL in this role. There were no other funding sources.
Competing interests The AFL conducts and funds an annual ongoing injury survey recording injuries for all players. JO is a contractor for the AFL in this role. There were no other competing interests.
Ethics approval Obtained from the AFL Research Board.
Patient consent Obtained.
Provenance and Peer review Not commissioned; externally peer reviewed.